Received June 18, 2015 Revised August 24, 2015 Accepted August 31, 2015 Corresponding Author Si-Young Park
Tel: +82-42-611-3231, Fax: +82-42-611-3776 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
서 론
인슐린저항성은 혈중 포도당 농도를 정상으로 유지하는데 많은 양의 인슐린이 요구되는 상태로, 인슐린에 대한 세포의 반응 저하나 무반응 상태를 의미한다.1)
1988
년Reaven
등2)이 이들 대사관련 만 성질환의 발생에 있어 인슐린저항성이 중심적인 역할을 하므로 이를 하나의 증후군으로 인식해야 한다고 주장하였는데, 이후 많은 연구 들이 진행되어 인슐린저항성이 심혈관, 대사질환의 발생위험과 연 관이 있음을 보여주었다.2-4)근육은 인슐린이 작용하는 주요 기관 중 하나로 대사증후군뿐 아 니라 당뇨병, 관상동맥질환을 포함한 다양한 심혈관 대사 이상이 근 육량 부족과 연관이 있는 것으로 알려져 있다.5-9) 최근 수년간 시행 된 연구결과에서 근 결핍은 신체기능 이상이나 건강상태, 사망률과 연관이 있었을 뿐 아니라, 당뇨병이나 이상지질혈증, 고혈압과 같은 심혈관 대사 질환 발생에 잠재적인 영향을 미치는 것으로 보고되고
있다.4, 10)
현재 신체 근육량을 측정하는 방법으로 자기공명영상(
MRI
)이나 컴퓨터단층촬영(CT
), 이중에너지 방사선 흡수계측법 (Dual energy
성인남녀에서 생체전기임피던스분석을 이용해 유추한 근육부족량과 인슐린저항성의 연관성
정신아, 최희정, 유건호, 장혜연, 조슬빛, 박시영
*을지대학병원 가정의학과
The association between insufficient muscle mass estimated from bioelectrical impedance analysis and insulin resistance in adults.
Sin-A Jung, Hee-Jeong Choi, Kern-Ho Yu, Hye-Yeon Jang, Sul-Bit Cho, Si-Young Park* Department of Family medicine, Eulji University Hospital
Background: Muscle is one of the primary site for insulin action that plays a role in maintenance of systemic metabolism. Sarcopenia, decrease of muscle mass and strength, occurs by aging and physical inactivity. Several studies have examined the relationship between sarcopenia and physical inability, metabolic disorder, cardiovascular disease in elderly. In this study, we aimed to investigate the association between muscle mass deficit estimated from body composition analysis and insulin resistance in young adults.
Methods: This is a cross-sectional study involving 406 adults aged over 19 to below 65 who visited Health Promotion Center. Physical examinations, bioelectrical impedance analysis and laboratory tests including serum fasting glucose, insulin levels were performed. Partial correlation analysis was done to identify the associated variables of high homeostatic model assessment-insulin resistance(HOMA-IR). Multivariate linear regression analysis was done to identify the major predictors of HOMA-IR. Univariate analysis of variance was used to estimate the corrected means of muscle mass deficit.
Results: HOMA-IR and muscle mass deficit significantly had a positive partial correlation(r=0.243). Insufficient muscle mass had influence on the HOMA-IR after adjusting age, sex, body mass index, waist circumference and other variables(R2=0.501). The corrected means of muscle mass deficit after adjusting variables showed significant difference between two groups, higher in high HOMA-IR(≥2) group than in normal group(P<0.001).
Conclusion: The muscle mass deficit estimated from bioelectrical impedance analysis was a dependent factor affected insulin resistance in adults. This suggests that we can predict the insulin resistance by the muscle mass deficit estimated from body composition analysis.
Keywords: Muscles, Insulin Resistance, bioelectrical impedance analysis
Sin-A Jung, et al. The association between insufficient muscle mass estimated from bioelectrical impedance analysis and insulin resistance in adults
Korean Journal of Family Practice
KJFP
X
-ray absorptiometry
,DEXA
)등이 있으나11, 12), 이들 측정방법은 정확도가 비교적 높은 반면 비용이나 방사선 노출, 접근성 등을 고 려할 때 임상에서 쉽게 사용하기 어렵다는 문제점이 있다. 한편, 체 성분분석은 조직의 생물학적 특성에 따라 다른 전기 전도를 이용한 측정법으로 생체전기임피던스를 분석하여 체지방량이나 골격근량, 체수분량을 유추하는 방법인데 상대적으로 비용이 적게 들며 방사 선 노출이 없고 측정방법도 간단하여 건강진단이나 외래 진료 시에 널리 사용되고 있다.13, 14)최근 우리나라에서도 서구화된 생활 습관이나 운동부족으로 노 인뿐 아니라 젊은 성인에서도 상대적으로 근육량이 적은 경우가 늘 어나고 있고,15) 대사 질환 역시 증가하는 추세이며, 인슐린이 작용 하는 주요 표적기관 중 하나가 근육이라는 점에 착안하여 저자들은 젊은 성인에서 체성분분석을 통해 유추된 근육부족량이 인슐린저 항성과 연관이 있는지 알아보고자 하였다.
