VOLUME 14, NUMBER 4, December 2009
Afferent Arteriovenous Anastomosis For Finger Tip Replantation
Soon-ho Hwang, MD
Department of Orthopaedic Surgery Kang-Nam Jungang Hospital
Purpose: The vessels of the finger tip are very small and fragile, have many branches, so the anastomosis of this vessel is very difficult. Guillotine type amputation of digits are rare, on the other hand, crush/avulsion injuries which require complex surgical solutions are more fre- quent. We often found that the arteries of distal amputee on crush/avulsion injuries are lost. In these cases, replan- tation is much more difficult even impossible. But when replantation is successes, the replantated finger tip pro- vides adequate soft tissue, restoration of length, sensory and nail.
Materials and Methods: We report here our experi- ence of finger tip replantation using afferent a-v anasto- mosis technique accumulated from March 2006 to March 2009.
Result: The success rate was 96.4%. Complications occurred in eight patients. (5 digit atrophy, 1 osteomyelitis, 1 severe digit pain and 1 cold intolerance)
Conclusions: We believe that the afferent a-v anasto- mosis replantation provides us wider range of indication of finger tip replantation on crush/avulsion injuries.
(J Korean Soc Hand Surg 2009;14:161-6)
Key Words: Finger tip, Replantation, Afferent arteriove- nous anastomosis
서 론
수지 첨부는 동맥의 크기가 작아 문합에 적당한 혈 관을 찾기가 힘들어 재접합이 어려운 것으로 알려져 있으며 수술 전후 혈관 수축과 혈전 형성이 빈번하여 성공률이 낮게 보고 되어 왔다1,2. 특히 압궤상 및 견열 손상의 경우 원위 절단부의 동맥이 소실되는 경우가 대부분이이서 재접합이 불가능한 경우를 흔히 접하게 된다. 수지 첨부 절단의 경우 재접합이 어려운 술식이 기는 하나 일반적으로 시행되는 단단성형술에 비해 길 이의 유지, 감각복원, 조갑보존, 기능상의 장점 등 여 러 장점이 있어 수지 첨부 재접합술의 중요성이 강조 되고 있다. 저자들은 압궤상, 견열손상 등으로 원위절 단부 동맥이 소실된 경우에 있어 Nakayama3 등에 의해 소개된 유리 동맥과 정맥피판의 개념을 도입하여 근위 절단부의 동맥과 원위 절단부의 정맥을 연결하는 동정맥문합을 이용한 Yamano1 혈관분류 Zone I, II 의 수지첨부 재접합술을 시행하였으며 이에 대해 문헌 고찰과 함께 보고 하고자 한다.
재료 및 방법
가. 대상
2006년 3월부터 2009년 3월 까지 동정맥문합술을 이용한 Yamano1 혈관분류 Zone I, II의 수지접합술 을 시행한 28예를 대상으로 하였다. 남자가 21명 여자 가 7명 이었으며 환자 연령은 1세에서 56세로 20, 30 대가 18예(64%)로 가장 많았다(Table 1).
수상형태는 압궤상이 12예(42.9%) 견열손상이 16 예(57.1%)이었다(Table 2).
Yamano1 혈관분류로는 Zone I이 17예(60.7%)
구
구심 심성 성 동 동정 정맥 맥 문 문합 합술 술을 을 이 이용 용한 한 수 수지 지첨 첨부 부의 의 재 재접 접합 합술 술
강남중앙병원 정형외과 황 순 호
Address reprint requests to: SSoooonn--HHoo HHwwaanngg,, MMDD Department of Orthopaedic Surgery,
Kang-Nam Jungang General Hospital
543-18 Sinlim 8 dong, Gwanakgu, Seoul, Korea TEL: 02-853-4600, FAX: 02-854-9844 E-mail: [email protected]
Zone II이 11예(39.3%)였다(Table 3). 19예에서 수 배부 정맥문합술이 불가능하여 구제술을 시행하였다.
나. 수술 방법
재접합 수술은 가능한 빠른 시간내에 하는 것을 원 칙으로 하여 내원 후 수술준비가 되는 대로 수술을 시 행하였으며 전 예에서 12시간 이내에 시행하였다. 모 든 예에서 압궤나 견열 손상이 심하여 원위 절단단의 동맥이 모두 소실되거나 파괴되어 동맥간의 문합이 불 가능한 경우 수장판의 연결가능한 정맥을 찾아 구심성 동-정맥 문합술을 시행하였다. 수배부 정맥 문합술은 가능한 모두 시행하였다(Fig. 1, 2, 3).
