Address reprint requests to Jong-Beom Park, M.D.
Department of Orthopedic Surgery, Uijongbu St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Korea
# 65-1 Kumho-dong, Uijongbu-city, Kyunggi-do, 480-130, Korea
Tel : 82-351-820-3048, Fax : 82-351-847-3671, E-mail : [email protected]
Os odontoideum과 환축추 불안정성이 있는 환자의 횡인대에 발생한 활막 낭종
- 증례보고 -
장장한・박종범・김기원*・박원종・김승기・최우성・권영정
가톨릭대학교 의과대학 의정부성모병원, 성모병원* 정형외과학교실
– Abstract –
Synovial Cyst of Transverse Ligament of Axis in a Patient with Os Odontoideum and Atlantoaxial Instability : A Case Report
Han Chang, M.D., Jong-Beom Park, M.D., Ki-Won Kim, M.D.*, Won-Jong Bahk, M.D., Seung-Key Kim, M.D., Woo-Sung Choi, M.D. and Young-Jeong Kwon, M.D.
Department of Orthopedic Surgery, Uijongbu St. Mary’s Hospital & St. Mary’s Hospital*, College of Medicine, The Catholic University of Korea, Korea
Study Design : A case report and review of the literature.
Objectives : To describe the diagnosis and successful treatment of the synovial cyst arising from the transverse ligament in a patient with Os odontoideum and atlantoaxial instability.
Summary of Literature Review : Synovial cyst arising from the transverse ligament of the axis is extremely rare and thought to be attributed to degenerative changes of the C1-C2 facet joints or microtraumas. Direct excision of the cyst is the only treatment method described in previous reports.
Materials and Methods : A case of synovial cyst arising from the transverse ligament of the axis in a 45-year-old man with Os odontoideum and atlantoaxial instability was managed with posterior atlantoaxial fusion alone. The characteristic MRI findings and surgical treatment, and related literature are reviewed.
Results : MRI of the cervical spine showed a large cystic mass located at the transverse ligament of the axis which was com- pressing the spinal cord near the C1-C2 junction: the images showed a low signal intensity on T1WI; high signal intensity on T2WI; and rim enhancement with no internal enhancement on Gadolinium enhanced T1WI. The spontaneous resolution of the cyst was identified on the follow-up MRI taken at 3 months after operation and clinical improvement was achieved.
Conclusions : The MRI findings of spontaneous resolution of synovial cyst arising from the transverse ligament of the axis after posterior atlantoaxial fusion alone suggest that stable fusion rather than direct excision of the cyst should be considered over the surgical option when the location of the cyst is difficult or dangerous to approach surgically.
Key Words : Os odontoideum, Atlantoaxial instability, Synovial cyst, Atlantoaxial fusion, Spontaneous resolution
Journal of Korean Spine Surg.
Vol. 6, No. 1, pp 151~156, 1999
서 론
척추에서 발생하는 활막 낭종의 대부분은 후관절의 과도한 운동이나 불안정성에 의한 퇴행성 변화 또는 미세한 외상과 연관되어8, 9, 12, 20) 하부 요추, 요천추 및 하부 경추의 후관절에 인접하여 발생하며4, 6, 7, 15, 16, 19,
22, 24), 환축추 관절을 포함한 상부 경추의 경우는 현재
까지 1 3례2, 4, 6, 7, 15, 16, 19, 22, 24)만이 보고될 정도로 극히 드물게 발생하는 것으로 보고되고 있다. 저자들은 현재
까지 문헌상 보고된 바 없는 환축추 불안정성을 동반 한 Os odontoideum 환자의 횡인대에 병발된 활막 낭 종에 대해 직접적인 낭종 제거술을 시행하지 않고 환 축추 후방 유합술로 환축추 관절의 불안정성을 제거한 후 추시 관찰중 이의 자연 소실을 자기공명영상 검사 로 확인하였기에 문헌 고찰과 함께 보고하고자 한다.