연구방법
1. 연구대상
이 연구는
2013
년4
월부터2014
년7
월까지 대학병원 건강증진센 터를 방문한 수진자로InBody 720
을 이용한 체성분분석을 받고, 혈 중 일반화학검사, 인슐린 공복혈당을 측정한 만19
세 이상에서65
세 미만의 성인남녀978
명을 대상으로 하였다. 이 중 간 질환(AST
>
200 IU
/L
또는ALT
>200 IU
/L
)이나 신 질환(eGFR
<60mL
/min
/1
.73m
2)이 의심되는 경우(n
=46
), 당뇨병에 대한 약물치료를 받고 있는 경우(n
=211
), 암의 과거력이 있거나 임신한 경우, 과거 력이나 생활습관(음주, 흡연, 운동) 설문지에 응하지 않은 경우, 기 타 측정항목에 결측치가 있는 경우(n
=315
)를 제외하고 최종적으로406
명을 대상으로 분석하였다.2. 병력, 신체계측 및 혈액검사
모든 대상자에서 자가 기입 설문지와 의사와의 면담을 통해 음 주, 흡연, 운동, 폐경 유무 등을 포함한 생활습관, 과거와 현재병 력, 약물 복용력을 조사하였다. 음주는
1
회 음주량과 주 또는 월 음 주횟수를 조사하였으며National Institute on Alcohol Abuse and Alcoholism
(NIAAA
)에서 제시한 기준에 따라 남성에서1
회5
단위 이상 또는 주15
단위 이상 음주를 하거나 여성에서1
회4
단위 이상 또는 주8
단위 이상 위험 음주를 하는 경우 음주자로 정의하였다.흡연은 금연한 지
6
개월 이내거나 현재 흡연자를 흡연자로 정의하 였다. 운동은1
일20
분 이상 높은 강도 운동을 주3
회 이상 하거나,1
일30
분 이상의 중간 강도 운동과1
일30
분 이상 걷는 정도의 낮은강도 운동을 하는 횟수를 합하여 주
5
회 이상 하는 경우 규칙적인 운동을 하는 것으로 정의하였다.체중과 신장은 얇은 검사용 가운을 입고 양말은 벗은 상태 로 측정하였고, 허리둘레는
WHO
권고방법에 따라 양 발 간격을20
~30cm
벌린 상태로 똑바로 서 체중을 균등하게 분배한 상태에 서 호기 말에 늑골 하단부와 장골능 상부의 중간지점에서0
.1cm
단 위까지 측정하였다. 체질량지수는Quetelet index
를 이용하여 체 중(kg
)을 신장(m
)의 제곱으로 나누어 계산하였다. 혈압은10
분간 휴식을 취한 후 자동혈압측정기(BP
-8800C
,Colin Electronics
,Komaki
,Japan
)를 이용하여5
분 간격으로2
회 측정, 측정치의 평균 을 수진자의 혈압으로 하였다.체성분분석은
InBody 720
(Biospace Co
.,Ltd
,Seoul
,Korea
)를 이용하여 체지방량과 골격근량, 체지방률, 제지방량과 내장지방면 적 등을 측정하였다. 대상자는 검사 전12
시간 이상 공복상태로, 격 렬한 운동이나 음주는 하지 않고, 체성분 측정 전 소변을 보게 한 후, 얇은 검사용 가운을 입고 양말과 전류 흐름에 영향을 주는 금속 류는 모두 제거하고 측정하였다. 생체전기임피던스분석에서 부족 한 근육량은 체성분분석 결과지에 근육조절량으로 표시되는데 이 것은 실제 제지방량과 표준 제지방량의 차이를 나타낸 값을 의미하 며, 우리는 본 연구에서 이 값을 이용하고 근육부족량이라고 표현 하기로 하였다.혈액검사는
12
시간 이상 금식 후 채혈하여3
시간 이내 분석 을 시행하였다. 혈액화학검사는ADVIA 1650 analyzer
(Byer Diagnostics
,Tarrytown
,NY
,USA
)를 이용하여 효소기법 (enzymatic technique
)으로 측정하였고, 저밀도지질단백은 직접 측정방법으로 측정하였다. 혈장 인슐린 농도는ADVIA Centaur XP device
