J Korean Soc Radiol 2017;76(6):375-385 https://doi.org/10.3348/jksr.2017.76.6.375
INTRODUCTION
Breast cancer is the most common cancer and is the leading cause of cancer death among women worldwide, accounting for 23% of all new cancer cases and 14% of all cancer deaths (1).
Approximately 7% to 9% of all breast cancers are diagnosed in women under 40 years of age, and less than 4% are found in women under 35 (1). The median age of breast cancer patients in Asia is lower than that in Western countries, and the propor- tion of young breast cancer patients is much higher. Breast cancer in young women accounts for up to 4.8% of cancers diagnosed in Western countries, but more than 10% of cancers diagnosed
in Asian countries (2, 3).
Breast cancer in young women generally has biological fea- tures indicating a more aggressive tumor, including a more ad- vanced tumor stage, more aggressive subtypes, and higher his- tological grades than in older women, and these characteristics are correlated with an increased risk of death (2-4). Breast cancer in young women is more likely to be associated with family his- tory and gene mutations, such as BRCA mutations, than in older breast cancer patients (5). Moreover, young women with breast cancer have higher local recurrence rates after either breast-con- serving surgery or mastectomy compared to older women (6).
Some studies have reported that breast cancer patients under
Clinicopathological and Imaging Features of Breast Cancer in Korean Women under 40 Years of Age
40세 미만 젊은 유방암 환자의 임상적, 병리학적, 영상의학적 특징
Junwoo Kim, MD
1, Mijung Jang, MD
1*, Sun Mi Kim, MD
1, Bo La Yun, MD
1, Jong Yoon Lee, MD
1, Eun-Kyu Kim, MD
2, Eunyoung Kang, MD
2, So Yeon Park, MD
3Departments of 1Radiology, 2Surgery, 3Pathology, Seoul National University Bundang Hospital, Seongnam, Korea
Purpose: To evaluate the clinicopathological and imaging features of mammogra- phy, ultrasonography, and magnetic resonance imaging (MRI) for breast cancer in Korean women under 40 years of age according to molecular subtypes.
Materials and Methods: We included 183 breast cancers in 176 consecutive women under 40 years old who had been diagnosed with breast cancer between January 2012 and November 2014. The patients’ clinical and pathologic records were available as electronic medical records. A retrospective review of the pre-operative imaging studies was performed with 177 mammographies, 183 ultrasonographies, and 178 MRIs.
Results: Eighty-six percent (158/183) of lesions were symptomatic, with masses (147/183) as the most common presentation. Eighty percent (22/25) of the asymp- tomatic lesions were diagnosed via screening ultrasonography. The luminal A subtype was the most common (n = 79, 43%), human epidermal growth factor receptor 2-en- riched subtype showed indistinct margins on mammography (p = 0.006), the triple negative subtype depicted a posterior enhancement on ultrasonography (p < 0.001) and rim enhancement on MRI (p < 0.001).
Conclusion: Breast cancers in Korean women under 40 years of age are commonly presented with a palpable mass, and luminal A is the most common molecular sub- type. In our study, the imaging and pathologic characteristics of breast cancer in younger women were similar to those previously reported for older patients.
Index terms Breast Cancer Mammography Ultrasonography
Magnetic Resonance Imaging Young Adult
Received August 4, 2016 Revised November 10, 2016 Accepted December 19, 2016
*Corresponding author: Mijung Jang, MD Department of Radiology, Seoul National University Bundang Hospital, 82 Gumi-ro 173beon-gil, Bundang-gu, Seongnam 13620, Korea.
Tel. 82-31-787-7622 Fax. 82-31-787-7614 E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distri- bution, and reproduction in any medium, provided the original work is properly cited.
40 years of age tended to receive delayed diagnoses, which could be related to the more advanced stage presentations of this pop- ulation (7, 8). Moreover, it is possible that a limited availability of cancer surveillance programs may cause delayed diagnosis, although this stance is controversial (9).
Many studies have reported an increase in the proportion of breast tumors with hormone receptor (HR) negativity and upreg- ulated human epidermal growth factor receptor 2 (HER2) in young women (10). In general, young women are most likely to be diagnosed with HR-positive/HER2-negative breast cancer; fol- lowed by cancers that are triple negative (TN) for estrogen recep- tor (ER), progesterone receptor (PR), and HER2; then by HR pos- itive/HER2-enriched tumors, and finally by HR negative/HER2- enriched subtypes (11). A recent study suggested that poorer outcomes in breast cancer treatment for young Korean patients might be the result of an increased frequency of TN/HER2-en- riched subtypes as well as the more aggressive clinical behavior of HR-positive tumors compared to those in older patients (11). Al- though there are many conflicting results and limited data, there remains a need to investigate breast cancer in younger women, es- pecially with respect to breast cancer subtypes.