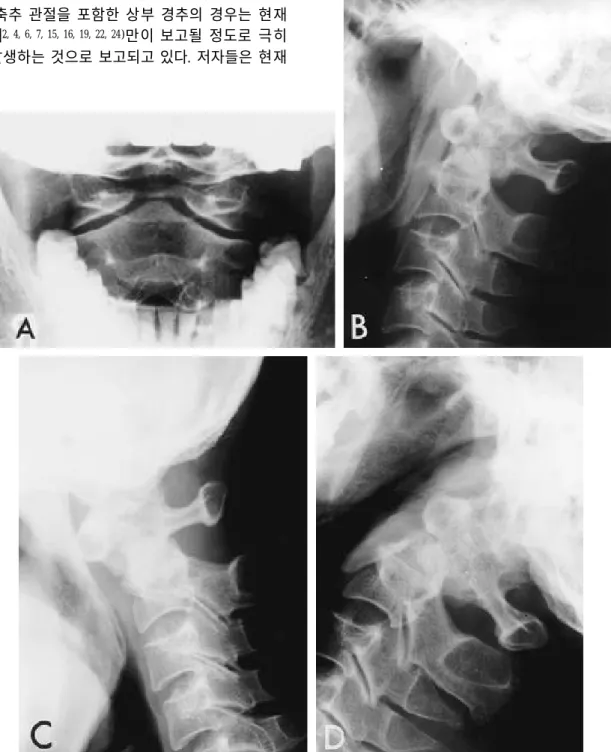
Fig. 1. A and B, Open mouth view and lateral radiograph of the cervical spine showing a small, round ossicle located above the C1-C2 facet joints with a wide gap between ossicle and axis body. C and D, Flexion and extension lateral radiographs of the cervical spine showing a severe anterior and posterior atlantoaxial instability.
증례 보고
4 5세 남자로 내원 2개월전 교통 사고후 발생한 좌 측 상지의 감각 이상 및 근력 약화를 주소로 내원하 였다. 내원당시 시행한 이학적 검사상 좌측 상지의 제6, 7, 8 경추 신경근 지각 영역의 감각이상과 G o o d 정도로 근력이 약화된 소견을 나타내었다. 경추부 전 후방 단순 방사선 및 개구 전후방 검사상 환축추 후 관절의 상방에 작고 둥근 소골이 존재하면서 이 소 골과 축추체와의 사이에 넓은 간격을 보였다(Fig. 1- A, B). 굴곡 및 신전 측면 방사선 검사상 환추의 전, 후방 이동거리는 1 6㎜, 불안정 지수는 40.74, 환축추 각도는 2 0도로 환축추 관절의 심한 전,후방 불안정성 소견을 나타내었다2 3 )(Fig. 1-C,D). 경추부 자기공명 영상 검사의 시상면 및 축상면 T1 강조 영상에서 둥 글고 경계가 명확하며 척수액과 비슷한 저신호 강도 를 보이는 낭종성 종물이 축추체 후연의 십자 인대 에 존재하면서(Fig. 2-A), T2 강조 영상에서 고신호 강도를 보이고(Fig. 2-B), Gadolinium 조영 증강 T 1 강조 영상에서 종물의 내부를 제외하고 가장자리만 조영 증강되는 낭종 소견을 나타내었다(Fig. 2-C).
저자들은 환축추 관절의 불안정성에 의한 추가적인 신경 손상을 예방하기 위하여 강선을 이용한 R o g e r 씨 환축추 후방 유합술을 시행하였다. 수술 직후 신
경학적 변화는 보이지 않았으며 Minerva cast를 이 용하여 외고정을 시행하였다. 술후 3개월에 시행한 단순 방사선 검사상 견고한 골유합 소견(Fig. 3)을 나타내고 추시 자기공명영상 검사상 낭종성 종물이 Fig. 2. A, Sagittal T1-weighted image showing a small, round, and well demarcated low signal intensity cystic mass (white arrow) located at the transverse ligament of the axis. B, Sagittal T2-weighted image showing a cystic mass (black arrow) of high sig- nal intensity. C, Sagittal Gadolinium-enhanced T1-weighted image showing a rim enhancement of the cystic mass with no internal enhancement (black arrow).
Fig. 3. At postoperative 3 months, lateral radiograph of the cer- vical spine showing a solid bony union of the atlantoax- ial fusion mass.
자연 소실(Fig. 4-A, B)되어 Minerva cast를 제거하 였다. 술후 1 2개월 최종 추시시 좌측 상지의 근력은 N o r m a l로 회복되었지만 제6, 7, 8 경추 신경근 지각 영역의 감각이상은 약간 남아 있었다.