(Siemens Healthcare Diagnostics
,Los Angeles
,CA
,USA
)를 이용하여 화학발광면역측정법(chemi luminescence immunoassays
)으로 측정하였고, 당화혈색소는HLC
-723 G7 machine
(Tosoh Corporation Tokyo
,Japan
)을 이용하여 이온교 환고성능액체크로마토그래피(ion
-exchange high
-performance liquid chromatography
) 방법으로 측정하였다. 인슐린저항성 평 가를 위해 다음의 식을 이용하여 호마지수(homeostasis model assessment of insulin resistance
,HOMA
-IR
)을 계산하였다([공복 인슐린(mIU
/mL
)× {공복혈당(mg
/dL
)/18
.1
}]/22
.5
).3. 통계분석
호마지수
2
.0
을 기준으로2
.0
미만을 정상군으로,2
.0
이상을 인 슐린저항군으로 나누어 분석하였다.3) 각 군에서 일반적 특성의 차 이는 연속형 변수의 경우T
검정, 범주형 변수의 경우 카이제곱 검정을 이용해 비교 분석하였다. 호마지수와 상관성이 있는 변수를 알아보기 위해 연령과 성별, 체질량지수를 보정한 후 편상관분석 을 하였고, 호마지수에 영향을 주는 변수를 찾기 위해 호마지수를 종속변수로 하여 다중회귀분석을 시행하였다. 호마지수 정상군과 인슐린저항군에 해당하는 각각의 근육부족량의 교정평균치를 구 하기 위하여 일변량분산분석을 하였다. 모든 통계분석은
SPSS for windows
(ver
.18
.0
)을 이용하였고, 통계적 유의수준은0
.05
미만으 로 하였다.결 과
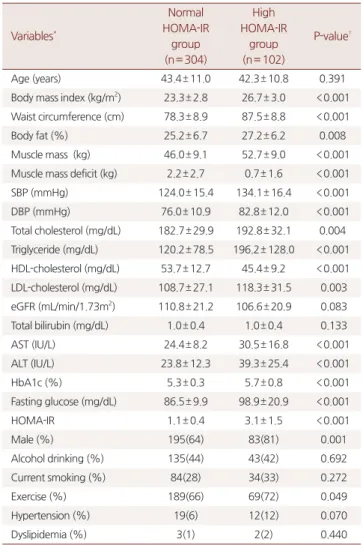
1. 연구대상자의 일반적 특성
연구대상자는 총
406
명으로, 평균나이는43
세 이었다. 호마지수2
.0
을 기준으로 정상이304
명(75
%), 인슐린저항이 있는 대상자는102
명(25
%) 이었다. 두 군 간에 평균 나이는 차이가 없었으나, 인슐 린저항군에서 남성의 비율이 더 높았다. 평균 호마지수는 정상군에 서1
.1
±0
.4
, 인슐린저항군에서3
.1
±1
.5
으로 인슐린저항군에서 높았으나(P
<0
.001
), 평균 근육부족량은 각각2
.2
±2
.7kg
과0
.7
±1
.6kg
으로 인슐린저항군에서 유의하게 낮았다(P
<0
.001
). 인슐린 저항군은 혈중 고밀도지질단백 농도가 유의하게 낮았고(P
<0
.001
), 혈중 총 콜레스테롤(P
<0
.05
), 혈중 저밀도지질단백(P
<0
.05
)과 혈중 중성지방 농도(P
<0
.001
), 허리둘레(P
<0
.001
), 체지방률 (P
<0
.05
), 근육량(P
<0
.001
)은 유의하게 높은 측정치를 보였다. 생 활습관 요인 중 운동이 두 군간에 유의한 차이를 보였다(Table 1
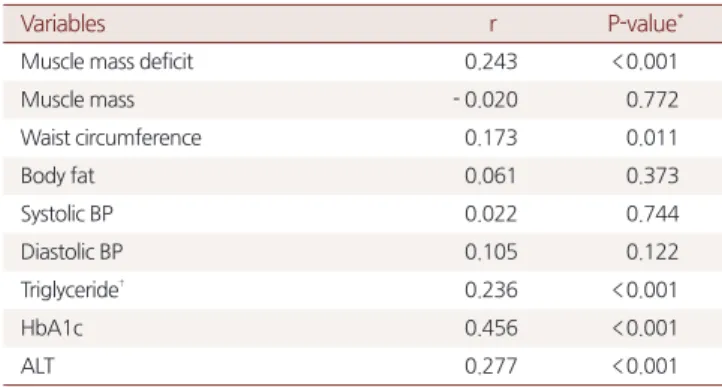
).2. 호마지수와 관련 변수와의 상관성
성별과 나이, 체질량지수를 보정한 후 호마지수는 근육부족량과 유의한 상관관계를 보였고(
r
=0
.243
,P
<0
.001
), 이외에도 허리둘 레(r
=0
.173
,P
=0
.011
), 혈중 중성지방수치(r
=0
.236
,P
<0
.001
), 혈중ALT
(r
=0
.277
,P
<0
.001
)가 호마지수와 유의한 상관관계를 보였다(Table 2
).호마지수에 독립적인 영향을 주는 변수를 결정하기 위해 종속변 수를 호마지수로 하고 성별, 나이, 체질량지수, 허리둘레, 근육부족 량, 당화혈색소, 혈중 중성지방과