In this study, we retrospectively reviewed mammography, ul- trasonography (US), and magnetic resonance imaging (MRI) findings of breast cancers in women under 40 years of age to identify correlations between the imaging features and immu- nohistochemical subtypes. Such correlations would be useful to characterize breast cancers in patients under 40 years of age and improve the interpretations of imaging findings.
MATERIALS AND METHODS
Patient Selection
Our Institutional Review Board approved this retrospective study, and the informed consent requirement was waived. A re- view of the medical records of patients treated between January 2012 and November 2014 at our institution revealed 1618 con- secutive women who had been diagnosed with breast carcino- ma. Among these patients, 184 (11.4%) women younger than 40 years who had undergone preoperative breast imaging were included in our study. Among these patients, 8 women who un- derwent an excisional biopsy for diagnosis before imaging were excluded. Hence, 183 lesions from 176 patients were analyzed
in our study.
The following clinicopathological information was recorded:
clinical symptoms, family history of breast cancer, previous his- tory of breast and/or ovarian cancer, marriage status, gravidity/
parity, histologic subtype and grade of tumors, tumor stage, nod- al status, and type of surgery. A mammography was available for 178 lesions, US for all 183 lesions, and MRI for 178 lesions.
Two radiologists retrospectively reviewed the image character- istics and reported their findings after arriving at a consensus.
They had 10 and 2 years of experience, respectively, and knew that the patients had been diagnosed with breast cancer, but were blind to the immunohistochemical subtypes.
Histopathological Analysis
The histological results were classified as invasive ductal car- cinoma (IDC), ductal carcinoma in situ (DCIS), both IDC and DCIS (IDC + DCIS), infiltrating lobular carcinoma, or others.
The pathology report of each surgical specimen was used as the gold standard. Immunohistochemistry (IHC) was used to eval- uate the expression of ER, PR, HER2, and Ki-67. ER and PR were regarded as positive if at least 1% of the tumor nuclei were positively stained (12). Regarding the Ki-67 proliferation index, cases with ≥ 14% positive tumor cells were regarded as having a high proliferation index (13). The expression of HER2 was scored according to the guidelines of the American Society of Clinical Oncology/College of American Pathologists (12). The tumors were considered HER2-positive if they had scores of 3 + on IHC or equivocal cases on IHC which were confirmed by HER2 gene amplification via fluorescence or silver in situ hybridization.
Each breast cancer was classified as luminal A (ER +, PR +/-, HER2 -, Ki-67 < 14%), luminal B (ER +, PR +/-, HER2 +/-, Ki- 67 ≥ 14%), HER2-enriched (ER -, PR -, HER2 +), or TN (ER -, PR -, HER2 -) (12).
Mammography
A digital mammography was performed in two standard im- aging planes (craniocaudal and mediolateral oblique view of each breast) using the Senographe 2000D (GE Healthcare, Milwaukee, WI, USA) or Selenia Dimensions (Hologic, Bedford, MA, USA) for 178 lesions. The description and evaluation of the mammo- graphic findings were based on the lexicon and classifications of the American College of Radiology Breast Imaging Report-
ing and Data System (ACR-BI-RADS 5th edition) (14). The le- sions were described as masses (for which size, shape, margin, and density were reported), calcification (for which size, shape, and distribution were reported), or asymmetry or architectural distortions (for which sizes were reported).
US
US examinations were performed on all 183 lesions using high-resolution ultrasound equipment (12-MHz electronically focused linear array transducer, iU22; Philips Healthcare, Both- ell, WA, USA), and the lesions were reviewed retrospectively.
The shapes, margins, orientations, echo patterns, and posterior features of the lesions were described according to the ACR-BI- RADS 5th edition lexicon and classifications.
MRI
Preoperative bilateral breast MRIs were performed on 178 le- sions and were retrospectively reviewed. Each patient under- went MRI with a 3T system (Achieva 3T TX or Ingenia 3T CX;
Philips Medical Systems, Best, the Netherlands) with a dedicat- ed 7-channel or 16-channel breast coil (SENSE-Breast 7TX or 16TX; Philips Medical Systems). The magnetic resonance pulse sequences included a three-plane localizing sequence, an axial fat-suppressed T2-weighted fast spin-echo, and an axial fast spoiled 3D gradient-echo T1-weighted non-fat-suppressed se- quence before contrast material administration. The dynamic T1-weighted fat-suppressed three-dimensional fast spoiled gra- dient-echo sequences are then used in the axial plane before and 5 times after intravenous administration of gadobutrol (Gadovist;
Bayer HealthCare, Wayne, NJ, USA) at 0.1 mmol/kg. All col- lected MRI data were processed using a commercially available CAD system (CAD stream software, version 5.2.8.591; Merge Healthcare, Chicago, IL, USA). The morphologies of the masses (shapes, margins, and internal enhancements) were assessed for each lesion according to MRI lexicon of the ACR-BI-RADS 5th edition.
