The Relationship between Degree of Stress and Quality of Life in Mothers of Children with Cerebral Palsy
Mi-Jung Yun, PT, MSc1, Wan-Hee Lee, PT, PhD2, Jae-Sub Lee, PT3, Kyoung-Suk Lee1
1Department of Physical Therapy, Graduate School of Sahmyook University , 2Department of Physical Therapy, Sahmyook University (Korea Falls Prevention Institute), 3Department of Physical Therapy, The Catholic University of Korea, Incheon St. Mary’s Hospital
Purpose: This study investigated the relationship between degree of stress and quality of life in mothers of children with cerebral palsy.
Methods: This study’s subjects were 77 mothers of children under 10 years of age with cerebral palsy. The instrument is a self-administered, structured, written questionnaire. The tool that measured the degree of stress was created by modifying the questionnaire by Park (2004). Quality of life for all mothers with cerebral palsy was evaluated by the ShortForm-36 Health Questionnaire. To verify the effects on degree of stress and quality of life arising from general characteristics, t-tests and ANOVAs were conducted. The correlation between degree of stress and quality of life was analyzed via Pearson’s correlation analysis.
Results: The mothers’ degree of stress was rated as 2.69 out of 5; their quality of life was rated as 53.07 out of 100. There was a significant negative correlation between quality of life and the age of cerebral palsy and positive correlations between quality of life and mother’s age, background, and family income. Degree of stress among mothers has a positive correlation with quality of life.
Conclusion: This study provides basic data about the relationship between degree of stress and quality of life in mothers of children with cerebral palsy.
Keywords: Cerebral palsy, Mothers, Stress, Quality of life
I. Introduction
Despite advancements in modern medical science and the health management industry, rates of cerebral palsy (CP) continue to rise. It has been reported that 2.3 out of 1,000 infants develop CP.1,2 CP is attributed to non-progressive disorders occurring in the development of the fetal or infant brain that cause limitation of activity; sensory, cognitive, perception, and behavior disorders; and seizures.3
Many children with CP may have complex limitations in self-care functions, which could result in requirements for
long-term care far exceeding the usual needs of children.4 Mothers of children with CP have shown negative effects in terms of psychological status and mental health and have higher levels of depressive symptoms.2,5 The growth and development of a child with CP is greatly impacted by the child’s mother. In addition, the mother plays an important role in the child’s rehabilitation process. Studies on mothers of children with CP study outcomes including stress factors,6 depression, anxiety,7 and quality of life.8
In a previous study, the quality of life among mothers of children with CP was reported to be worse than that of normal children, and they also had lower scores for physical functioning, vitality, general health, and emotional roles.9
For the advanced research on stress of mothers with CP, there was reported that stress was related to community support10, the solutions for the mothers’ stress11, economical, psychological, social, physical, and educational stress12, the Received May 16, 2012 Revised June 6, 2012
Accepted June 7, 2012
Corresponding author Wan-Hee Lee, [email protected]
Copyright © 2012 by The Korean Society of Physical Therapy
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
The Journal of Korean Society of Physical Therapy Original Article
severity of CP, caregiver satisfaction13, high family needs, low family adaptability and cognitive impairment.14 However, very few studies have been conducted on stress and quality of life among mothers of children with CP.
The purpose of this study was to investigate the relation- ship between degree of stress and quality of life in mothers of children with CP. Through this study, primary caregivers and mothers of children with CP will be provided with provide data to help improve their quality of life as part of a comprehensive rehabilitation plan.
II. Materials and Methods
1. Subjects and periods
The subjects were out patients of Kaiser Rehabilitation Hospital in Guri and Eulji University Hospital in Daejeon.