ALT
, 생활습관 요인 등을 독립변 수로 하여 다중회귀분석을 한 결과, 나이, 체질량지수, 근육부족량, 당화혈색소,ALT
가 호마지수에 영향을 미치는 변수로 나타났고, 이들 변수가 호마지수를50
.1
% (R2
=0
.501
) 설명할 수 있는 것으로 나타났다(Table 3
).3. 호마지수 각 그룹의 근육부족량의 교정평균치
정상군과 인슐린저항군에 해당하는 각각의 근육부족량의 교정 평균치를 구하기 위해 일변량분산분석을 시행하였다. 근육부족량 에 영향을 끼칠 수 있는 성별과 나이, 체질량지수를 보정한 후 일 변량분산분석을 통한 근육부족량의 교정평균치를 구한 결과, 인슐 린저항군에서 근육부족량의 교정평균치는
2
.2kg
이었던 반면, 정상 군에서는1
.7kg
으로 두 군 간에 유의한 차이를 보였다(P
<0
.001
) (Table 4
).Table 1. General characteristics of the subjects according to normal and high HOMA-IR* groups
Variables*
Normal HOMA-IR
group (n= 304)
High HOMA-IR
group (n= 102)
P-value†
Age (years) 43.4± 11.0 42.3± 10.8 0.391
Body mass index (kg/m2) 23.3± 2.8 26.7± 3.0 <0.001 Waist circumference (cm) 78.3± 8.9 87.5± 8.8 <0.001
Body fat (%) 25.2± 6.7 27.2± 6.2 0.008
Muscle mass (kg) 46.0± 9.1 52.7± 9.0 <0.001 Muscle mass deficit (kg) 2.2± 2.7 0.7± 1.6 <0.001
SBP (mmHg) 124.0± 15.4 134.1± 16.4 <0.001
DBP (mmHg) 76.0± 10.9 82.8± 12.0 <0.001
Total cholesterol (mg/dL) 182.7± 29.9 192.8± 32.1 0.004 Triglyceride (mg/dL) 120.2± 78.5 196.2± 128.0 <0.001 HDL-cholesterol (mg/dL) 53.7± 12.7 45.4± 9.2 <0.001 LDL-cholesterol (mg/dL) 108.7± 27.1 118.3± 31.5 0.003 eGFR (mL/min/1.73m2) 110.8± 21.2 106.6± 20.9 0.083 Total bilirubin (mg/dL) 1.0± 0.4 1.0± 0.4 0.133
AST (IU/L) 24.4± 8.2 30.5± 16.8 <0.001
ALT (IU/L) 23.8± 12.3 39.3± 25.4 <0.001
HbA1c (%) 5.3± 0.3 5.7± 0.8 <0.001
Fasting glucose (mg/dL) 86.5± 9.9 98.9± 20.9 <0.001
HOMA-IR 1.1± 0.4 3.1± 1.5 <0.001
Male (%) 195(64) 83(81) 0.001
Alcohol drinking (%) 135(44) 43(42) 0.692
Current smoking (%) 84(28) 34(33) 0.272
Exercise (%) 189(66) 69(72) 0.049
Hypertension (%) 19(6) 12(12) 0.070
Dyslipidemia (%) 3(1) 2(2) 0.440
Data are shown as the mean±SD for continuous variables and N(%) for categorical variables.
