© Copyright
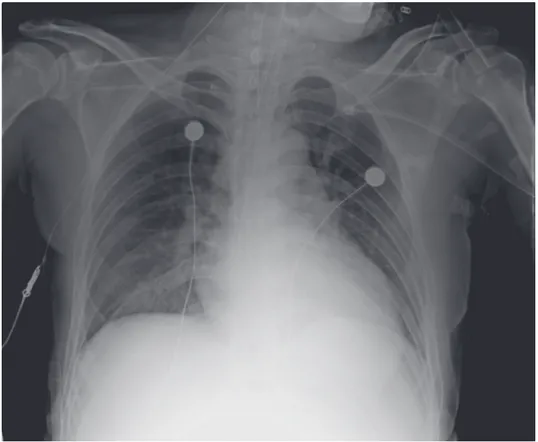
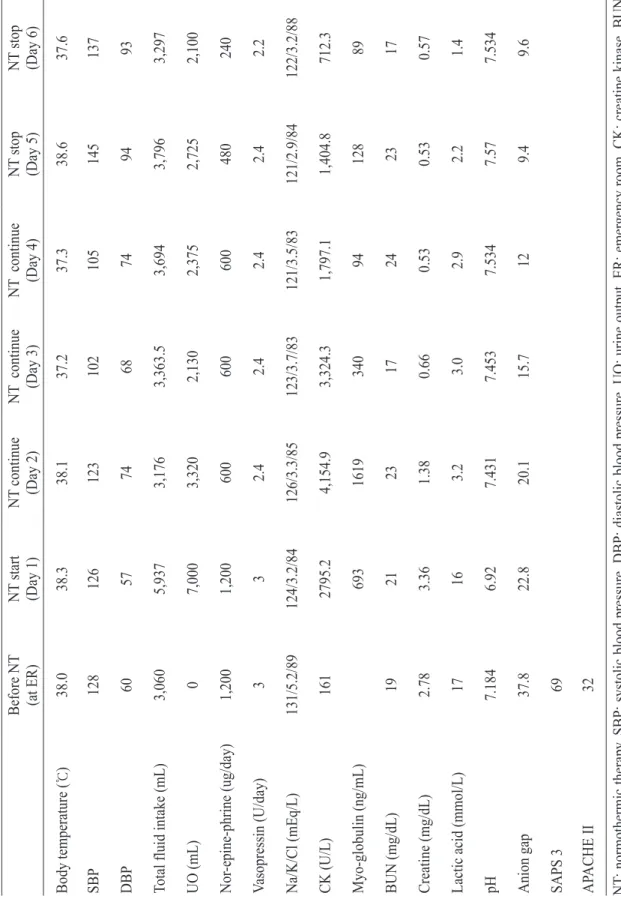
Rhabdomyolysis with Acute Kidney Injury Successfully Treated with External Cooling
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치
관련 문서
mould with rapid and uniform cooling characteristics using the deposition of the multi-materials based on the direct metal rapid tooling process.. In order
S., An Experimental Study on the Cooling and Heating Performance of a Residential Ground Source Heat Pump System, Korean Journal of Air-Conditioning
Null hypotheses of this study was there is no difference in root canal length determination between conventional and heat-treated Ni-Ti files by 2
We evaluated the general characteristics, mechanism of injury, Revised Trauma Score(RTS), Injury Severity Score(ISS), Trauma Injury Severity Score(TRISS). More men
• To compare this neural activity with MI of a human with spinal cord injury, MN performed a step tracking, ‘center-out’ task using the neural
In the present study we investigated the proliferation effect of human oral cancer KB cell treated with pulsatilla koreana extract.. We analyzed the effects of this
We evaluated the general characteristics : mechanism of injury, vital sign, Revised Trauma Score(RTS), Injury Severity Score(ISS), Hemoglobin Value which
Glucose level before use of mannitol and peak osmolarity during mannitol treatment were associated with renal failure in univariate analysis.. In logistic regression