고 찰
하부 요추, 요천추 및 하부 경추의 후관절에 인접 하여 주로 발생하는 활막 낭종은 과거에는 드물게 보 고되었으나, 최근 컴퓨터 단층촬영 및 자기공명영상 등의 진단 방법이 발달하면서 이에 대한 보고가 증가 하고 있다3, 5, 11, 16-18). 이의 원인은 현재까지 정확히 밝혀지지는 않았으나 후관절의 운동이 가장 많이 일 어나는 부위에서 주로 발생하고 퇴행성 척추 전방 전 위증과 연관이 있는 것으로 미루어 후관절의 퇴행성 변화 또는 이에 대한 반복적인 미세한 외상이 중요한 원인일 것이라고 추측하고 있다8, 9, 12, 20). Kao 등1 1 )은 척수내“j u x t a - f a c e t”낭종을 조직학적 차이에 따라 활막 낭종과 결정성 낭종으로 구분하였지만, 임상적 으로 의미있는 차이를 보이지 않기 때문에 혼용하여 사용되고 있다.
단순 방사선 검사로 활막 낭종에 대한 진단은 불가
능하며, 척수강 조영술에서는 경막외 결손으로 나타 날 수 있지만 추간판 탈출증과의 감별이 어렵고 감 수성 및 특이성이 떨어지는 단점이 있다1, 3, 9). 컴퓨 터 단층촬영은 낭종성 종물을 명확히 나타낼 수 있 고 낭종내에 존재하는 가스 음영이나 낭종의 벽에 존재하는 석회화 음영이 나타나는 경우에는 진단을 내릴 수 있다1 2 ). 자기공명영상은 T1 강조 영상에서 척수액과 유사한 저신호 강도를 나타내는 낭종성 종 물이 T2 강조 영상에서 고신호 강도를 나타내고 Gadolinium 조영 증강 T1 강조 영상에서 낭종의 내 부를 제외하고 가장자리만 조영 증강되는 특징적인 소견을 나타낼 경우 활막 낭종으로 진단할 수 있다
1 0 , 1 2 , 1 5 , 1 9 , 2 0 ). 본 증례의 경우도 이러한 활막 낭종의 특
징적인 자기공명영상 소견을 나타내어 Os odon- t o i d e u m에 의한 환축추 관절의 전,후방 불안정성에 의해 축추체 후연의 횡인대에 발생한 활막 낭종으로 진단할 수 있었지만, 이와 유사한 소견을 나타내는 수막종(meningioma), 경막외 농양, 지주막 낭종 (arachnoid cyst)등 낭종성 종양 및 환축추 관절의 만성적인 아탈구와 연관되어 발생할 수 있는 위종양 등과의 감별 진단이 반드시 고려되어야 한다4 , 1 4 , 1 8 , 2 1 ). 수막종의 경우 Gadolinium 조영 증강 T1 강조 영상 에서 낭종의 내부까지도 광범위하게 조영 증강되는 Fig. 4. A and B, At postoperative 3 months, follow-up sagittal T1- and T2-weighted images showing
spontaneous resolution of the cystic mass, but intramedullary high signal intensity(white arrow) still remained at C1-2 junction.
소견으로, 섬유성 조직인 위종양의 경우 T1 및 T 2 강조 영상에서 저신호 또는 중간 신호를 보이는 소 견으로, 지주막 낭종의 경우 후관절의 퇴행성 변화없 이 척추경과 후궁을 침범하여 얇게 하는 ( t h i n n i n g ) 소견으로 각각 활막 낭종과 감별될 수 있다.
하부 요추, 요천추 및 하부 경추에서 발생한 활막 낭종의 대부분은 후궁 절제술후 낭종에 대한 직접적 인 제거술을 시행하여 척추의 안정성에 손상을 주지 않으면서도 만족할 만한 결과를 얻을 수 있지만, Hemminghytt 등8 )과 Hsu 등9 )은 증상이 있는 요추 의 활막 낭종에서 휴식 및 보조기를 이용한 외고정 만으로도 낭종의 자연 감소와 증상의 회복을 얻었다 고 보고하였다.