Statistical Analysis
The relationships between all image findings and molecular subtypes were statistically evaluated using the SPSS software (version 20.0; SPSS Inc., Chicago, IL, USA). We used Fisher’s ex- act or the chi-square test to evaluate the qualitative data, and p-
values less than 0.05 were considered statistically significant.
For Fisher’s exact test in contingency table larger than 2 × 2, the data were analyzed using R Core Team (2014): a language and environment for statistical computing (R-3.1.3, R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Clinicopathological Data
All 183 lesions in 176 patients with breast cancer were includ- ed in the analysis (Table 1). Seven patients had bilateral breast cancers at the time of diagnosis. The median age of the patients
Table 1. Clinicopathologic Data for 183 Breast Cancers in 176 Pa- tients
n (%) Clinical symptom
Negative 25 (14)
Lump 147 (80)
Discharge 8 (4)
Lump with discharge 3 (2)
Histology
IDC 23 (12)
IDC + DCIS 124 (68)
DCIS 23 (13)
ILC 2 (1)
Others 11 (6)
Histologic grade
I 23 (13)
II 87 (47)
III 73 (40)
Molecular subtype
Luminal A 79 (43)
Luminal B 42 (23)
HER2 + 19 (10)
Triple negative 43 (24)
Prior breast biopsy for breast cancer*
No 133 (80)
Yes 33 (20)
Family history of breast cancer*
No 138 (81)
Yes 32 (19)
Distant metastasis
No 179 (98)
Yes 4 (2)
*Non-responders were excluded in these categories.
DCIS = ductal carcinoma in situ, HER2 = human epidermal growth factor re- ceptor 2, IDC = invasive ductal carcinoma, ILC = invasive lobular carcinoma
was 37 (range 24–39) years. The tumor was self-discovered in 86% (158/183) of cases. Screening US detected 80% (22/25) of asymptomatic breast cancers; 2 of the remaining 3 were found incidentally during an evaluation for a known contralateral breast cancer and primary occult bone metastasis, and 1 was discov- ered following the observation of suspicious calcification on a
screening mammography (confirmed as DCIS). 80.3% (147/183) of lesions were invasive carcinomas, predominantly IDC ac- companied by DCIS. DCIS alone accounted for 13% of total breast cancers. Most cancers (87%, 160/183) were of a high his- tological grade (II or III). As for tumor subtypes (Table 1), lu- minal A was the most common (43%) (Fig. 1), followed by TN
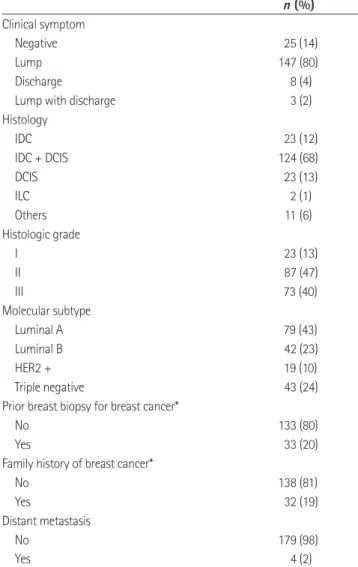
Fig. 1. Luminal A type breast cancer of 37-year-old woman.
A. Right mediolateral oblique mammography shows 2 cm-sized isodense mass with irregular shape and indistinct margin (arrow) on the right lower breast.
B. Ultrasonography shows 2.5 cm-sized hypoechoic mass with irregular shape and indistinct margin (arrows) in the right 6 o’clock direction.
C. Axial contrast-enhanced T1-weighted MR image with fat suppression shows a 2.5 cm-sized heterogeneously enhancing mass with an irregu- lar shape and margin (arrows).
A B C
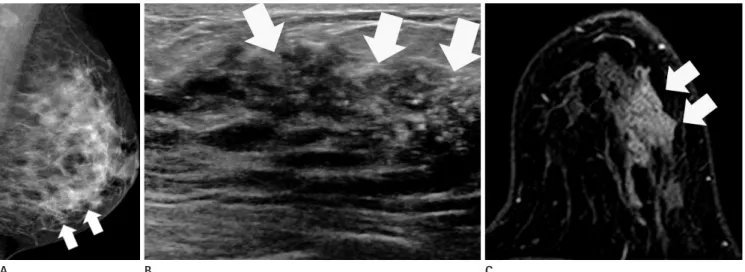
Fig. 2. Triple negative type breast cancer of 37-year-old woman.
A. Right craniocaudal mammography shows 3 cm-sized hyperdense mass with an irregular shape and obscured margin (arrows) on the right outer breast.
B. Ultrasonography shows 3.4 cm-sized hypoechoic mass with an oval shape and circumscribed margin with a posterior enhancement (arrows) in the right 9 o’clock direction.