HOMA-IR: homeostasis model assessment of insulin resistance; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein;
LDL: low-density lipoprotein; eGFR: estimated glomerular filtration rate; AST:
aspartate aminotransferase; ALT: alanine aminotransferase; HbA1c: hemoglobin A1c
* High HOMA-IR group is defined as HOMA-IR≥2.0
† P-value by independent t-test for continuous variables and by χ2 test for categorical variables.
Sin-A Jung, et al. The association between insufficient muscle mass estimated from bioelectrical impedance analysis and insulin resistance in adults
Korean Journal of Family Practice
KJFP
고 찰
근육은 이동과 자세유지에 중요한 신체기관 중 하나로, 출생 후
30
세에 이르기까지 성장하고 강해지며 이후 근육의 양과 기능이 점 진적으로 감소한다.16, 17) 근육량은 운동이나 신체활동 수준에 따라 달라지지만, 신체활동수준이 낮은 경우40
대부터70
대에 이르기까지
10
년마다8
%의 근육량 감소가 일어나고 이후부터는 더욱 급속 하게 감소하는 것으로 알려져 있다.17)1989
년Rosenberg
18)에 의해 근결핍증(sarcopenia
)의 개념이 도 입된 이래 노인에서 근육량 감소가 낙상이나 골절 위험을 증가시키 고 장애와 깊은 연관성이 있을 뿐 아니라,19) 비만, 고혈압, 당뇨병, 고지혈증과 같은 대사질환과 심혈관질환과도 연관성이 있다는 연 구결과들이 발표되면서 근결핍증에 대한 중요성이 대두되었다.4, 10) 한편, 이러한 연구 대부분이65
세 이상 노인을 대상으로 이루어져 젊은 성인에서도 같은 결과를 보이는지에 대해서는 알려진 바가 없 다. 이 연구는65
세 미만의 성인 남녀를 대상으로 생체전기임피던 스분석을 통해 유추된 근육부족량이 인슐린저항성과 연관이 있는 지 알아보았고, 노인을 대상으로 한 연구결과와 마찬가지로 근육부 족량은 인슐린저항성의 결정인자로 나타났다.몇몇 유관학회에서 근결핍증을 평가하거나 진단하는 방법에 대 해 제시하고 있으나,20, 21) 아직 표준화된 평가방법이나 진단기준은 없는 실정이다. 비교적 정확하게 근육량을 평가할 수 있는 방법으 로 컴퓨터단층촬영이나 자기공명영상, 이중에너지방사선흡수계측 법 등이 있지만 이들 측정방법은 해당 장비와 더불어 근육량 측정에 필요한 소프트웨어가 있어야 하고, 방사선노출이나 비용에 따른 문 제가 있어 일차진료를 담당하는 의료기관이나 대규모 선별검사에 서 사용하기 어렵다는 문제점이 있다. 생체전기임피던스분석은 빠 르고 간단하게 신체 구성성분을 측정하는 방법으로 일차진료기관 이나 건강증진센터에서 널리 사용되고 있다. 생체전기임피던스분 석을 이용하여 측정한 제지방량은 이중에너지방사선흡수계측법으 로 측정한 근육량과 높은 연관성을 보이는데22-24), 이 연구에서 사용 한 근육조절량 즉, 근육부족량은 측정대상자의 표준체중을 이용하 여 표준 제지방량을 산정한 후 실제 제지방량과의 차이를 계산한 값 이다.
근육량 부족과 인슐린저항성의 연관성은 근육량 감소로 근육에 서 포도당 섭취가 감소하는 것과 단백질의 이화작용을 억제하는 인 슐린의 기능 자체가 근육의 양과 기능을 유지하는데 중요하기 때문 으로 생각할 수 있다.25) 인슐린은 근육에서
GLUT4
를 통해 세포 내 로 포도당이 유입할 수 있도록 하고, 근육은 이렇게 흡수한 포도당 을 이용하여 기능을 할 수 있게 된다. 따라서 근육이 소실되거나 근 육에서 인슐린저항성이 발생하면 당 조절장애를 유발하는 핵심적 인 요인이 될 수 있다.7, 25) 또한 근육소실이 기능저하로 이어져 신체 활동 수준이 더욱 낮아지면 기초대사량이 감소하면서 체지방량이 증가하는 것 또한 인슐린저항성을 유발하는 요인이 될 수 있다.6-8,25) 한편, 체지방량이 증가하면 지방조직에서
TNF
-α
,IL1 and IL6
와 같은 염증성 사이토카인의 분비가 증가하는데 이러한 사이토카 Table 2. Correlations between HOMA IR and metabolic risk factorsVariables r P-value*
Muscle mass deficit 0.243 <0.001
Muscle mass - 0.020 0.772
Waist circumference 0.173 0.011
Body fat 0.061 0.373
Systolic BP 0.022 0.744
Diastolic BP 0.105 0.122
Triglyceride† 0.236 <0.001
HbA1c 0.456 <0.001
ALT 0.277 <0.001
* Adjusted for age, sex, body mass index
† Values are analyzed after natural log-transformation.