현재까지 상부 경추에서 보고된 1 3례의 활막 낭종 중 1례를 제외한 1 2례가 축추체 후연의 횡인대에서 발생하였고2, 4, 6, 7, 15, 16, 19, 22) 이중 1례를 제외한 1 1례 에서 단순 방사선 검사상 환축추 관절의 불안정성 없 이 후관절의 퇴행성 변화 소견을 나타냈다. 이들에 대 한 수술적 치료로는 1례는 후외측 도달법으로6 ), 3례 는 경구강 도달법으로2 , 4 , 1 2 ), 나머지 9례는 환추의 후궁 절제술후 직접적인 낭종 제거술을 시행하여 1 3례 모 두에서 만족할만한 결과를 얻었다고 보고하였다. 특 히 경구강 도달법으로 직접적인 낭종 제거술을 시행 한 3례중 1례만이 추가적으로 후방 유합술을 시행하 였고, 술전 단순 방사선 검사상 환축추 아탈구를 보였 던 1례를 포함한 2례에서는 후방 유합술을 시행하지 는 않았지만 추시 결과 환축추 불안정성을 나타내지 않았다고 보고하였다. 이에 비해 저자들은 본 증례의 경우는 Os odontoideum에 의한 환축추 관절의 심한 전,후방 불안정성으로 인한 횡인대의 퇴행성 변화로 이에 병발된 활막 낭종으로 판단하였으나, 일차적으 로 Os odontoideum에 의한 환축추 관절의 불안정성 에 대하여 후방 유합술을 시행하고 활막 낭종에 대하 여는 환자의 증상과 추시 자기공명영상의 소견에 따 라 이차적인 낭종 제거술의 시행 여부를 결정하기로 하였다. 이에 R o g e r씨 환축추 후방유합술을 시행하였 고 추시 관찰중 좌측 상지의 감각 이상 및 약화되었 던 근력의 회복을 보였고 술후 3개월에 추시한 자기 공명영상 검사에서 활막 낭종의 자연 소실이 확인되 었다. 술후 1 2개월 최종 추시시 좌측 상지의 근력은 N o r m a l로 회복되었고 제6, 7, 8 경추 신경근 지각영 역의 감각 이상은 약간 남아 있는 상태이다.
결론적으로 저자들은 현재까지 문헌상 보고된 바 없는 환축추 불안정성을 동반한 Os odontoideum 환 자의 횡인대에 병발된 활막 낭종을 보고한다. 또한 직접적인 낭종 제거술을 시행하지 않고 환축추 후방
유합술로 활막 낭종의 자연 소실을 자기공명영상 검 사로 확인할 수 있었다. 따라서 수술적으로 도달하기 어려운 부위에 발생한 활막 낭종의 경우에는 직접적 인 제거술보다는 견고한 유합술을 반드시 고려해야 할 것으로 보이며 추시 자기공명영상 검사로 낭종의 진행여부를 확인하는 것이 필요하다고 판단된다.
REFERENCES
11) Baum JA and Hanley Jr ED : Intraspinal Synovial Cyst Simulating Spinal Stenosis. A case Report. Spine, 11:187- 189, 1986.
12) Birch BD, Khandeji AG and McCormick PC : A t l a n t o a - xial degenerative articular cysts. J Neurosurg, 85:810-816, 1 9 9 6 .
13) Cartwright MJ, Nehls DG, Carrion CA and Spetzier RF : Synovial cyst of a cervical facet joint. case report.
Neurosurgery, 16:850-859, 1985.
14) Choe W, Walot I, Schlesinger C, Chambi I and Lin F : Synovial cyst of dens causing spinal cord compression. Case report. Paraplegia, 31:803-807, 1993.
15) Epstein NE and Hollingsworth J : Synovial Cyst of the Cervical Spine. Case Report. J Spinal Disord, 6:182-185, 1993.
16) Fransen P, Pizzolato GP, Otten P, Reverdin A, Lagier R and Tribolet ND : Synovial cyst and degeneration of the transverse ligament: an unusual cause of high cervical myelopathy. J Neurosurg, 86:1027-1030, 1997.
17) Goffin J, Wilms G, Plets C, Bruneel B and Casselman J : Synovial Cyst at the C1-C2 Junction. Neurosurgery, 30:914-916, 1992.
18) H e m m i n g h y t t S , D a n i e l s D L , W i l l i a m s A L a n d Haughton VM : Intraspinal synovial cyst: natural history and diagnosis by CT. Radiology, 145:375-376, 1982.
19) Hsu KY, Zucherman JF, Shea WJ and Jeffrey RA : Lumbar Intraspinal Synovial and Ganglion Cysts(Facet Cysts). Ten-Year Experience in Evaluation and Treatment.
Spine, 20:80-89, 1995.
10) Jackson DE Jr, Atlas SW, Mani JR and Norman D : Intraspinal Synovial Cysts: MR Imaging. Radiology, 170:
527-530, 1989.
11) Kao CC, Winkler SS and Turner JH : Synovial cyst of spinal facet. J Neurosurg, 41:372-376, 1974.
12) Kaufmann AM, Halliday WC, West M, Fewer D and Ross I : Periodontoid Synovial Cyst Causing Cervico-
medullary Compression. Can J Neurol Sci, 23:227-230, 1996.
13) Liu SS, Williams KD, Drayer BP, Spetzler RF and Sonntag VKH : Synovial Cysts of the Lumbosacral Spine:
Diagnosis by MR Imaging. Am J Neuroradiol, 10:1239- 1242, 1989.