C. Axial contrast-enhanced T1-weighted MR image with fat suppression shows a 3.5 cm-sized mass with an oval shape, circumscribed margin and rim enhancement (arrows) in the right outer center breast.
A B C
(24%) (Fig. 2), luminal B (23%), and HER2-enriched (10%) (Fig. 3).
Mammography
The most common mammographic feature was a mass with or without calcification (66%) (Table 2). Two thirds of masses (64%) were of a high density, of which a majority had irregular shapes (89%); a plurality (45%) had indistinct margins. TN type cancer frequently showed as a mass with or without calcification (83%) compared to the other types (p = 0.019). Thirty-six percent of lu- minal type A tumors showed indistinct margins (Fig. 1A), while 85% of HER2-enriched type tumors did so, which was signifi- cantly higher than in other tumor types (p = 0.006). Sole calcifi- cation accounted for 18% of tumors.
US
Most breast cancers (98%) were depicted as masses with or without calcification (Table 3). Irregular shapes (86%) and indis- tinct margins (40%) were the most common sonographic find- ings irrespective of the immunohistochemical subtype. The tu- mor showed as a mass with a circumscribed margin in 21% of TN cases, which was more than in any of the other types. How- ever, this was not statistically significant (Fig. 2B). More than half (52%) of the breast cancer masses showed as a hypoechoic lesions on the US overall. However, HER2-enriched type cancer
more often showed a heterogeneous echo pattern (44%) than a hypoechoic pattern (33%) (Fig. 3B). The TN type was found with a posterior enhancement more frequently (49%) than the other immunohistochemical subtypes (p < 0.001) (Table 3).
MRI
The breast cancers were most commonly depicted as an en- hancing mass (80%), with an irregular shape (83%), and irregu- lar margin (56%). The TN type cancer more commonly showed as a mass (93%) when compared to the other types, but this was not statistically significant (Table 4). The degree of background parenchymal enhancement showed an even distribution among all breast cancers and showed no significant differences by tumor types (p < 0.133). Regarding the internal enhancement patterns, a heterogeneous enhancement was the most common (44%).
However, the rim enhancement pattern was the most common finding in TN type tumors (55%, p < 0.001) (Fig. 2C).
DISCUSSION
In this study, we analyzed the clinicopathological and molecu- lar subtypes in young women (under 40 years of age) with breast carcinoma. Most (86%) patients showed self- or clinically-detect- ed symptoms, such as lumps or discharge. Eighty percent of as- ymptomatic patients were diagnosed with breast cancer by US
Fig. 3. Human epidermal growth factor receptor-2 enriched type breast cancer of 38-year-old woman.
A. Left mediolateral oblique mammography shows a 9-cm area of segmental fine linear microcalcifications (arrows).
B. Ultrasonography shows more than 5 cm-sized heterogeneous echoic mass with an irregular shape and calcifications (arrows) in the left 5 o’clock direction.
C. Axial contrast-enhanced T1-weighted MR image with fat suppression shows a 7-cm area of non-mass enhancement with segmental distribu- tion and clustered ring internal enhancement pattern (arrows) on the left lower outer breast.
A B C
screening.
A number of studies have shown that differences in molecular and biologic subtypes may vary by race as a function of age. Col- lins et al. (15) reported in their large cohort study that luminal B type is the most prevalent (35%) in young breast cancer patients compared to the general population. Another study reported that luminal A type was the most common subtype in young breast cancer patients (16). In our series, luminal A subtype was the most common (43%), followed by TN (24%), luminal B (23%), and HER2-enriched (10%) subtypes. Our rate of TN type (24%) was similar in proportion to that previously reported in older and
younger women (11, 17).