HOMA-IR: homeostasis model assessment-estimated insulin resistance; HbA1c:
hemoglobin A1c; ALT: alanine aminotransferase
Table 3. Multivariate regression analyses with HOMA-IR as a dependent variable
R2 B Std. error Beta P*
(constant) Body mass index Muscle mass deficit Age
0.501 - 6.049
0.163 0.090 - 0.016
0.716 0.024 0.026 0.005
0.552 0.257 - 0.176
<0.001
<0.001 0.001 0.001
HbA1c 0.716 0.107 0.368 <0.001
ALT 0.011 0.004 0.161 0.007
sex - 0.066 0.245
Waist circumference 0.184 0.072
Triglyceride† 0.084 0.173
Current smoking - 0.019 0.708
Alcohol drinking - 0.063 0.210
Exercise 0.011 0.831
* Adjusted for age, sex, body mass index, waist circumference, HbA1c, triglyceride, ALT, current smoking, alcohol drinking, exercise
† Values are analyzed after natural log-transformation HbA1c: hemoglobin A1c; ALT: alanine aminotransferase
Table 4. Corrected means of muscle mass deficit according to normal and high HOMA-IR* groups
Variables Average (kg) Std. error P-value† Normal HOMA-IR group
(n= 304) 1.739 0.105 <0.001
High HOMA-IR group
(n= 102) 2.183 0.191 <0.001
* High HOMA-IR group is defined as HOMA-IR≥2.0
† Adjusted for age, sex, body mass index
인은 인슐린저항성을 유발할 뿐 아니라, 근원섬유단백질 분해를 촉 진하고 단백질 합성을 감소시켜 직접적으로 근육 소모를 유발, 근 감소를 더욱 악화시킬 수 있다.26, 27)
대부분 노인을 대상으로 시행된 연구이나, 근 감소와 인슐린저항 성 또는 당뇨병 발생간에 연관성을 보였던 기존의 연구결과들도 이 연구와 유사한 결과를 보고하고 있다.5, 6, 8, 9, 28)
Korean longitudinal study on health and aging
(KLoSHA
) 연구에서는 사지근육량 (appendicular skeletal muscle mass
,ASM
)을 체중으로 나눈 지표 를 이용하여 근 감소를 진단하였을 때 근감소군에서 공복혈당, 인 슐린저항성 지표뿐 아니라, 대사증후군의 유병률이 정상군에 비 해64
.4
%나 높은 것으로 나타났다.28) 또한 미국 국민건강조사(The Third National Health and Nutrition Examination Survey III
) 자 료를 이용하여 분석한 또 다른 연구에서는 골격근량지수(skeletal muscle mass index
)가10
% 증가할 때마다 인슐린저항성이11
% 감 소하고, 체격에 비해 상대적으로 근육량이 많은 경우 인슐린민감도 가 높아지고 전단계 당뇨병의 위험을 낮춘 것으로 나타났다.9) 이 외 에도 근육량이 부족한 경우 인슐린저항성과 당뇨병의 위험이 높아 진다는 몇몇 연구결과가 있었으며5, 6, 8), 근육량이 약간만 증가하여 도 이들 질환의 위험성이 감소하는 용량반응효과를 보여준 결과도 보고되고 있다.29, 30)이 연구의 제한점으로는 첫째, 건강증진센터에 방문한 성인 남녀 를 대상으로 하였기 때문에 선택치우침의 가능성이 있어 이 연구결 과를 일반인에 확대 적용하는데 주의가 필요하다는 것이다. 둘째, 이 연구가 단면연구로 이루어져 근육부족량과 인슐린저항성 간의 인과관계를 추론할 수 없다는 것이다. 셋째, 인슐린저항성을 호마 지수를 이용하여 평가하였고, 단
1
회 측정한 공복혈당과 인슐린농 도를 이용하여 계산하였다는 것이다.결론적으로, 일반 성인에서 체성분분석 결과를 토대로 생체전기 임피던스분석의 근육조절량 즉, 근육부족량이 클수록 호마지수가 증가하였으며 근육부족량 자체가 인슐린저항성의 결정인자임을 보 여주었다. 이러한 결과는 임상에서 체성분분석검사를 하였을 때 제 공되는 변수인 근육부족량을 통해 인슐린저항성을 예측할 수 있을 뿐 아니라, 환자와 상담하거나 교육을 하는데도 유용할 것으로 생 각된다.