The data of this research have been collected from January to April of 2011, and total of 110 participants answered the questionnaire. Inclusion criteria for the mothers of children with CP were as follows: (a) children had been diagnosed with CP by a specialist, (b) the mothers of children under 10 years of age with CP, (c) absence of a severe or chronic medical condition such as stroke, diabetes mellitus etc, (d) absence of history of severe or chronic psychological disorder. Among them, exclusion criteria for mothers of children with CP were follows: (a) those whose children had been diagnosed except CP such as mental retardation, Down syndrome etc, (b) those whose answers were not sincere enough to be used as research material. The questionnaires were distributed to participants after they agreed to hear a description of the research purpose and were informed of the autonomy of participation and the confidentiality of personal information. Self-administered, structured, written questionnaires were distributed to the participants.
A total of 77 mothers of children with CP who answered the questionnaire were selected as the subjects of the study.
2. Measurement and instruments
The study questionnaire included questions regarding general characteristics: gender, age, height, education level of mothers, family income, and included questions about
treatment status of children with CP of the sample: frequency of treatment, duration of treatment, duration of treatment, educational information for treatments, difficulty in the treatment, usefulness of mothers treated, adapted treatment.
Mothers of children with CP were measured with a tool revealing the degree of stress measurement, which was created by modifying the questionnaire by Park.11 Each survey question used a Likert-type 5-point rating method. To gauge stress, 29 questions are divided into three different areas: the disability status and prognosis area (8 items), the therapeutic area (10 items), and the personal role area (the interpersonal realm, 11 items). Cronbach’s α for this questionnaire was 0.84 in this study, while it was 0.94 in Park’s study.11
Quality of life for mothers of children with CP was evaluated by the Medical Outcomes Study ShortForm-36 (SF- 36) Health Questionnaire. The SF-36 Health Questionnaire was developed as a result of the Medical Outcomes Study.
The SF-36 health survey has 36 items and measures eight concepts: physical functioning (PF, 10 items), role restriction related to physical problems (3 items), bodily pain (BP, 2 items), general health perception (GH, 5 items), vitality (VT, 4 items), social functioning (SF, 2 items), role limitation because of emotional problems (RE, 3 items), and mental health status (MH, 5 items).15 Subscale scores are calculated according to standard procedures, and score values range between 0 and 100; higher scores indicate better conditions. The SF-36 has been shown to be a reliable and valid assessment tool for quality of life, and it has been used as an outcome indicator in numerous clinical trials and in a wide range of diagnostic groups.16,17 Reliability coefficients of the SF-36 has been shown 0.65 to 0.94.18
3. Data analysis
The collected data were analyzed using the SPSS ver. 12.0 software package (SPSS Inc., Chicago, IL, USA). The general characteristics of the subjects were calculated the number and percentage, the evaluation of degree of stress and quality of life were calculated mean and standard deviation of the descriptive statistics. To verify the effects on degree of stress and quality of life arising from general characteristics, an independent t-test and ANOVA were conducted. The
correlation between degree of stress and quality of life was analyzed via Pearson’s correlation analysis.
III. Results
General characteristics related to the gender and age of CP, academic background and age of the mothers of those children, and family income are listed in Table 1. The general target candidate showed the characteristic of CP in the gender of male for 51.9% of the male child (40 children), and 48.1% for female children (37 children). CP was most popular in the ages of 24 to 47 months (27 people), and the mothers of age 35 to 39, with 26 people. The education levels of mothers were the highest at college level being a total of 47 people, followed by high school graduation, and graduation school. The income of families appeared to be high with 2.5~2.99 million won and over 3 million won each for 25 people.