Regarding the clinicopathologic correlation, 30% of the DCIS lesions were asymptomatic whereas only 12% of invasive can- cers with or without DCIS were so. Given the high percentages of high-grade and invasive carcinomas in our cohort, concern of unfavorable diagnoses and poor prognoses of breast cancers in younger patients are valid. In many countries, asymptomatic women under 40 years of age are usually not recommended for mammographic breast cancer screening due to the possible hazards of regular exposure to radiation and cost-benefit issues related to having dense breast tissue (18). Furthermore, the Ko- Table 2. Evaluation of Mammographic Features of Breast Cancer under 40 Years Old
Characteristics All (n = 177) Luminal A (n = 76) Luminal B (n = 40) HER2 (n = 19) TN (n = 42) p-Value*
Finding (%) 0.019
Negative 14 (8) 9 (12) 2 (5) 1 (5) 2 (5)
Mass (± calcification) 116 (66) 42 (55) 26 (65) 13 (68) 35 (83)
Calcification only 32 (18) 14 (18) 11 (28) 5 (26) 2 (5)
Others† 15 (8) 11 (14) 1 (3) 0 (0) 3 (7)
Mass (n = 116)
Shape (%) 0.668
Oval/round 13 (11) 6 (14) 3 (12) 0 (0) 4 (11)
Irregular 103 (89) 36 (86) 23 (88) 13 (100) 31 (89)
Margin (%) 0.006
Circumscribed 6 (4) 3 (7) 0 (0) 0 (0) 3 (9)
Obscured 32 (28) 8 (19) 7 (27) 1 (8) 16 (46)
Microlobulated 3 (3) 2 (5) 1 (4) 0 (0) 0 (0)
Indistinct 52 (45) 15 (36) 12 (46) 11 (85) 14 (40)
Spiculated 23 (20) 14 (33) 6 (23) 1 (8) 2 (6)
Density (%) 0.075
High 75 (65) 21 (50) 18 (69) 11 (85) 25 (71)
Equal 41 (35) 21 (50) 8 (31) 2 (15) 10 (29)
Low 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Calcification (n = 81)
Shape (%) 0.399
Round 7 (9) 3 (10) 2 (8) 1 (8) 1 (8)
Amorphous 16 (20) 8 (27) 3 (12) 2 (15) 3 (31)
Coarse heterogeneous 8 (10) 2 (7) 1 (4) 1 (8) 3 (23)
Fine pleomorphic 28 (35) 10 (33) 11 (44) 3 (23) 4 (31)
Fine linear branching 22 (27) 7 (23) 8 (32) 6 (46) 1 (8)
Distribution (%) 0.143
Grouped 40 (49) 12 (40) 14 (56) 5 (38) 9 (69)
Linear 8 (10) 2 (7) 0 (0) 3 (23) 3 (23)
Segmental 13 (16) 5 (17) 6 (24) 2 (15) 0 (0)
Regional 14 (17) 8 (27) 3 (12) 2 (15) 1 (8)
Diffuse 6 (7) 3 (10) 2 (8) 1 (8) 0 (0)
*The p-value was calculated with Fisher’s exact test or Pearson’s chi square test.
†This category includes asymmetry and architectural distortion.
HER2 = human epidermal growth factor receptor 2, TN = triple negative
rean Cancer Association has not recommended mammographic surveillance for women under 40 years of age who are asymp- tomatic. However, a recent evaluation of the National Compre- hensive Cancer Network Breast Cancer Outcomes Database Project revealed that, in women diagnosed with breast cancer at ages under 40 years, symptomatic presentations were more common than mammographic abnormalities, and this was as- sociated with a diagnostic delay (8). It is important to consider the possibility of a malignancy in symptomatic young women while also considering recommending a screening US in asymp- tomatic young women who have a relatively high risk of dis- ease, such as those with a family history of breast cancer.
The mammographic features according to the immunohisto- chemical subtypes have been described in previous studies for all age groups, with significantly more spiculated masses found in
the luminal subgroup (19) and overexpression of HER2-enriched subtype tumors significantly correlated with the presence of cal- cifications (20). Our results were consistent with these data, and the predominance of luminal types could be responsible for the high rate of irregular masses. We observed a relatively low (10%) proportion of HER2-enriched cancers, and only 26% of HER2- enriched tumors manifested as a sole calcification. There was no significant association between the calcification and molecular subtype. However, 68% of HER2-enriched subtype tumors showed calcifications when including the mass with calcification, and this was consistent with a previous report (20).
An US showed a very high sensitivity (98%) for cancer detec- tion, which is consistent with previous reports (21). Only 4 le- sions showed negative findings on US, 3 of which corresponded to sole calcification while 1 showed as a mass with calcification Table 3. Evaluation of Ultrasonography Features of Breast Cancer under 40 Years Old
Characteristics All (n = 183) Luminal A (n = 79) Luminal B (n = 42) HER2 (n = 19) TN (n = 43) p-Value*
Finding (%) 0.211
Mass (± calcification) 179 (98) 78 (99) 40 (95) 18 (95) 43 (100)
Negative 4 (2) 1 (1) 2 (5) 1 (5) 0 (0)
Mass (± calcification) (n = 179)
Shape (%) 0.481
Oval/round 25 (14) 8 (10) 8 (20) 2 (11) 7 (16)
Irregular 154 (86) 70 (90) 32 (80) 16 (89) 36 (84)
Margin (%) 0.478
Circumscribed 24 (13) 11 (14) 3 (8) 1 (6) 9 (21)
Indistinct 71 (40) 30 (38) 18 (45) 9 (50) 14 (33)
Angular 42 (23) 19 (24) 9 (23) 3 (17) 11 (26)
Microlobulated 33 (18) 12 (15) 7 (18) 5 (28) 9 (21)
Spiculated 9 (5) 6 (8) 3 (8) 0 (0) 0 (0)
Orientation (%) 0.095
Parallel 146 (82) 60 (77) 34 (85) 18 (100) 34 (79)
Non-parallel 33 (18) 18 (23) 6 (15) 0 (0) 9 (21)
Echo pattern (%) 0.079
Anechoic 1 (1) 1 (1) 0 (0) 0 (0) 0 (0)
Hyperechoic 2 (1) 2 (3) 0 (0) 0 (0) 0 (0)
Complex cystic and solid 6 (3) 3 (4) 0 (0) 0 (0) 3 (7)
Hypoechoic 93 (52) 41 (53) 21 (53) 6 (33) 25 (58)
Isoechoic 23 (13) 15 (19) 4 (10) 4 (22) 0 (0)
Heterogeneous 54 (30) 16 (21) 15 (38) 8 (44) 15 (35)
Posterior feature (%) < 0.001
Non 114 (64) 56 (72) 33 (83) 7 (39) 18 (42)
Enhancement 46 (26) 14 (18) 5 (13) 6 (33) 21 (49)
Shadowing 13 (7) 6 (8) 1 (3) 3 (17) 3 (7)
Combined 6 (3) 2 (3) 1 (3) 2 (11) 1 (2)
*The p-value was calculated with Fisher’s exact test or Pearson’s chi square test.
