혼합 용매에 따른 보툴리눔 A형 독소의 역가 차이
서울대학교 의과대학 재활의학교실, 분당서울대학교병원 재활의학과 서울대학교 의과대학 피부과학교실�, 모델로피부과��
서구일��∙오민균∙은희철�∙백남종
– Abstract –
The Potency Difference of Botulinum Toxin Type A according to Reconstituting Media
Kyle Seo, M.D., Ph.D.**, Min-Kyun Oh, M.D., Hee Chul Eun, M.D., Ph.D.*, Nam-Jong Paik, M.D., Ph.D.
Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National University Bundang Hospital
Department of Dermatoloty, Seoul National University College of Medicine, Seoul National University Hospital*, Botulinum Institute and Modelo Dermatology and Laser Clinic**
Objectives: The purpose of this study is to compare the potency of botulinum toxin type A (BTA) recon- stituted with preserved saline to that with nonpreserved saline in humans.
Methods: We conducted double blinded controlled study of injecting BTA reconstituted with normal saline to one side of extensor digitorum brevis (EDB) and BTA reconstituted with preserved saline to the other side of EDB in 11 healthy volunteers.
Amplitude of the EDB compound muscle action potentials (CMAP) was compared between both sides before and 1 week, 4 weeks, 8 weeks and 12 weeks after the injection.
Results: At 1 week after the injection, there was no difference in potency between two sides. However, there was a significant potency difference at 4 weeks, 8 weeks and 12 weeks after the injection, showing reduced potency of BTA reconstituted with preserved saline compared to BTA reconstituted with normal saline.
Conclusion: Potency of the BTA might be reduced when it is reconstituted with preserved saline as com- pared to normal saline, therefore reconstituting BTA with preserved saline should be reconsidered.
Key Words: Botulinum toxin type A, Potency, Reconstitution
Address reprint requests to Nam-Jong Paik, M.D. Ph.D.
Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul National University Bundang Hospital
#166 Gumi-Ro, Bundang-gu, Seongnam-si, 463-707, South Korea TEL : 82-31-787-7731, FAX : 82-31-787-4056, E-mail : njpaik@snu.ac.kr 투고일 2008년 6월 11일, 게재확정일: 2008년 8월 1일
서 론
보툴리눔 독소는 clostridium botulinum에 의해 생 성된 단백질로 말초 신경의 콜린성 시냅스에 작용하여 아세틸콜린의 분비를 억제하여 근육의 일시적인 마비를 일으킨다.1 이런 특성을 이용하여 사시(strabismus) 치
료방법으로 보툴리눔 독소가 처음 소개된 이후2 그 적용 범위가 점차 넓어져 현재에는 근긴장이상증(dysto- nia), 안면경련, 안검경련, 연축성 사경(spasmodic torticollis), 사시 등 다양한 질환의 치료에 이용되고 있으며,3,4 최근에는 주름살과 다한증의 치료에도 사용되 는 등 그 적용범위가 확대되고 있다.
현재 시판되고 있는 보툴리눔 독소 중의 하나인 보톡 스(Botox�, Allergan, Inc, Irvine, CA, USA)의 제품사용 설명서에 따르면 역가가 시간이 경과함에 따 라 감소하기 때문에 생리 식염수와 혼합 후 4시간 이내 에 사용할 것을 권유하고 있다. 그러나, 임상적으로는 약값이 고가인데다 소아 환자, 주름살치료, 연축성 발 성장애(spasmodic dysphonia) 등과 같이 한 바이알 (vial) 이하의 작은 용량의 주사만 필요한 경우에는 환 자를 모아서 주사하여야 하지만 여의치 않은 경우가 많 아, 일부 연구자들은 제조회사의 권고에 반하여 냉장보 관을 오래 지속하겠다는 바램 하에 0.9% benzyl alcohol을 포함한 보존 생리식염수 (preserved saline)에 보툴리눔 독소를 섞어 사용하는 경우가 있 다.5-7
따라서 본 연구는 정상 성인들을 대상으로 한쪽 단지 신근(extensor digitorum brevis)에는 혼합용매로 일 반 생리식염수를 사용한 보툴리눔 독소를 근주하고 반 대편에는 보존 생리식염수를 혼합한 보툴리눔 독소를 주사하여 양쪽 근육 마비율을 복합근활동전위를 이용하 여 비교하여 보툴리눔 독소의 혼합용매에 따른 근육 마 비 역가의 차이를 알아보고자 하였다.
연구대상 및 방법
1. 연구 대상
본 연구는 전향적, 군내 대조군, 이중맹검법으로 시 행되었으며 신경학적 검진을 통하여 중추신경과 말초신 경계 이상이 없고 단지신근을 포함한 근골격계 손상이 나 이상이 없는 정상 성인 남녀 11명을 대상으로 하였 으며 연구 전 2주와 연구 중에는 약물 복용은 금지 하 였다.