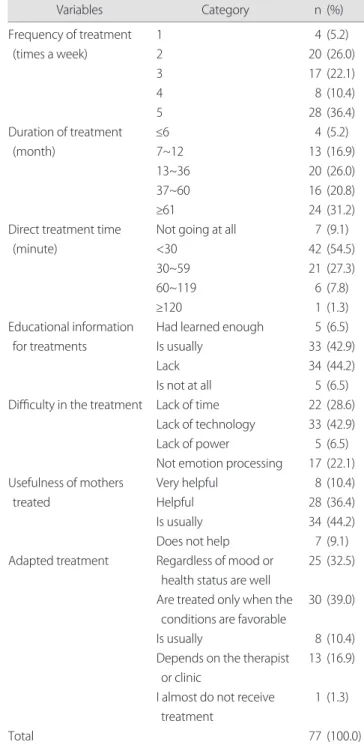
The treatment status of CP was listed in Table 2. The
treatment status of CP showed up to be its frequency of treatment as 5 times in a week tested from 28 people. The treatment duration appeared highest at 13 to 36 months, and the direct treatment appeared to be under 30 minutes for 42 people. Thirty-four people have claimed that there was a lack of educational information for treatments, including 33
Table 1. General characteristics of subjects
Variables Category n (%)
Gender of CP Ages of CP (month)
Ages of mothers (yr)
Education level of mothers
Family income (10,000 KRW)
Total
Male Female
<24 24~47 48~71
≥72
<30 30~34 35~39
≥40
Middle school High school College Graduate school
<150 150~199 200~249 250~299
≥300
40 37 13 27 22 15 16 23 26 12 0 27 47 3 2 11 14 25 25 77
(51.9) (48.1) (16.9) (35.1) (28.6) (19.5) (20.8) (29.9) (33.8) (15.6) (0.0) (35.1) (61) (3.9) (2.6) (14.3) (18.2) (32.5) (32.5) (100.0) CP: cerebral palsy, KRW: Korean won.
Table 2. Treatment status of children with cerebral palsy
Variables Category n (%)
Frequency of treatment (times a week)
Duration of treatment (month)
Direct treatment time (minute)
Educational information for treatments
Difficulty in the treatment
Usefulness of mothers treated
Adapted treatment
Total
1 2 3 4 5
≤6 7~12 13~36 37~60
≥61
Not going at all
<30 30~59 60~119
≥120
Had learned enough Is usually
Lack Is not at all Lack of time Lack of technology Lack of power
Not emotion processing Very helpful
Helpful Is usually Does not help Regardless of mood or
health status are well Are treated only when the
conditions are favorable Is usually
Depends on the therapist or clinic
I almost do not receive treatment
4 20 17 8 28 4 13 20 16 24 7 42 21 6 1 5 33 34 5 22 33 5 17 8 28 34 7 25 30
8 13 1 77
(5.2) (26.0) (22.1) (10.4) (36.4) (5.2) (16.9) (26.0) (20.8) (31.2) (9.1) (54.5) (27.3) (7.8) (1.3) (6.5) (42.9) (44.2) (6.5) (28.6) (42.9) (6.5) (22.1) (10.4) (36.4) (44.2) (9.1) (32.5) (39.0)
(10.4) (16.9) (1.3) (100.0)
people who have considered difficulty of treatment due to the lack of educational treatment information. Thirty people have answered that when treating for CP, the child best accepts or adapts to treatment when the conditions are favorable.
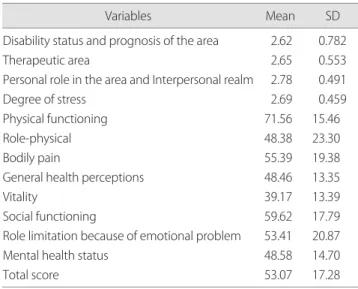
Mean scores for the degree of stress and quality of life are listed in Table 3. The degree of stress of the mothers were an average of 2.69 out of 5, observing by domains the stress from disability status and prognosis of the area 2.62 out of 5, 2.65 from therapeutic area, 2.78 from personal role in the area and Interpersonal realm. The quality of life of mothers with CP was 53.07 out of 100. The average rates by domains in order are 71.56 for physical functioning, 59.62 for social functioning, and 55.39 for bodily pain.
According to the results of the difference of quality of life and stress caused under the general characteristics and the treatment status, there has not been a remarkable statistic difference (Table 4).
