Pigmented Mammary Paget Disease
Vol. 26, No. 6, 2014 747
Received April 24, 2013, Revised May 20, 2013, Accepted for publication May 30, 2013
Corresponding author: Mi Ryung Roh, Department of Dermatology, Gangnam Severance Hospital, 211 Eonj-uro, Gangnam-gu, Seoul 135-720, Korea. Tel: 82-2-2019-3363, Fax: 82-2-3463-6136, E-mail:
karenroh@yuhs.ac
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://
creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ann Dermatol Vol. 26, No. 6, 2014 http://dx.doi.org/10.5021/ad.2014.26.6.747
CASE REPORT
Pigmented Mammary Paget Disease Misdiagnosed as Malignant Melanoma
Ji Hye Lee, Tae Hyung Kim, Soo-Chan Kim, You Chan Kim1, Mi Ryung Roh
Department of Dermatology, Gangnam Severance Hospital, Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, 1Department of Dermatology, Ajou University School of Medicine, Suwon, Korea
Pigmented mammary Paget disease is a very rare clinicopath- ologic variant of mammary Paget disease. Diagnosis is often difficult because its clinical and histological features are very similar to those of malignant melanoma. Herein, we report a case of pigmented mammary Paget disease misdiagnosed as malignant melanoma. (Ann Dermatol 26(6) 747∼750, 2014)
-Keywords-
Malignant melanoma, Mammary paget disease
INTRODUCTION
Pigmented mammary Paget disease is a very rare clinico- pathologic variant of mammary Paget disease. Because the clinical and histological features of pigmented mammary Paget disease are very similar to those of malignant mela- noma, it is very difficult to differentiate and diagnose.
Herein, we describe a case of pigmented mammary Paget disease mimicking malignant melanoma.
CASE REPORT
A 67-year-old Asian woman with a history of breast and
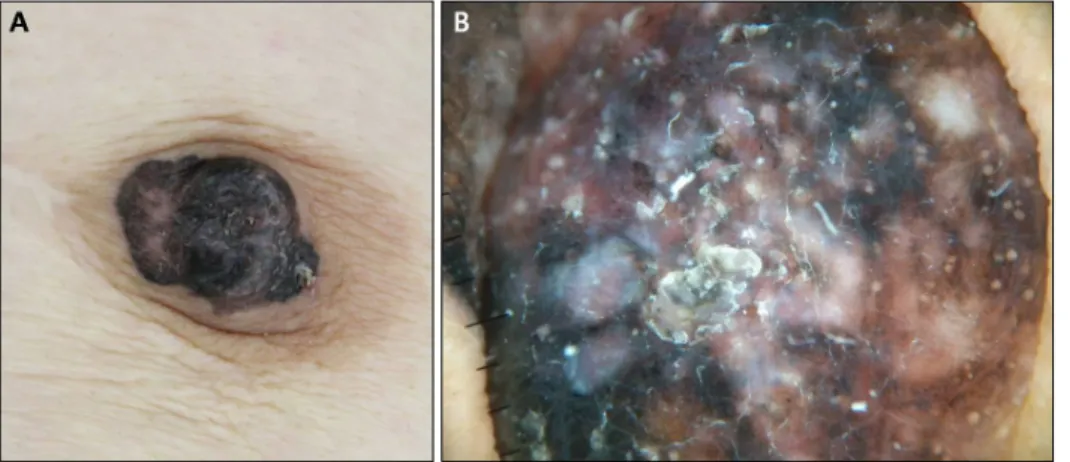
thyroid cancers presented with an asymptomatic brownish to black plaque on the left nipple that had been present for 10 years (Fig. 1A). Ten years previously, she had a diagnosis of ductal carcinoma in situ of the left breast and she underwent partial mastectomy with postoperative radiation therapy. She had regular positron emission tomo- graphy/computed tomography (PET/CT) scans for recur- rence evaluation during the 10-year follow-up period. Her last PET/CT scan follow-up was 2 years ago; however, no evidence of recurrence or metastasis was noted at that time. On dermoscopy, the lesion showed multiple colors, irregular dots/globules, small gray-blue pepper-like granules, and scar-like depigmentation, which strongly suggest malignant melanoma (Fig. 1B). A punch biopsy was performed at the darkest part of the lesion. Hematoxylin and eosin staining showed large neoplastic epithelial cells with pigmentation. Furthermore, a focal neoplastic micro- infiltration was seen in the superficial dermis with moder- ate inflammatory infiltrate (Fig. 2A). On the basis of the clinical and histopathologic findings, the lesion was diagnosed as malignant melanoma. Following this initial biopsy, wide excision with 1 cm margins and sentinel lymph node biopsy were performed. In frozen-section examination, micrometastases were not identified; there- fore, a complete lymph node dissection was not performed.
Hematoxylin and eosin staining of the excised specimens showed atypical epithelial cells with pale cytoplasm containing hyperchromatic large nuclei. The tumor cells were scattered or formed clusters along and above the basal layer of the epidermis; however, the cells were restricted within the epidermis. Inflammatory cell infiltra- tion, mostly composed of lymphocytes, with some mela- nophages in the superficial dermis was also seen (Fig. 2B).
Immunohistochemical tests showed that the tumor cells were positive for cytokeratin 7 (CK7) (Fig. 2C), epithelial membrane antigen (EMA), and C-erbB2 (Fig. 2D). The
JH Lee, et al
748 Ann Dermatol
Fig. 1. Clinical and dermoscopic features of pigmented mammary Paget disease. (A) Well-demarcated dark brown plaque on the nipple.