HER2 = human epidermal growth factor receptor 2, TN = triple negative
on mammography. Three of these lesions manifested as non- mass enhancements on MRI, and 1 did not undergo MRI. When we consider the correlation between the sonographic findings and molecular subtypes, it is similar to those found in a previous study for all age groups (22). Hormonal receptor negative sub- types, especially the TN subtype, showed more frequent posterior enhancement compared to luminal subtypes on US (23).
The most common abnormal findings on MRI were masses (80%), followed by non-mass enhancements (18%), and foci (2%). In a previous study, young patients under 35 years of age were more likely to display a round/oval or lobular mass shape, a smooth mass margin, and a high signal intensity on T2-weight- ed images when compared to the relatively older patient group
of 35 to 45 year-olds (24). However, our series showed that only 17% of lesions had round or oval shapes, and 29% had circum- scribed margins. Our findings were similar to the results for the older age group (35 to 45 year-olds) in the previous study. How- ever, given the age range of our cohort, there was substantial over- lap in the ages of the both groups that were compared. Addition- ally, TN tumors commonly showed rim enhancement in our study, as in a previous study (25).
Our retrospective study complements many previous studies regarding multimodality imaging findings of breast cancer in two ways. First, the correlation of the imaging features that we observed with certain molecular subtypes was consistent with those reported in other papers. For example, HER2-enriched Table 4. Evaluation of Magnetic Resonance Imaging Features of Breast Cancer under 40 Years Old
Characteristics All (n = 178) Luminal A (n = 76) Luminal B (n = 41) HER2 (n = 18) TN (n = 43) p-Value*
Finding (%) 0.086
Mass 143 (80) 58 (76) 33 (80) 12 (67) 40 (93)
NME 32 (18) 15 (20) 8 (20) 6 (33) 3 (7)
Focus 3 (2) 3 (4) 0 (0) 0 (0) 0 (0)
Mass (n = 143)
Shape (%) 0.618
Oval/round 24 (17) 9 (16) 8 (24) 1 (8) 6 (15)
Irregular 119 (83) 49 (84) 25 (76) 11 (92) 34 (85)
Margin (%) 0.179
Circumscribed 41 (29) 17 (29) 10 (30) 2 (17) 12 (30)
Irregular 80 (56) 27 (47) 18 (55) 9 (75) 26 (65)
Spiculated 22 (15) 14 (24) 5 (15) 1 (8) 2 (5)
Internal enhancement (%) < 0.001
Homogenous 37 (26) 20 (34) 11 (33) 2 (17) 4 (10)
Heterogeneous 63 (44) 31 (53) 13 (39) 5 (42) 14 (35)
Rim 41 (29) 7 (12) 9 (27) 3 (25) 22 (55)
Dark internal septation 2 (1) 0 (0) 0 (0) 2 (17) 0 (0)
NME (n = 32)
Distribution (%) 0.587
Focal 0 (0) 0 (0) 0 (0) 0 (0) 0 (0)
Linear 1 (3) 1 (7) 0 (0) 0 (0) 0 (0)
Segmental 14 (44) 6 (40) 4 (50) 4 (67) 0 (0)
Regional 7 (22) 4 (27) 2 (25) 0 (0) 1 (33)
Multiple regional 3 (9) 2 (13) 0 (0) 1 (17) 0 (0)
Diffuse 7 (22) 2 (13) 2 (25) 1 (17) 2 (67)
Internal enhancement (%) 0.578
Homogenous 6 (19) 3 (20) 3 (38) 0 (0) 0 (0)
Heterogeneous 14 (43) 7 (47) 3 (38) 3 (50) 1 (33)
Clumped 8 (25) 4 (27) 1 (13) 1 (17) 2 (67)
Clustered ring 4 (13) 1 (7) 1 (13) 2 (33) 0 (0)
*The p-value was calculated with Fisher’s exact test or Pearson’s chi square test.