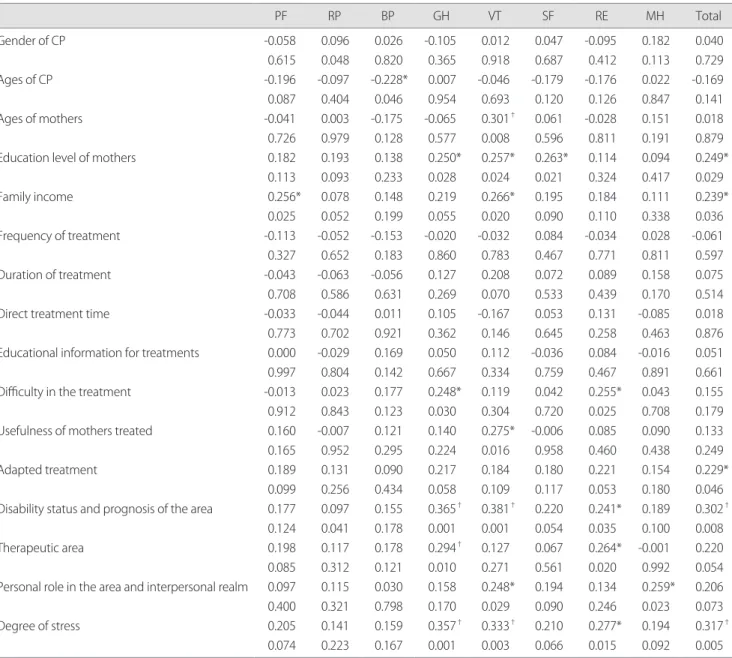
The Pearson’s correlation coefficients between SF-36 measures, treatment variables, and general characteristics of mothers with CP were as follows: -0.228 between the age of CP and bodily pain; 0.301 between the age of the mother and vitality; 0.250, 0.257, and 0.263 between the academic background of the mother and general health perception, vitality, and social functioning, respectively; 0.256 between
family income and physical functioning; and 0.266 between family income and vitality.
Correlation coefficients associated with the treatment status of CP were 0.248 between difficulty in treatment and general health perception 0.255 between role limitation and emotional problems, and 0.275 between mothers’ feelings of usefulness and vitality. The candidates’ general characteristics were in correlation with the education level of the mothers, family income, and child’s adapted treatment, and the level of life quality and the coefficient of correlation are 0.249, 0.239, 0.229, showing the amount of positive correlation.
The Pearson’s correlation coefficients between SF-36 measures and the degree of stress among mothers were 0.365, 0.381, and 0.241 between disability status/prognosis area and general health perception, vitality, and role limitation because of emotional problems, respectively; 0.294 between therapeutic area and general health perception; 0.264 between therapeutic area and role limitation because of emotional problem; 0.248 between personal roles in the area and interpersonal realm and vitality; 0.259 between personal roles and mental health status; and 0.357, 0.333, and 0.277 between degree of stress and perceived general health, vitality, and role limitation because of emotional problems, respectively. Correlation coefficients between SF-
Table 3. Mean score on degree of stress and SF-36 quality of life parameters of the mothers
Variables Mean SD
Disability status and prognosis of the area Therapeutic area
Personal role in the area and Interpersonal realm Degree of stress
Physical functioning Role-physical Bodily pain
General health perceptions Vitality
Social functioning
Role limitation because of emotional problem Mental health status
Total score
2.62 2.65 2.78 2.69 71.56 48.38 55.39 48.46 39.17 59.62 53.41 48.58 53.07
0.782 0.553 0.491 0.459 15.46 23.30 19.38 13.35 13.39 17.79 20.87 14.70 17.28 Values are number of mean±standard deviation.
SF-36: ShortForm-36.
Table 4. Difference of degree of stress and quality of life followed characteristics
Variables Degree of stress Quality of life
t or F p t or F p
Gender of CP Ages of CP Ages of mothers (yr) Education level of mothers Family income
Frequency of treatment Duration of treatment Direct treatment time Educational information for treatments
Difficulty in the treatment Usefulness of mothers treated Adapted treatment
0.825 0.007 0.896 0.862 0.851 0.824 0.336 1.281 0.501
0.608 0.809 1.757
0.367 0.999 0.448 0.427 0.498 0.514 0.853 0.285 0.683
0.612 0.493 0.147
0.059 1.397 0.153 2.856 1.604 0.260 0.955 0.336 0.379
0.993 0.562 1.173
0.809 0.250 0.928 0.064 0.183 0.902 0.437 0.853 0.768
0.401 0.642 0.330 CP: cerebral palsy.