고 찰
1962년 Malt4에 의해 절단된 사지의 재접합이 성공 한 이후 1968년 Komatsu와 Tamai5가 수지 재접합
Fig. 1. (A) 10month old girl. 3rd and 4th finger distal phalanx amputation with crushing type. Artery of the amputee was so small that arteriorrhaphy was impossible. Arteriovenous anastomosis was done. (B) Immediate post-op. (C) Post-op. 2 month.
Table 1. Age and sex distribution
Age Number of Patient
Total (%)
Male Female
1-20 3 1 04 (14.2%)
21-30 5 2 07 (25.0%)
31-40 8 3 11 (39.2%)
41-50 4 1 05 (17.8%)
51-60 1 0 01 (03.5%)
Total 21 7 28 (100%)
Table 2. Type of injury
Type Number of the digits (%)
Crushing 12 (42.9%)
Avulsion 16 (57.1%)
Total 28 (100%)
Table 3. Yamano classification
Zone Number of the digits (%)
I 17 (60.7%)
II 11 (39.3%)
Total 28 (100%)
은 성공한 이래 수지 첨부에서는 1972년 Synder6가 처음으로 구제술을 성공하였다. 수지 첨부 재접합은 혈관의 크기가 아주 작고 분지되어 있으며 얇아서 손 상 받기가 쉬워 적당한 문합 혈관을 찾기 힘들다7. 또, 혈관 문합에 성공하더라도 술후 혈전과 혈관 연축이 빈번하여 그 성공률도 낮게 보고 되고 있다7. 또한, 최 근 증가하고 있는 압궤/견열 손상 또한 수지 첨부의
재접합술을 어렵게 하고 성공률도 떨어뜨리는 한 요인 이 되고 있다8. 수지 첨부 혈관 구조에 대해 Coleman 과 Ainson9에 의하여 발표되었고 Yamano1는 혈관 분류상 수지 첨부는 Zone I과 Zone II로 분류하였다.
Zone I은 조갑 기저부의 원위부, Zone II는 조갑기저 부에서 윈위지 관절까지를 말한다.
Cheng10 등은 Zone I에서는 동맥의 직경이
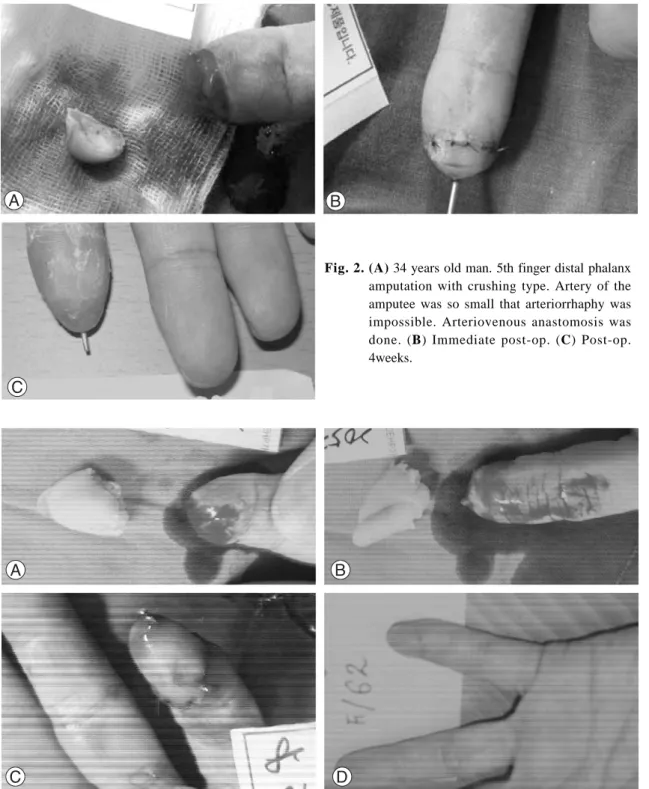
Fig. 2. (A) 34 years old man. 5th finger distal phalanx amputation with crushing type. Artery of the amputee was so small that arteriorrhaphy was impossible. Arteriovenous anastomosis was done. (B) Immediate post-op. (C) Post-op.