피험자 중 임신 중이거나 수유 중인 사람, 신경근 질 환을 앓고 있거나 과거에 앓은 사람, 보툴리눔 독소에 대한 과민증의 기왕력이 있는 사람, 급성 질환을 앓고 있는 경우는 대상에서 제외하였다. 대상자의 연령분포 는 25세에서 35세로 평균연령은 28.18±3.79세였고, 성별분포는 남자 5명, 여자 6명 이었다. 본 연구의 프 로토콜은 임상심의 윤리위원회의 승인을 받았으며, 모 든 임상 시험 참여자에 대하여 서면 동의를 취득하였다.
2. 연구 방법
1) 보톨리눔 독소의 희석 방법
보톡스�는 vial간에 약 30%의 역가 차이가 있을 수 있어8 역가의 차이를 배제하기 위하여 다음과 같은 방법 으로 일반 생리식염수군과 보존 생리식염수군의 용액을
준비하였다. 우선 보톡스� 100 unit(1 vial)을 일반 생 리식염수 1cc로 희석하여 100 unit/1 cc가 되도록 조 제한 후, 그 중 0.5 cc는 용기에서 뺀 후 다른 용기에 담고 일반 생리식염수 1.5 cc를 추가하여 일반생리식염 수 2 cc당 50 unit, 즉 2.5 unit/0.1 cc가 되도록 일 반 생리식염수군을 조제하였으며, 남아있는 0.5 cc에는 보존 생리식염수 1.5 cc를 추가로 넣어주어 75% 보존 생리식염수 2 cc(일반생리식염수 0.5 cc+보존생리식염 수 1.5 cc)당 50 unit, 즉 2.5 unit/0.1 cc가 되도록 보존 생리식염수군을 조제하였다.
2) 보톨리눔 독소의 투여 방법
30 gauge needle이 달린 1 cc 주사기에 보톡스�를 각각 2.5 unit(0.1 cc)씩 넣고 양측 단지신근에 각각 주사하였다. 한쪽의 단지신근에는 일반 생리식염수를 사용한 보톡스� 2.5 unit, 반대측 단지신근에는 보존 생리식염수를 사용한 보톡스� 2.5 unit를 무작위 방법 에 의해 각각 주사하였으며, 주사부위는 단지신근의 최 대 팽대부위인 복합근 활동전위가 최고로 측정되는 곳 을 선정하여 마킹 펜으로 표시한 후 근육 주사하였다.
3) 비골신경전도검사
보툴리눔 독소 주사 후 근육의 마비율을 측정하기 위 하여 Sloop 등9이 제안한 비골운동신경전도검사 모델을 사용하였다. 즉, 단지신근의 복합근 활동전위의 진폭 (baseline to peak)을 보톡스� 주사 전에 측정하고 보 톡스� 주사 후에 다시 측정하여 근육의 마비율을 구하 였다.
근전도 기기는 Sapphire (Medelec, Surrey, UK)
Fig. 1. Measurement of compound muscle action potentials.
Active surface electrode was attached to the extensor digitorum brevis muscle and reference surface electrode was attached to the fifth metatarsal head. Stimulation was applied 8 cm proximal to the recording electrode.
기기를 사용하였으며 여과주파수는 2~10 kHz, 민감 도는 2 mV/division, 스윕 지속시간(sweep dura- tion)은 2 ms/division으로 하였다.
대상자를 5분간 안정시킨 후 최대한 발 근육을 사용 하지 않고 편하게 있도록 하였으며 체표의 온도는 발등 부위에서 측정하여 32도 이상이 되도록 하였다. 활동 전극은 표면전극을 사용하여 단지신근의 팽대부에 부착 하였으며 참고 전극은 제5 중족골두에 부착하였다. 자 극은 활동전극으로부터 8 cm 떨어진 족관절 전면부에 서 비골신경을 초최대(supramaximal) 강도로 가하였 다(Fig. 1).
4) 추적관찰 및 통계방법
단지신근의 복합근 활동전위의 진폭을 보톡스� 주사 전, 주사 후 1주, 4주, 8주 12주째에 측정하였으며, 측 정된 복합근 활동전위의 진폭을 보톡스� 주사 전 기저 복합근 활동전위의 진폭에 대한 백분율로 환산하여 통 계처리 하였다. 통계처리는 paired t-test로 검정하였 으며 p값이 0.05 이하인 경우를 통계학적으로 유의한 것으로 판단하였다.