요 약
연구배경: 근육은 인슐린이 작용하는 주요 기관중의 하나로 우리 몸의 대사 조절에 관여하고 있으며, 노화와 운동수준에 따라 근육 량과 강도가 감소하는 근결핍증이 발생할 수 있다. 근육량의 감소
는 신체적 기능이상 외에도 대사질환과 심혈관 질환의 연관성이 있 다는 연구결과가 있는데, 이러한 연구들은 대부분 노인들을 대상으 로 시행되었다. 이 연구에서는 젊은 성인남녀를 대상으로 체성분분 석을 통해 측정된 근육부족량과 인슐린저항성의 연관성을 알아보 고자 하였다.
방법: 건강증진센터를 방문한 만
19
세 이상에서65
세 미만의 성인 남녀 중 신체계측과 생체전기임피던스분석을 이용한 체성분분석 및 혈중 공복 혈당과 인슐린을 포함한 검사실 검사를 시행한406
명을 대상으로 하였다. 호마지수(homeostatic model assessment
-insulin resistance
,HOMA
-IR
)와 상관성이 있는 변수를 알아보기 위해 편상관분석을 하였고 호마지수를 예측할 수 있는 변수를 찾기 위해 다중회귀분석을 하였으며, 근육부족량의 교정평균치를 구하 기 위해 일변량분산분석을 하였다.결과: 호마지수는 근육부족량과 유의한 양의 상관관계를 보였다 (
r
=0
.243
). 연령, 성별, 체질량지수, 허리둘레 등을 비롯한 여러 변 수들을 보정하고 근육부족량은 호마지수에 영향을 줄 수 있는 요인 으로 나타났으며 이들 변수가 호마지수를50
.1
% (R2
=0
.501
) 설명 할 수 있었다. 성별과 나이, 체질량지수를 보정한 후 근육부족량의 교정평균치는 인슐린저항군에서 정상군에 비해 높게 나왔으며 두 군간에 유의한 차이가 있었다(P
<0
.001
).결론: 성인 남녀에서 생체전기임피던스분석으로 유추한 근육부족 량은 인슐린저항성에 영향을 줄 수 있는 독립적인 요인임을 알 수 있었다. 이러한 결과는 체성분분석을 통해 근육량 부족이 있는 성 인에서 인슐린저항성을 예측하는데 도움이 될 수 있을 것으로 생각 된다.
중심단어: 근육, 인슐린저항성, 생체전기임피던스분석
REFERENCES
1. Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes 1988;37:1595-607.
2. Reaven GM, Chen YD, Jeppesen J, Maheux P, Krauss RM. Insulin resistance and hyperinsulinemia in individuals with small, dense low density lipoprotein particles. The Journal of clinical investigation 1993;92:141-6.
3. Hedblad B, Nilsson P, Engstrom G, Berglund G, Janzon L. Insulin resistance in non-diabetic subjects is associated with increased incidence of myocardial infarction and death. Diabetic medicine : a
Sin-A Jung, et al. The association between insufficient muscle mass estimated from bioelectrical impedance analysis and insulin resistance in adults
Korean Journal of Family Practice
KJFP
journal of the British Diabetic Association 2002;19:470-5.
4. Karakelides H, Nair KS. Sarcopenia of aging and its metabolic impact. Current topics in developmental biology 2005;68:123-48.
5. Atlantis E, Martin SA, Haren MT, Taylor AW, Wittert GA, Members of the Florey Adelaide Male Ageing S. Inverse associations between muscle mass, strength, and the metabolic syndrome. Metabolism:
clinical and experimental 2009;58:1013-22.
6. Dominguez LJ, Barbagallo M. The cardiometabolic syndrome and sarcopenic obesity in older persons. Journal of the cardiometabolic syndrome 2007;2:183-9.