4weeks.
Fig. 3. (A) 62 years old woman. 5th finger distal phalanx amputation with avulsion type. Artery of the amputee was lost.Arteriovenous anastomosis was done. (B) Immediate post-op. (C) Post-op. 2month.
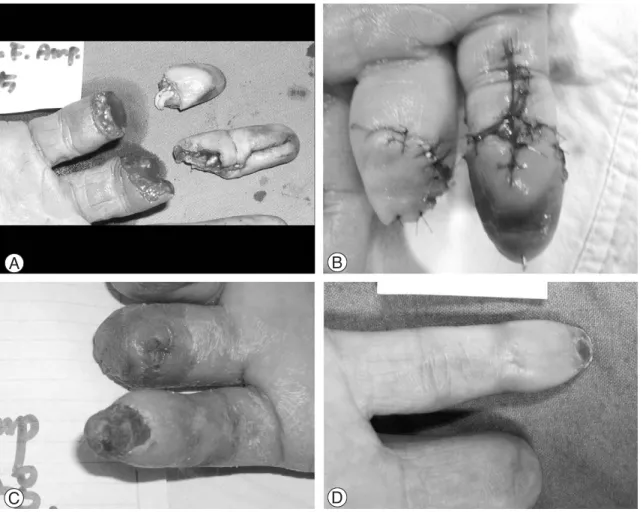
Fig. 4. (A) 38 years old man. 5th finger distal phalanx amputation with avulsion type. Artery of the amputee was lost.Arteriovenous anastomosis was done. (B) Immediate post-op. (C) Post-op. 3weeks. Partial necrosis of fin- ger tip was developed. (D) Post-op. 6weeks.
Fig.5. (A) 34 years old man. 5th finger distal phalanx amputation with avulsion type. Artery of the amputee was lost.Arteriovenous anastomosis was done. (B) Immediate post-op. (C) Post-op. 2month. Digit atrophy was developed.
0.3~0.5 mm이며 Pulp에서 여러갈래로 세분되어 직 경 0.1~0.2 mm 정도이며 Zone II에서는 혈관 직경 은 0.4~0.7 mm 정도이다. 정맥의 경우 조갑 양측의 수배부 정맥이 합쳐져 그 직경이 0.4~0.7 mm에 이 르며 수질부에서도 0.4~0.6 mm의 수장부 정맥을 발 견할 수 있다.
성공적인 유리동맥과 정맥 피판은 1981년 Nakayama3 에 의해 처음 보고되었다. 그 이후 수부 연부조직손상 에 이 방법을 많이 사용하고 있다. 구심성 동∙정맥 문합술을 이용한 수지 첨부의 재접합술이 Koshima11 등에 의해 발표되었다. 또한 원심성 동∙정맥 문합술 을 이용한 수지 첨부의 재접합술도 활발히 시행되고 있다12,13.
구심성 동∙정맥 문합시의 동맥화된 정맥층의 미세 혈류역학에 대해서는 아직 잘 알려지지는 않고 있지만 저용량의 동맥유입에 의해 피판이 생존하는 것으로 생 각되고 있다14.
수지첨부의 정맥에도 판막이 존재하나15 이것이 구심 성 동∙정맥 문합의 혈류 유합을 방해하지는 않는다16. 구심성 동∙정맥 문합술의 개념은 Nakayama3 등에 의해 처음 도입된 이후 고전적인 동맥 문합술이 불가 능 할 경우에 응급술식으로 수지 첨부의 재접합에 사 용되고 있고 상대적으로 큰 절단단의 생존에도 효과적 인 것으로 보고되고 있다16. 압궤상이나 견열 손상으로 동맥이 소실된 경우나 수지첨부의 동맥직경이 0.2 mm이하인 경우에도 정맥의 직경은 0.2 mm이상 이 므로, 정맥의 해부학적 구조가 비전형적이라 하더라도 제한된 경우에 있어서 동∙정맥문합이 가능하며, 대체 술식으로 수지첨부 재접합에 사용할 수 있다10,16. 저자 들의 경우 고식적인 동맥문합술 보다는 수지 위축이나 한랭부전들의 합병증이 많이 관찰되었다. 이는 초기의 심한 압궤상이나 견열 손상에 의한 것인지, 저용량의 동맥유입에 의한 조직 허혈에 의한 것인지 아직 밝혀 지지는 않았지만 성공률에 있어서는 고식적인 방법과 크게 차이를 보이지 않았다. 향후 수지위축이나 한랭 부전에 대한 원인 규명과 이에 대한 적절한 조치가 연 구된다면 원위 절단단의 동맥이 소실된 경우에 사용할 수 있는 매우 유용한 술식이라고 사료된다.