HER2 = human epidermal growth factor receptor 2, NME = non-mass enhancement, TN = triple negative
subtypes more frequently showed indistinct margins than the other subtypes on mammography, and HR-negative subtypes, especially TN, showed more frequent posterior enhancement compared to luminal subtypes on US. Moreover, as stated above, TN tumors commonly showed rim enhancement on MRI. These specific imaging features will enable the identification of mo- lecular subtypes and will be useful in predicting patients’ prog- noses. Second, our study showed a similar distribution of breast cancer subtypes in younger patients as that for older patients in previous reports. In our study, young Korean women were more likely to present luminal A type tumors, as is the case with older patients. However, we also observed relatively more prevalent TN type tumors in young patients than in older individuals, as did previous studies with Korean populations (11, 26). Tumors in young women were more likely to be present with advanced disease and to be of a high grade.
Our study has some limitations, mainly due to its retrospec- tive design and relatively small number of patients. Awareness of known breast cancer patients may have affected the diagnos- tic sensitivities of the mammography, US, and MRI. In addition, a comparison with an older patient cohort for the same time period would have been helpful to more accurately characterize young breast cancer patients. We also did not include sporadic or genetic information, although breast cancer in young patients raises suspicion of BRCA mutations. In fact, we routinely rec- ommend BRCA testing for young women with breast cancer.
However, BRCA information was not available in our electronic medical records.
In conclusion, young women with breast cancer in Korea were more likely to present the luminal A type. The imaging and pa- thologic characteristics of breast cancer in women under 40 years of age were similar to those of older counterparts, as has been previously reported. However, TN type tumors were relatively more prevalent than those previously reported for older patients, and tumors in young women were more likely to be present with advanced disease and to be of a high grade.
Acknowledgments
This research was supported by the Basic Science Research Pro- gram through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT & Future Planning (grant number 2014R1A1A1003355).
REFERENCES
1. Jemal A, Clegg LX, Ward E, Ries LA, Wu X, Jamison PM, et al.
Annual report to the nation on the status of cancer, 1975- 2001, with a special feature regarding survival. Cancer 2004;
101:3-27
2. Ko SS; Korean Breast Cancer Society. Chronological chang- ing patterns of clinical characteristics of Korean breast can- cer patients during 10 years (1996-2006) using nationwide breast cancer registration on-line program: biannual up- date. J Surg Oncol 2008;98:318-323
3. Ahn SH, Son BH, Kim SW, Kim SI, Jeong J, Ko SS, et al. Poor outcome of hormone receptor-positive breast cancer at very young age is due to tamoxifen resistance: nationwide survival data in Korea--a report from the Korean Breast Cancer Society. J Clin Oncol 2007;25:2360-2368
4. Fredholm H, Eaker S, Frisell J, Holmberg L, Fredriksson I, Lindman H. Breast cancer in young women: poor survival despite intensive treatment. PLoS One 2009;4:e7695 5. Prevalence and penetrance of BRCA1 and BRCA2 mutations
in a population-based series of breast cancer cases. Anglian Breast Cancer Study Group. Br J Cancer 2000;83:1301-1308 6. Zhou P, Recht A. Young age and outcome for women with
early-stage invasive breast carcinoma. Cancer 2004;101:
1264-1274
7. Neal RD, Allgar VL. Sociodemographic factors and delays in the diagnosis of six cancers: analysis of data from the “Na- tional Survey of NHS Patients: Cancer”. Br J Cancer 2005;
92:1971-1975
8. Partridge AH, Hughes ME, Ottesen RA, Wong YN, Edge SB, Theriault RL, et al. The effect of age on delay in diagnosis and stage of breast cancer. Oncologist 2012;17:775-782 9. Ruddy KJ, Gelber S, Tamimi RM, Schapira L, Come SE,
Meyer ME, et al. Breast cancer presentation and diagnos- tic delays in young women. Cancer 2014;120:20-25 10. Keegan TH, DeRouen MC, Press DJ, Kurian AW, Clarke CA.
Occurrence of breast cancer subtypes in adolescent and young adult women. Breast Cancer Res 2012;14:R55 11. Park YH, Lee SJ, Jung HA, Kim SM, Kim MJ, Kil WH, et al.