결 과
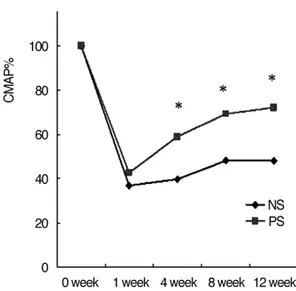
보톡스� 주사전 혼합용매에 따른 복합근 활동전위의 진폭의 차이는 없었다(p=0.66). 복합근 활동전위 (CMAP%)는 일반 생리식염수로 혼합한 보톡스�를 주 사한 경우와 보존 생리식염수를 혼합한 보톡스�를 주사 한 후 1주째 각각 36.77±14.31%, 42.54±14.21%로 감소 하였고 두 부위 간에 통계학적으로 유의한 차이는 없었다(p=0.33).
보톡스� 주사후 4주째 복합근 활동전위의 백분율은 각각 39.67±15.61%, 58.98±19.61%였고, 8주째에 는 47.99±13.15%, 69.19±11.58%, 12주째에는 48.16±14.10%, 72.22±16.73%로 감소하였고 두 부 위 사이에 통계학적으로 유의한 차이를 보였다 (p<0.05)(Table 1)(Fig. 2).
고 찰
현재 시판되고 있는 보툴리눔 독소 A형 중의 하나인 Botox�는 약값이 고가인데다 작은 근육의 치료에는 1 바이알(100 unit) 이하의 적은 용량만 필요한 경우가 종종 있기 때문에 실제 치료를 적용함에 있어 남은 양 을 다시 사용하기 위하여 재냉동 혹은 냉장보관을 하는 경우가 실제로 있는데 이경우 무균성의 유지와 역가의 감 소 가 문 제 로 대 두 된 다 . 실 제 로 Gartlan과 Fig. 2. Comparison of compound muscle action potentials
(CMAP) between sides injected with Botox�reconsti- tuted with normal saline (NS) and with preserved saline (PS). CMAP is expressed as percentage of baseline amplitude. CMAP % was more attenuated in one side treated with Botox�reconstituted with normal saline than in the other side treated with Botox�reconstituted with preserved saline (*P<0.05).
Table 1. Comparison of CMAP % recorded at Extensor Digitorum Brevis Between Sides Injected with Botox�Reconstituted with Normal Saline and Reconstituted with Preserved Saline
Normal saline Preserved saline
11 week 36.77±14.31 42.54±14.21*
14 weeks 39.67±15.61 58.98±19.61*
18 weeks 47.99±13.15 69.19±11.58*
12 weeks 48.16±14.10 72.22±16.73*
CMAP %: Compound muscle action potentials were expressed as percentage of the amplitude of the baseline.
Values are means±standard deviation (%).
*P<0.05 by paired t-test between normal saline and preserved saline.
Hoffman10은 보툴리눔 독소의 냉장 혹은 냉동 보관 후 2주째 보툴리눔 독소의 역가가 Swiss-Webster 쥐에서 감소되었다고 보고하였고, Paik 등11도 사람의 단지신 근에서 냉장 보관한 보툴리눔 독소를 주사한 결과 근육 마비의 효과가 감소한다고 보고하였다.
한편, 일부의 임상가들은 보툴리눔 독소의 냉장 혹은 냉동보관시 무균성을 유지하기 위하여 생리적 식염수가 아닌 보존 생리식염수(preserved saline)를 사용하기 도 한다.5-7 보존 생리식염수는 대게 0.9% 염화나트륨 외에 정균 작용을 하는 benzyl alcohol을 포함하고 있 는데 이 경우 주사 후에 통증이 적다는 보고도 있다.12 보존 생리식염수를 사용하였을 때 역가의 감소에 관하 여는 일반 생리식염수에 비하여 큰 차이가 없다는 보고 가 있었지만,13,6 이 연구들의 경우 주사 후 추적 관찰기 간이 짧고 보톨리눔 독소의 신경근 차단효과의 평가를 위한 객관적인 검사가 미약하였다. Gutman과 Pratt14 는 복합근 활동전위의 진폭 감소가 보톨리눔 독소에 의 해 유발된 신경근 차단효과를 반영하여 임상적 검사로 유용하게 사용될 수 있다고 제시하였으며 Sloop 등9은 정상인에서 비교적 잘 사용하지 않는 단지신근에 보툴 리눔 독소를 주사하고 그 복합근 활동전위를 측정함으 로써 신경근 차단효과를 측정할 수 있는 신경전도검사 모델을 제안하였다.