(B) Dermoscopy shows irregular dots/globules, gray-blue pepper-like granules, and a scar-like appearance.
cytoplasm of the tumor cells was positive for D-PAS staining. The tumor cells were negative for S-100, HMB-45 (Fig. 2E), and Melan-A staining (Fig. 2F). On the basis of these findings, the diagnosis was revised as pigmented mammary Paget disease. The sentinel lymph node in frozen section was reported negative for micrometastases;
however, the final pathologic report with immunohisto- chemical staining showed metastatic carcinoma in one lymph node (maximal metastasis dimension, 2 mm). The patient was referred to the general surgery department for total mastectomy and total axillary lymphadenectomy. A diagnosis of invasive ductal cancer was concluded after mastectomy, and the patient is currently undergoing chemo- therapy.
DISCUSSION
Paget disease of the breast usually presents as an erythe- matous patch mimicking nipple eczema. However, Azzo- pardi and Eusebi1 first described pigmented mammary Paget disease as a pigmentation of breast carcinoma in 1977. Currently, about 35 cases have been reported in the literature2. A possible explanation for the mechanism of hyperpigmentation was that Paget cells might induce the production of melanin from normal melanocytes3.
Because the clinical, dermoscopic, and histologic features are very similar with malignant melanoma, immunohisto- chemical staining is essential for differentiating pigmented mammary Paget disease from malignant melanoma. The tumor cells show positive staining for CK7, EMA, C-erbB2, and CAM 5.2 but negative for melanoma cell markers such as S-100, Melan-A, and HMB-454. In our case, because the clinical, dermoscopic, and histological features of the patient were consistent with the features of malignant melanoma, we performed a wide excision without immunohistoche-
mical evaluation. Because a misdiagnosis was made owing to a lack of evaluation, an unnecessary excision was performed before total mastectomy.
Although it is very difficult to differentiate Paget cells from melanoma cells on the basis of histologic features, there are some different features between them. Paget cells are situated above the basal keratinocytes with some ductal formation, whereas melanoma cells are located in all layers of the epidermis including the basal layer, with intraepidermal pagetoid spread. Also, Paget cells are not seen freely in the dermis, whereas melanoma cells may be present in the dermis5,6. Nevertheless, as these differences are not often obvious, immunohistochemical staining is necessary.
An intraductal or infiltrating ductal carcinoma of the breast can be seen in association with mammary Paget disease7. In our case, the patient also previously had ductal carci- noma in situ and received partial mastectomy with posto- perative radiation therapy. However, although our patient had regular evaluations with biennial PET/CT scan and annual mammography during 10 years, mammary Paget disease has not been detected. A few case reports have documented the efficacy of the detection of extramam- mary Paget disease by using PET/CT scan; however, there is no report about its usefulness in mammary Paget disease. In our case, PET/CT scan did not detect the lesion although it has been existing for 10 years. Therefore, skin biopsy should be performed in suspicious lesions by using checklists such as the ABCDE criteria.
Because the treatment and prognosis of pigmented mam- mary Paget disease and malignant melanoma are different, the diagnosis of pigmented lesions of the breast should be decided carefully. In this case, immunohistochemical sta- ining is indispensable for the final diagnosis of pigmented mammary Paget disease.
Pigmented Mammary Paget Disease
Vol. 26, No. 6, 2014 749 Fig. 2. Histologic and immunohistochemical features of pigmented mammary Paget disease. (A) Initial biopsy specimen showing large neoplastic epithelial cells with pigmentation and dermal melanophages (H&E, ×400). (B) Excision specimen showing intraepidermal proliferation of atypical cells with large hyperchromatic nuclei and pale cytoplasm (H&E, ×400). Tumor cells express immunoreactivity for (C) cytokeratin 7 (CK7, ×100) and (D) C-erbB2 (×100). Tumor cells show negative immunoreactivity for (E) HMB45 (×100) and (F) Melan-A (×100).
REFERENCES
1. Azzopardi JG, Eusebi V. Melanocyte colonization and pigmen- tation of breast carcinoma. Histopathology 1977;1:21-30.
2. Yanagishita T, Tamada Y, Tanaka M, Kasugai C, Takahashi E, Matsumoto Y, et al. Pigmented mammary Paget disease mimicking melanoma on dermatoscopy. J Am Acad Dermatol 2011;64:e114-e116.
JH Lee, et al
750 Ann Dermatol
3. Saitoh K, Saga K, Okazaki M, Maeda K. Pigmented primary carcinoma of the breast: a clinical mimic of malignant melanoma. Br J Dermatol 1998;139:287-290.
4. Al-Daraji WI, O'Shea AM, Looi LM, Yip CH, Ellis I. Pig- mented mammary Paget's disease: not a melanoma. Histopa- thology 2009;54:614-617.
5. Requena L, Sangueza M, Sangueza OP, Kutzner H. Pig- mented mammary Paget disease and pigmented epidermo- tropic metastases from breast carcinoma. Am J Dermatopathol
2002;24:189-198.
6. Meyer-Gonzalez T, Alcaide-Martin A, Contreras-Steyls M, Mendiola M, Herrera-Acosta E, Herrera E. Pigmented mam- mary Paget disease mimicking cutaneous melanoma. Int J Dermatol 2010;49:59-61.
7. Soler T, Lerin A, Serrano T, Masferrer E, García-Tejedor A, Condom E. Pigmented paget disease of the breast nipple with underlying infiltrating carcinoma: a case report and review of the literature. Am J Dermatopathol 2011;33:e54-e57.