Case Report
원고 접수일 2010년 10월 14일, 게재 확정일 2011년 1월 2일 책임저자 남정훈
(150-950) 서울시 영등포구 대림1동 948-1, 한림대학교 의과대학 강남성심병원 치과/구강외과학교실
Tel: 02-829-5233, Fax: 02-846-9789, E-mail: [email protected]
RECEIVED October 14, 2010, ACCEPTED January 2, 2011 Correspondence to Jeong-Hun Nam
Department of Oral and Maxillofacial Surgery, Kangnam Sacred Heart Hospital, College of Medicine, Hallym University
948-1, Daerim 1-dong, Yeongdeungpo-gu, Seoul 150-950, Korea Tel: 82-2-829-5233, Fax: 82-2-846-9789, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
함치성 낭종의 조대술 후 미맹출 변위 영구치의 교정적 정출: 증례보고
남정훈1,3ㆍ노경록1ㆍ유우근1ㆍ이병민1ㆍ전지현1ㆍ박수현1ㆍ안장훈1ㆍ김정희2
1한림대학교 의과대학 강남성심병원 구강악안면외과학교실, 2한림대학교 임상치의학대학원 치과병원,
3스타28치과그룹 일산센터 치과임플란트과
Abstract
Forced Eruption of Severe Angulated and Impacted Permanent Teeth after Marsupialization of Dentigerous Cyst: Case Report
Jeong-Hun Nam 1,3 , Kyung-Lok Noh 1 , Woo-Geun Yoo 1 , Byeong-Min Lee 1 , Ji-Hyeon Jeon 1 , Su-Hyun Park 1 , Jang-Hoon Ahn 1 , Jung-Hee Kim 2
1
Department of Oral and Maxillofacial Surgery, Kangnam Sacred Heart Hospital, College of Medicine,
2
Dental Hospital, Graduate School of Clinical Dentistry, Hallym University,
3
Department of Dental Implantology, Ilsan Center, STAR 28 Dental Group
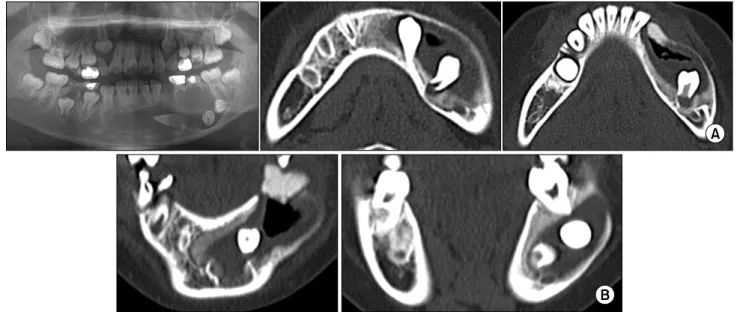
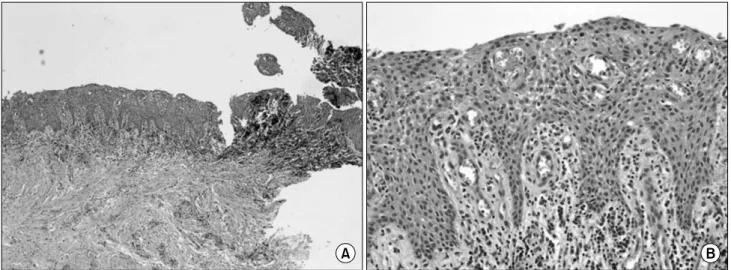
The goal of this treatment is the surgical-orthodontic eruption of impacted permanent teeth associated with a large dentigerous cyst in a preadolescent patient. Although enucleation of the entire cyst and the extraction of impacted teeth are common treatments, missing permanent teeth cause several problems in young patients. In this report, an 11-year-old female visited with the chief complaint of a large radiolucent lesion from the mandibular anterior area to the left mandibular posterior area. The permanent left canine and premolars were displaced toward the mandibular inferior border area. The extraction of infected deciduous teeth and marsupialization were performed. After 4 months, orthodontic buttons for forced eruption were applied to the impacted permanent teeth. The teeth emerged into the oral cavity 3 months after the orthodontic treatment.
Although the root form was abnormal, there were no other pathogenic signs. The alveolar bone had a normal trabecular pattern and the teeth appeared to be well maintained at postoperative 24 months.
Key words: Forced eruption, Marsupialization, Dentigerous cyst