36 measures and total of the degree of stress among mothers were 0.302, 0.317 between disability status/prognosis area and degree of stress (Table 5).
IV. Discussion
This study was intended to provide basic data to improve the quality of life of mothers with CP in the future by identifying their degree of stress and their quality of life and discovering
the correlations between them.
Treatments of CP are conducted by a team approach considering various factors, including the development of CP, clinical type, severity of disability, and accessibility of treatment; mothers play a crucial role in all these processes.19 Mothers with CP have a high risk of depression related to their stress.2
The average degree of the mothers’ stress was rated as 2.69, similar to the result of 2.65 from a study by Jung10 on stress
Table 5. Correlation (r) between characteristics and SF-36 quality
PF RP BP GH VT SF RE MH Total
Gender of CP Ages of CP Ages of mothers
Education level of mothers Family income
Frequency of treatment Duration of treatment Direct treatment time
Educational information for treatments Difficulty in the treatment
Usefulness of mothers treated Adapted treatment
Disability status and prognosis of the area Therapeutic area
Personal role in the area and interpersonal realm Degree of stress
-0.058 0.615 -0.196 0.087 -0.041 0.726 0.182 0.113 0.256*
0.025 -0.113 0.327 -0.043 0.708 -0.033 0.773 0.000 0.997 -0.013 0.912 0.160 0.165 0.189 0.099 0.177 0.124 0.198 0.085 0.097 0.400 0.205 0.074
0.096 0.048 -0.097 0.404 0.003 0.979 0.193 0.093 0.078 0.052 -0.052 0.652 -0.063 0.586 -0.044 0.702 -0.029 0.804 0.023 0.843 -0.007 0.952 0.131 0.256 0.097 0.041 0.117 0.312 0.115 0.321 0.141 0.223
0.026 0.820 -0.228*
0.046 -0.175 0.128 0.138 0.233 0.148 0.199 -0.153 0.183 -0.056 0.631 0.011 0.921 0.169 0.142 0.177 0.123 0.121 0.295 0.090 0.434 0.155 0.178 0.178 0.121 0.030 0.798 0.159 0.167
-0.105 0.365 0.007 0.954 -0.065 0.577 0.250*
0.028 0.219 0.055 -0.020 0.860 0.127 0.269 0.105 0.362 0.050 0.667 0.248*
0.030 0.140 0.224 0.217 0.058 0.365† 0.001 0.294† 0.010 0.158 0.170 0.357† 0.001
0.012 0.918 -0.046 0.693 0.301† 0.008 0.257*
0.024 0.266*
0.020 -0.032 0.783 0.208 0.070 -0.167 0.146 0.112 0.334 0.119 0.304 0.275*
0.016 0.184 0.109 0.381† 0.001 0.127 0.271 0.248*
0.029 0.333† 0.003
0.047 0.687 -0.179 0.120 0.061 0.596 0.263*
0.021 0.195 0.090 0.084 0.467 0.072 0.533 0.053 0.645 -0.036 0.759 0.042 0.720 -0.006 0.958 0.180 0.117 0.220 0.054 0.067 0.561 0.194 0.090 0.210 0.066
-0.095 0.412 -0.176 0.126 -0.028 0.811 0.114 0.324 0.184 0.110 -0.034 0.771 0.089 0.439 0.131 0.258 0.084 0.467 0.255*
0.025 0.085 0.460 0.221 0.053 0.241*
0.035 0.264*
0.020 0.134 0.246 0.277*
0.015
0.182 0.113 0.022 0.847 0.151 0.191 0.094 0.417 0.111 0.338 0.028 0.811 0.158 0.170 -0.085 0.463 -0.016 0.891 0.043 0.708 0.090 0.438 0.154 0.180 0.189 0.100 -0.001 0.992 0.259*
0.023 0.194 0.092
0.040 0.729 -0.169 0.141 0.018 0.879 0.249*
0.029 0.239*
0.036 -0.061 0.597 0.075 0.514 0.018 0.876 0.051 0.661 0.155 0.179 0.133 0.249 0.229*
0.046 0.302† 0.008 0.220 0.054 0.206 0.073 0.317† 0.005 SF-36: ShortForm-36, PF: physical functioning, RP: role restriction related to physical problems, BP: bodily pain, GH: general health perception, VT: vitality, SF: social functioning, RE: role limitation because of emotional problem, MH: mental health status.