본 연구에서는 Sloop 등9의 모델을 이용하여 정상 성 인들을 대상으로 보톨리눔 독소를 단지신근에 주사 후 복합근활동전위의 진폭을 연속적으로 측정함으로써 혼 합용매간의 역가를 비교하였다. 그 결과 주사후 1주째 에는 복합근 활동전위의 백분율(CMAP%)이 일반 생 리식염수 혼합용매를 사용한 부위와 보존 생리식염수 혼합용매를 사용한 부위 사이에 통계학적으로 유의한 차이는 없었다. 이는 benzyl alcohol의 보톡스�에 대 한 영향이 충분히 나타나기 전에 측정된 결과에 의한 것으로 생각되고 4주, 8주 및 12주째에는 두 부위 사이 에 유의한 차이가 나타나는 결과를 보였다. 이는 보톡 스�의 혼합용매로 보존 생리식염수를 사용할 경우 ben- zyl alcohol에 의해 보톡스�가 부분적으로 불활성화 되 거나 benzyl alcohol의 영향으로 보톡스�의 역가가 감 소되는 것으로 가설로 제시되고 있고5,11 향후 그 기전에 대한 연구가 필요할 것으로 생각된다. 본 연구의 제한 점으로는 보톡스� 2.5 unit/0.1 ml를 단지신근에 근육 주사하여 역가의 변화를 관찰하였기 때문에 더 많은 용 량이 필요한 큰 근육에서의 역가 차이나 투여 횟수에 따른 역가 차이를 제시할 수 없었다. 그러나 본 연구에 서는 주사 후 3개월간의 충분한 추적 관찰과 보톨리눔 독소의 신경근 차단효과의 평가를 위해 객관적인 검사 를 시행하여 혼합용매에 따른 역가의 변화차이를 확인 할 수 있었다.
결 론
본 연구는 정상인들을 대상으로 단지신근의 한쪽에는 혼합용매로서 일반 생리식염수를 사용한 보톡스�를 근 주하고 반대편에는 보존 생리식염수를 혼합한 보톡스� 를 주사하여 양쪽 근육의 마비율을 복합근활동전위를 이용하여 비교하고 보툴리눔 독소의 혼합용매에 따른 근육 마비 효과를 확인하였다. 결론적으로 보툴리눔 독 소의 주사를 위한 혼합용매로 보존 생리식염수를 사용 할 경우 그 역가가 감소될 수 있으므로 이를 감안하여 야 한다.
참고문헌
01. Sellin LC: The action of batulinum toxin at the neuromus- cular junction. Med Biol 1981: 59: 11-20.
02. Scott AB: Botulinum toxin injection into extraocular mus- cles as an alternative to strabismus surgery. Ophthalmolo- gy 1980: 87: 1044-1049.
03. Schantz EJ, Johnson EA: Properties and use of botulinum toxin and other microbial neurotoxins in medicine. Micro- biol Rev 1992: 56: 80-99.
04. Mu¨nchau A, Bhatia KP: Uses of botulinum toxin injection in medicine today. BMJ 2000: 320: 161-165.
05. Klein AW: Dilution and storage of botulinum toxin. Der- matol Surg 1998: 24: 1179-1180.
06. Alam M, Dover JS, Arndt KA: Pain associated with injec- tion of botulinum A exotoxin reconstituted using isotonic sodium chloride with and without preservative: a double- blind, randomized controlled trial. Arch Dermatol 2002:
138: 510-514.
07. Kwiat DM, Bersani TA, Bersani A: Increased patient com- fort utilizing botulinum toxin type a reconstituted with preserved versus nonpreserved saline. Ophthal Plast Reconstr Surg 2004: 20: 186-189.
08. Schantz EJ, Kautter DA: Standardized assay for Clostridi- um botulinum toxins J Assoc Off Anal Chem 1978: 61:
96-99.
09. Sloop RR, Cole BA, Escutin RO: Reconstituted botulinum toxin type A does not lose potency in humans if it is refrozen or refrigerated for 2 weeks before use. Neurology 1997: 48: 249-253.
10. Gartlan MG, Hoffman HT: Crystalline preparation of bot- ulinum toxin type A (Botox): degradation in potency with storage. Otolaryngol Head Neck Surg 1993: 108: 135-140.
11. Paik NJ, Seo K, Eun HC: Reduced potency after refriger- ated storage of botulitum toxin A: human extensor digito-
rum brevis muscle study. Mov Disord 2006: 21: 1759- 1763.
12. Sarifakioglu N, Sarifakioglu E: Evaluating effects of preservative-containing saline solution on pain perception during botulinum toxin type-a injections at different loca- tions: a prospective, single-blinded, randomized controlled
trial. Aesthetic Plast Surg 2005: 29: 113-115.
13. Garcia A, Fulton JE, Jr.: Cosmetic denervation of the mus- cles of facial expression with botulinum toxin. A dose- response study. Dermatol Surg 1996: 22: 39-43.
14. Gutmann L, Pratt L: Pathophysiologic aspects of human botulism. Arch Neurol 1976: 33: 175-179.