14) Mercader J, Munoz GJ and Cardenal C : I n t r a s p i n a l synovial cyst: diagnosis by CT. Follow up and spontaneous remission. Neuroradiology, 27:346-348, 1985.
15) Miller AD, Al-Mefty O and Middleton TH : S y n o v i a l cyst at the craniovertebral junction. Surg Neurol, 31:239- 242, 1989.
16) Onofrio BM and Mih AD : Synovial Cysts of the Spine.
Neurosurgery, 22:642-647, 1988.
17) Patel SC and Sander WP : Synovial cyst of the cervical spine: case report and review of the literature. Am J Neu- roradiol, 9:602-603, 1988.
18) Pendleton B, Carl B and Pollay M : Spinal extradural benign synovial or ganglion cyst: case report and review of the literature. Neurosurgery, 13:322-326, 1983.
19) Quaghebeur G and Jeffree M : Synovial cyst of the high cervical spine causing myelopathy. Am J Neuroradiol, 13:
981-982, 1992.
20) Silbergleit R, gebarski S, Brunberg J, McGillicudy J and Blaivas M : Lumbar synovial cyst: correlation of myelographic CT, MRI, and pathologic findings. Am J Neuroradiol, 11:777-779, 1990.
21) Sze G, Brant-Zawadzki Mn, Wilson CR and Newton TH : Pseudotumor of the craniovertebral junction associ - ated with chronic subluxation: MR imaging studies.
Radiology, 161:391-340, 1986.
22) Vergne P, Bonnet C, Zabraniecki L, Bertin P, Moreau JJ and Treves R : Synovial Cyst at the C1-C2 Junction and Spondyloarthropahty. J Rheumatol, 23:1438-1440, 1996.
23) Watanabe M, Toyama Y and Fujimura Y : Atlantoaxial Instability in Os odontoideum with Myelopathy. Spine, 21:
1435-1439, 1996.
24) Weymann CA, Capone P, Kinkel PR and Kinkel WR : Synovial cysts of the upper cervical spine: MRI with gado- linium. Neurology, 43:2151-2152, 1993.
연구 계획 : 증례 보고 및 문헌 고찰
연구 목적 : Os odontoideum과 환축추 불안정성이 있는 환자의 횡인대에 발생한 활막 낭종의 진단 및 치료를 기술 하고자 한다.
대상 및 방법 : Os odontoideum과 환축추 불안정성이 있는 4 5세 남자 환자의 횡인대에 발생한 활막 낭종에 대해 환축추 후방 유합술만을 시행후 추시 관찰하였다. 그리고 활막 낭종의 특징적인 자기공명영상 소견, 수술적 치료 및 문헌 고찰을 기술하였다.
결과 : 경추부 자기공명영상 검사의 T1 강조 영상에서 둥글고 경계가 명확하며 척수액과 비슷한 저신호 강도를 보 이는 낭종성 종물이 축추체 후연의 십자 인대에 존재하면서, T2 강조 영상에서 고신호 강도를 보이고, Gadolinium 조영 증강 T1 강조 영상에서 종물의 내부를 제외하고 가장자리만 조영 증강되는 활막 낭종의 소견을 나타내었다.
환축추 후방 유합 술후 3개월에 시행한 추시 자기공명영상 검사상 낭종의 자연 소실이 확인되었다.
결론 : 저자들은 현재까지 문헌상 보고된 바 없는 환축추 불안정성을 동반한 Os odontoideum 환자의 횡인대에 병 발된 활막 낭종을 보고한다. 또한 직접적인 낭종 제거술을 시행하지 않고 환축추 후방 유합술로 활막 낭종의 자연 소실을 자기공명영상 검사로 확인할 수 있었다. 따라서 수술적으로 도달하기 어려운 부위에 발생한 활막 낭종의 경 우에는 직접적인 제거술보다는 견고한 유합술을 반드시 고려해야 할 것으로 보이며 추시 자기공명영상 검사로 낭 종의 진행여부를 확인하는 것이 필요하다고 판단된다.
색인단어: Os odontoideum, 환축추 불안정성, 활막 낭종, 환축추 유합술, 자연 소실 국 문 초 록
※ 통신저자 : 박 종 범
경기도 의정부시 금오동 65-1
가톨릭대학교 의과대학 의정부성모병원 정형외과학교실
Tel : 82-351-820-3048, Fax : 82-351-847-3671, E-mail : [email protected]