*Statistically significant difference. *p<0.005, †p<0.001.
among the mothers of CP. However, these values are lower than the 3.47 obtained in a study by Lee et al.12 and the 3.30 from a study by Park11 on the same topic. This study showed that the highest level of stress came from personal roles and the interpersonal realm.
According to the results of the difference of quality of life and stress caused under the situation of a mother with a child suffering from CP and treatment, there has not been a remarkable statistic difference. It is suspected that there were an insufficient number of examples to show a notable difference, or the target candidates may have been relatively well-adapted to dealing with stress. One correlation between the subjects’ general characteristics and treatment shown in this study was that the child’s age was negatively correlated with the mother’s bodily pain. The reason could be that bodily pain was affected by changes in the difficulty of caring for a child as his/her body grows. A mother’s age was positively correlated with vitality, and her academic background was positively correlated with general health perception, vitality, and social functioning. Family income was positively correlated with physical functioning and vitality. These findings show that the higher a mother’s age, academic background, and family income are, the higher was her quality of life; these findings are consistent with the studies by Sohn20 and Kwon21.
The findings of correlations between the degree stress among mothers and their quality of life are as follows:
disability status and prognosis was area are positively correlated with general health perception, vitality, and role limitation because of emotional problems; therapeutic area is positively correlated with general health perception and role limitation because of emotional problems; personal roles and the interpersonal realm are positively correlated with vitality and mental health status; and the mother’s degree of stress was positively correlated with general health perception, vitality, and role limitation because of emotional problems. In the social area, a study of maternal stress and quality of life by Lee et al.12 showed similar results to this study.
These findings show that mothers who believe that they have high quality of life feel more stress. These mothers dislike the deterioration of their CP’s condition and feel more
pressure concerning the uncertainty in their child’s recovery.
They feel more stress about long treatment periods and the lack of perfect treatment; further, they feel that their work in taking care of their children was burdensome. They also derive stress from personal relationships. They want to be confident in themselves, to meet friends, and to be good at maintaining personal relationships. That was, their higher recognition of their need for social activities was reflected in their higher stress level.
Mothers of children with CP may have had low scores on the mental component and other relevant components of quality of life because they cannot receive a sufficient amount of mental and psychological support in their environment.
This is not only a family matter but also a social matter requiring policy support. Therefore, there is a need for a social program to be developed in which both physical and psychological support can be provided to mothers with CP.
This research has been conducted targeting at mothers with child suffering from CP, carrying meaning in the comparison of relative prescience of the factors that might affect the survey such as the candidate personality amongst many, which affects the amount of stress and the life quality of the mother. And the evaluation on stress seems to be limited due to the constraint of topics, an expanded and detailed research for the subject of stress may be required, as well as repetition of research with expansion of candidate numbers and regions.
With an intention to provide basic data for developing measures to improve the quality of life of the mothers with CP, this study identified degree of the mothers’ stress and quality of life and examined correlations between them. The findings are as follows.
1) Degree of the mothers’ stress was 2.69 out of 5 and quality of life was 53.07 out of 100.
2) Correlations between quality of life and other factors, based on the general characteristics, were showed: a negative correlation with the age of CP, and positive correlations with mother’s age, background and family income.
3) Degree of the mothers’ stress has a positive correlation with quality of life.