결 과
구심성 동∙정맥 문합술을 이용하여 재접합술을 시 행한 28예중 27예가 생존하여 96.4%의 생존율을 보 였다. 생존에 실패한 1예는 구제술을 시행한 경우였으 며, 술후 10일째 창상감염이 심하여 절단단 성형술을 시행하였다.
술후 합병증으로는 재접합부의 위축이 5예, 골수염
1예, 심한 통증을 호소한 경우가 1예, 한랭부전을 호 소한 경우가 2예 관찰되었다(Fig. 4, 5).
결 론
수지 첨부의 심한 압궤상이나 견열손상이 동반되어 윈위지 절단단의 동맥이 소실된 경우를 자주 겪을 수 있다. 이런 경우 성급한 절단단 성형술을 시행하기 보 다는 문합 가능한 정맥이 있는지 세밀하게 관찰을 하 여 동∙정맥 문합술을 시행하여 재접합술을 성공하면 환자에게 여러 가지 장점이 있으므로 적극적인 관심과 시도가 이루어져야 할 것으로 사료된다.
참고문헌
01) Yamono Y. Replantation of the amputated distal part of fingers. J Hand Surg. 1985;10:211-8.
02) Han SK, Lee BI, Kim WK. External bleeding method in zone I replantation. J Korean Soc Hand Surg. 1996;1:117- 25.
03) Nakayama Y, Soeda S, Kasai Y. Flaps nourished by arteri- al inflow through the venous system: an experineuteil investigation. Plast Reconstr Surg. 1981;67:328-34.
04) Malt RA, Mackhann CF. Replantation of servered arms.
JAMA. 1964;18:716.
05) Komatsu S, Tamai S. Successful replantation of a com- pletely cut off thumb: a case report. Plast Reconstr Surg.
1968;42:374-7.
06) Synder CC, Stevenson RM Browne EZ. Successful replan- tation of totally served thumb. Plast Reconstr Surg.
1972;50:553-9.
07) Kong BS, Kim YJ. Finger tip replantation. J K Microsurg.
2003;12:105-11.
08) Merle M, Dautel G. Advance in digital replantation. Plast Reconstr Surg. 1997;24: 87-105.
09) Colemann SS, Anson BJ. Arterial patterns in the hand based upon a study of 650 species. Surg Gynecol Obstet.
1961;113:409.
10) Cheug GL, Pan DD, Yang ZX, Qu ZY. Replantation of digit amputated at or about the distal interphalangeal joint.
Ann Plast Surg. 1985;15:465-73.
11) Koshima I, Soeda S, Moriguchi T, Higakai H, Miyakaua S, Yamasaki M. The use of arteriovenous anastomosis for replantation of thdistal phalanx of the fingers. Plast Reconstr Surg. 1992;89:710-4.
12) Smith AR, Sonneveld GJ, Van der Meulen JC. Av anasto- mosis as a solution for abscent venous drainage in replan-
tation surgery. Plast Reconstr Surg. 1983;71:525-30.
13) Suzuki Y, Ishikawa N, Isshiki N, Takami S. Finger tip replantation with an efferent A-V anastomosis for venous drainage. clinical reports. Br J Plast Surg. 1993;46:187-93.
14) Inada Y, Fukui S, Tamai S, Mizumoto S. The arterialized venous flap: experimental studies and a clinical case. Br J Plast Surg. 1993;46:61.
15) Moss SH, Schwartz KS, Von Drasek - Ascher G, Ogden L, Wheelar CS, Listor GD. Digital venous anatomy. J Hand Surg Am. 1985;10:473-82.
16) David R, Anthony C, Yvonne J, Stephen K. Afferent arte- riovenous anastomosis for thumb replantation: a case report. Microsurg. 1994;15:808-10.