Prevalence and clinical outcomes of young breast cancer (YBC) patients according to intrinsic breast cancer sub- types: single institutional experience in Korea. Breast
2015;24:213-217
12. Hammond ME, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/Col- lege Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and proges- terone receptors in breast cancer. J Clin Oncol 2010;28:
2784-2795
13. Cheang MC, Chia SK, Voduc D, Gao D, Leung S, Snider J, et al. Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J Natl Cancer Inst 2009;101:736- 750
14. American College of Radiology. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. Reston: American College of Radiology, 2013
15. Collins LC, Marotti JD, Gelber S, Cole K, Ruddy K, Kereako- glow S, et al. Pathologic features and molecular phenotype by patient age in a large cohort of young women with breast cancer. Breast Cancer Res Treat 2012;131:1061-1066 16. Tang J, Wu CC, Xie ZM, Luo RZ, Yang MT. Comparison of
clinical features and treatment outcome of breast cancers in young and elderly chinese patients. Breast Care (Basel) 2011;6:435-440
17. Kim EK, Noh WC, Han W, Noh DY. Prognostic significance of young age (<35 years) by subtype based on ER, PR, and HER2 status in breast cancer: a nationwide registry-based study. World J Surg 2011;35:1244-1253
18. Bassett LW, Ysrael M, Gold RH, Ysrael C. Usefulness of mammography and sonography in women less than 35 years of age. Radiology 1991;180:831-835
19. Taneja S, Evans AJ, Rakha EA, Green AR, Ball G, Ellis IO. The mammographic correlations of a new immunohistochemi- cal classification of invasive breast cancer. Clin Radiol 2008;
63:1228-1235
20. Bullier B, MacGrogan G, Bonnefoi H, Hurtevent-Labrot G, Lhomme E, Brouste V, et al. Imaging features of sporadic breast cancer in women under 40 years old: 97 cases. Eur Radiol 2013;23:3237-3245
21. Lehman CD, Lee CI, Loving VA, Portillo MS, Peacock S, DeMartini WB. Accuracy and value of breast ultrasound for primary imaging evaluation of symptomatic women 30-39 years of age. AJR Am J Roentgenol 2012;199:1169-1177 22. Au-Yong IT, Evans AJ, Taneja S, Rakha EA, Green AR, Paish
C, et al. Sonographic correlations with the new molecular classification of invasive breast cancer. Eur Radiol 2009;
19:2342-2348
23. Kojima Y, Tsunoda H. Mammography and ultrasound fea- tures of triple-negative breast cancer. Breast Cancer 2011;
18:146-151
24. Kim JY, Lee SH, Lee JW, Kim S, Choo KS. Magnetic resonance imaging characteristics of invasive breast cancer in women aged less than 35 years. Acta Radiol 2015;56:924-932 25. Uematsu T, Kasami M, Yuen S. Triple-negative breast can-
cer: correlation between MR imaging and pathologic find- ings. Radiology 2009;250:638-647
26. Thapa B, Singh Y, Sayami P, Shrestha UK, Sapkota R, Sayami G. Breast cancer in young women from a low risk popula- tion in Nepal. Asian Pac J Cancer Prev 2013;14:5095-5099
40세 미만 젊은 유방암 환자의 임상적, 병리학적, 영상의학적 특징
김준우
1· 장미정
1* · 김선미
1· 윤보라
1· 이종윤
1· 김은규
2· 강은영
2· 박소연
3목적: 40세 미만의 젊은 유방암 환자의 임상적, 병리학적 소견과 유방촬영, 초음파, 자기공명영상의 영상의학적 소견을 분자아형에 따라 비교 분석하였다.
대상과 방법: 본 연구는 2012년 1월부터 2014년 11월까지 유방암을 진단받은 40세 미만 176명의 여성에게서 발견된 183 개의 병변을 대상으로 하였다. 전체 환자의 임상 및 병리학적 검사는 전자의무기록을 이용하였고 177예의 유방촬영, 183 예의 유방초음파, 178예의 유방자기공명영상 판독소견을 바탕으로 후향적 분석을 수행하였다.
결과: 전체 환자의 86%(183예 중 158예)에서 임상 증상을 통해 자가 진단되었으며 만져지는 종괴(183예 중 147예)가 가 장 흔한 임상 증상이었다. 무증상 환자의 80%(25예 중 22예)는 선별초음파를 통해 진단되었다. 분자아형 중 가장 흔한 것은 luminal A (43%)였으며 triple negative (이하 TN) (24%), luminal B (23%), human epidermal growth factor re- ceptor 2 (이하 HER2) 아형(10%) 순이었다. 영상의학적으로는 HER2 아형이 유방촬영술에서 불분명한 경계를 가진 종 괴로 보였으며, TN 아형이 유방초음파에서의 후방증강소견 및 자기공명영상에서 가장자리의 조영 증강 양상이 특징적으 로 관찰되었다.
결론: 40세 미만의 젊은 유방암 환자에서는 만져지는 종괴가 가장 많았으며 luminal A 아형이 가장 흔했다. 본 연구에서 분자아형별 영상의학적-병리학적 연관성은 40세 이상의 유방암 환자에서 보고된 것과 유사한 결과를 나타내었다.
분당서울대학교병원 1영상의학과, 2외과, 3병리과