These results demonstrate a need for the development of a program that enables mothers to improve their quality of life by turning stress into bliss. Social strategy and research are both necessary to improve quality of life, which is required in order to achieve more comprehensive rehabilitation for children with CP.
Author Contributions
Research design: Lee JS
Acquisition of data: Lee JS, Yun MJ
Analysis and interpretation of data: Yun MJ, Lee KS Drafting of the manuscript: Yun MJ
Administrative, technical, and material support: Lee WH Research supervision: Lee WH
References
1. Ko JY, Lee SM. Functions (mobility, self-care, social ability) and health-related quality of life in children with cerebral palsy. J Korean Soc Phys Ther. 2010;22(3):37-44.
2. Manuel J, Naughton MJ, Balkrishnan R et al. Stress and adaptation in mothers of children with cerebral palsy. J Pediatr Psychol.
2003;28(3):197-201.
3. Rosenbaum P, Paneth N, Leviton A et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007;109:8-14.
4. Raina P, O’Donnell M, Schwellnus H et al. Caregiving process and caregiver burden: conceptual models to guide research and practice. BMC Pediatr. 2004;4:1.
5. Yim SY, Moon HW, Rah UW et al. Psychological characteristics of mothers of children with disabilities. Yonsei Med J. 1996;37(6):380- 4.
6. Choi ES, Park JH, Kim YT et al. Estimation of Stress level in mothers with cerebral palsy children. J Korean Acad Rehabil Med.
1998;22(5):1028-34.
7. Yun JH, Kang JM, Kim KS et al. Health-related quality of life in korean patients with chronic diseases. J Korean Rheum Assoc.
2004;11(3):263-74.
8. Cho YK, Kim EJ, Park JW et al. Assessment of quality of life in parents of children with cerebral palsy. J Korean Acad Rehabil Med. 2008;32(6):682-8.
9. Tuna H, Unalan H, Tuna F et al. Quality of life of primary caregivers of children with cerebral palsy: a controlled study with Short Form-36 questionnaire. Dev Med Child Neurol. 2004;46(9):647-8.
10. Jung HJ. The study of relationship between social support and mother’s stress with cerebral palsy children. Dankook University.
Dissertation of Master’s Degree. 2002.
11. Park ES. The study on stress and management on mothers of children with cerebral palsy. Daejeon University. Dissertation of Master’s Degree. 2004.
12. Lee JH, Kim HY, Lee JH. A study on maternal stress in rearing children with disabilities and maternal quality of life. J Korean Acad Child Health Nurs. 2007;13(1):5-12.
13. Dagenais L, Hall N, Majnemer A et al. Communicating a diagnosis of cerebral palsy: caregiver satisfaction and stress. Pediatr Neurol.
2006;35(6):408-14.
14. Glenn S, Cunningham C, Poole H et al. Maternal parenting stress and its correlates in families with a young child with cerebral palsy.
Child Care Health Dev. 2009;35(1):71-8.
15. Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-83.
16. Leidy NK, Elixhauser A, Vickrey B et al. Seizure frequency and the health-related quality of life of adults with epilepsy. Neurology.
1999;53(1):162-6.
17. Kaya K, Unsal-Delialioglu S, Ordu-Gokkaya NK et al. Musculo- skeletal pain, quality of life and depression in mothers of children with cerebral palsy. Disabil Rehabil. 2010;32(20):1666-72.
18. McHorney CA, Ware JE Jr, Lu JF et al. The MOS 36-item short- form health survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Med Care. 1994;32(1):40-66.
19. Ones K, Yilmaz E, Cetinkaya B et al. Assessment of the quality of life of mothers of children with cerebral palsy (primary caregivers).
Neurorehabil Neural Repair. 2005;19(3):232-7.
20. Sohn HS. A study on quality of life index of mothers with cerebral palsy children. Graduate school of health science and management. Yonsei University. Dissertation of Master’s Degree.
2005.
21. Kwon MJ. Satisfaction of utilization of physical therapy and quality of life for caregivers of cerebral palsy children. J Korean Soc Phys Ther. 2009;21(2):55-63.