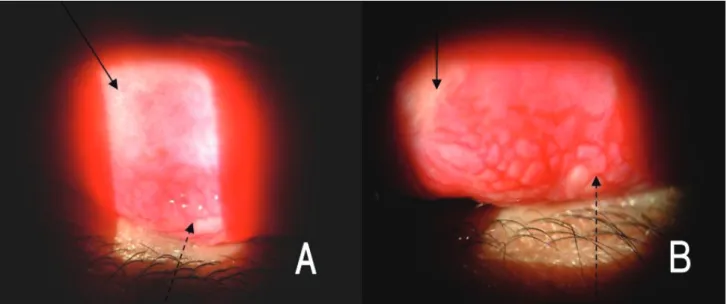
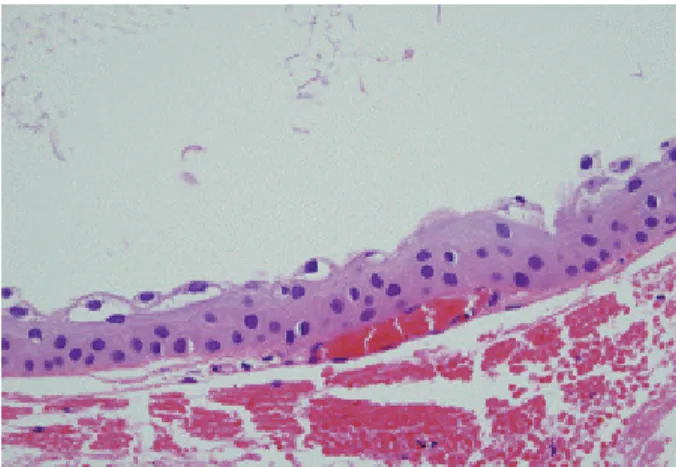
Conjunctival Inclusion Cysts in Long-standing Chronic Vernal Keratoconjunctivitis
4
0
0
전체 글
(2)
(3)
(4)
수치
관련 문서