7. Mohammad E K, Mojtaba M, Rokhsareh A, Zahra E. Sarcopenia and diabetes: pathogenesis and consequences. Br J Diabetes Vasc Dis 2011;11:230-4.
8. Srikanthan P, Hevener AL, Karlamangla AS. Sarcopenia exacerbates obesity-associated insulin resistance and dysglycemia: findings from the National Health and Nutrition Examination Survey III.
PloS one 2010;5:e10805.
9. Srikanthan P, Karlamangla AS. Relative muscle mass is inversely associated with insulin resistance and prediabetes. Findings from the third National Health and Nutrition Examination Survey. The Journal of clinical endocrinology and metabolism 2011;96:2898- 903.
10. Janssen I. Evolution of sarcopenia research. Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme 2010;35:707-12.
11. Mitsiopoulos N, Baumgartner RN, Heymsfield SB, Lyons W, Gallagher D, Ross R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. Journal of applied physiology 1998;85:115-22.
12. Wang ZM, Visser M, Ma R, et al. Skeletal muscle mass: evaluation of neutron activation and dual-energy X-ray absorptiometry methods. Journal of applied physiology 1996;80:824-31.
13. Nunez C, Gallagher D, Grammes J, et al. Bioimpedance analysis:
potential for measuring lower limb skeletal muscle mass. JPEN Journal of parenteral and enteral nutrition 1999;23:96-103.
14. Pietrobelli A, Morini P, Battistini N, Chiumello G, Nunez C, Heymsfield SB. Appendicular skeletal muscle mass: prediction from multiple frequency segmental bioimpedance analysis. European journal of clinical nutrition 1998;52:507-11.
15. Park SH, Jang SY, Kim H, Lee SW. An association rule mining- based framework for understanding lifestyle risk behaviors. PloS one 2014;9:e88859.
16. Aoyagi Y, Shephard RJ. Aging and muscle function. Sports medicine 1992;14:376-96.
17. Grimby G, Saltin B. The ageing muscle. Clinical physiology 1983;3:209-18.
18. Rosenberg IH. Sarcopenia: origins and clinical relevance. The Journal of nutrition 1997;127:990S-1S.
19. Scott D, Hayes A, Sanders KM, Aitken D, Ebeling PR, Jones G.
Operational definitions of sarcopenia and their associations with 5-year changes in falls risk in community-dwelling middle-aged and older adults. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA 2014;25:187-93.
20. Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiology of sarcopenia among the elderly in New Mexico. American journal of epidemiology 1998;147:755-63.
21. Janssen I, Heymsfield SB, Baumgartner RN, Ross R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. Journal of applied physiology 2000;89:465-71.
22. Ling CH, de Craen AJ, Slagboom PE, et al. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clinical nutrition 2011;30:610-5.
23. Malavolti M, Mussi C, Poli M, et al. Cross-calibration of eight- polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21-82 years. Annals of human biology 2003;30:380-91.
24. Wi YS, Swearingin B, Crooms.B., Lee R, Choi Y, Dail T. Body composition measurements determined by air displacement plethysmography and eight-polar bioelectrical impedance analysis are equivalent in African American college students. HealthMed 2012;6:1896.
25. Baron AD, Brechtel G, Wallace P, Edelman SV. Rates and tissue sites of non-insulin- and insulin-mediated glucose uptake in humans. The American journal of physiology 1988;255:E769-74.
26. Fong Y, Moldawer LL, Marano M, et al. Cachectin/TNF or IL-1 alpha induces cachexia with redistribution of body proteins. The American journal of physiology 1989;256:R659-65.
27. Lang CH, Frost RA, Nairn AC, MacLean DA, Vary TC. TNF- alpha impairs heart and skeletal muscle protein synthesis by altering translation initiation. American journal of physiology Endocrinology and metabolism 2002;282:E336-47.
28. Kim JH, Choi SH, Lim S, et al. Assessment of appendicular skeletal muscle mass by bioimpedance in older community-dwelling Korean adults. Archives of gerontology and geriatrics 2014;58:303- 7.
29. Izumiya Y, Hopkins T, Morris C, et al. Fast/Glycolytic muscle fiber growth reduces fat mass and improves metabolic parameters in obese mice. Cell metabolism 2008;7:159-72.
30. Walsh K. Adipokines, myokines and cardiovascular disease.
Circulation journal : official journal of the Japanese Circulation Society 2009;73:13-8.