Abstract
Maxillary sinus membrane perforation is not unusual during sinus lift procedures. The perforation of sinus membranes can cause maxillary sinusitis, graft failure and osseo-integration failures. Therefore, perforations of the maxillary sinus membranes should be carefully treated to obtain a successful result in implant restorations with sinus grafting. In cases of sinus perforation, the implant installation or sinus grafting has been delayed. However, if an adequate repair technique can be applied using a lateral window approach, then sinus grafting with or without dental implantations can be accomplished without any complications. Two cases in which sinus membrane perforations occurred during sinus lifting procedures are reviewed in this report. The perforated area in each case was at the margin of the detached lateral bony window, although the size was small, it was not ignored. Therefore, an additional bony window was formed at the margin at which the perforation occurred; thus, the perforation point became surrounded by a visible, intact sinus membrane, and the intact sinus membrane was lifted. The perforated area was covered with collagen membranes, accompanied by sinus bone grafting and implant installation. The repair of sinus membrane perforation was verified by radiographic examination, and a clinically good prognosis was observed during the follow-up period.
Key Words: dental implants, perforation, repair, schneiderian membranes, sinus floor augmentation
Application of a Simple Repair Technique for Small-Sized Perforations of Schneiderian Membranes: Case Report
In-Seong Jeon1, Min-Suk Heo2, Kwang-Heung Han1
1S & H Dental Clinic, Seoul, Korea
2Department of Oral and Maxillofacial Radiology, Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea
ISSN 1229-5418 Implantology 2013; 17(2): 80~86
Reprint requests: Kwang-Heung Han
S & H Dental Clinic, 485 Nohae-ro, Nowon-gu, Seoul 139-821, Korea Tel: 82-2-932-3618, Fax: 82-2-932-3619
E-mail: [email protected] Received for publication: April 26, 2013 Accepted for publication: June 14, 2013
Copyright © 2013. The Korean Academy of Oral & Maxillofacial Implantology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits
for small perforations of the Schneiderian membrane arising during sinus lifting surgery, with a review of two cases.
II Case Report
1. Case 1
A 51-year-old woman visited the dental clinic because of pain in the left maxillary second premolar.
The patient had no smoking habit and had no other specific medical history. She had undergone root canal therapy for the tooth; however, radiographic imaging showed an incomplete canal filling state and periapical radiolucency, indicating abscess formation. Endodontic treatment was again attempted for the tooth; however, an apical canal obstruction was found, and therefore immediate implantation with extraction of the tooth was planned.
The alveolar residual height from the alveolar crest to the sinus floor of the surgical area was 3~4 mm;
therefore, sinus grafting was planned using a through lateral window approach. In the radiographic exami- nation, the apex of the left maxillary second premolar was positioned over the sinus floor, but no oroantral communication was found because of the presence of a thick bundle of bone around the dental root.
Extraction of the tooth under local anesthesia was
Lateral and crestal approaches are widely rec- ommended for maxillary sinus floor augmenta- tion. Furthermore, the lateral window approach has been recommended to obtain more predictable results in cases of small residual alveolar ridges because it can provide a greater amount of membrane lifting with no tearing1,2.
Several factors, such as an acute bony angle between the two planes of the maxillary sinus floor, membrane thickness, a sinus septum, and the dental root config- uration, contribute to Schneiderian membrane tear- ing3. Membrane perforation can also occur during the lateral window approach; however, Boyne suggested that the perforation itself did not matter when it could be repaired appropriately4.
In many cases in which sinus membrane perforation has occurred, the perforation could be repaired by being covered with collagen membrane. However, to secure the positional stability of the collagen mem- brane that covers the perforation area, the membrane should be supported by an intact sinus membrane;
therefore, exposure of the intact sinus membrane around the perforation area should precede the repair procedure.
Two cases are introduced here, in which successful sinus grafting and implant restoration were achieved through additional bony window preparation and col- lagen membrane application for the repair of accidental perforation of the sinus membrane.
Case Reports
undertaken, and a vertical incision was made with a
#15 blade at the distal side of the upper left first pre- molar and the mesial side of upper left first molar, and the mucoperiosteal flap was elevated. With this step, the apico-coronal length of the buccal flap was suffi- cient to make visible the lateral bony wall of the max- illary sinus.
The lateral bony window was prepared with a low- speed diamond point and was detached. During the sinus membrane lifting procedure, a membrane perfo- ration occurred at the anterior margin of the exposed sinus membrane. To expose the intact sinus membrane around the perforation point, the bony window was extended anteriorly by 2 mm; thus, a small-sized accessory bony window, which included the perforation area, was created. The exposed, intact sinus mem-
brane was lifted cautiously so as not to touch the torn area, and lifting of the palatal side of the sinus mem- brane was verified.
After drilling for implant fixture installation was accomplished, the perforation area was covered with moisturized collagen membrane (CollaTape, Zimmer Dental, Carlsbad, CA, USA). At this step, every margin of the CollaTape contacted the intact sinus membrane.
Alloplastic bone substitute material (Cerasorb, Curasan, Kleinostheim, Germany) was packed into the cavity under the lifted Schneiderian membrane, while CollaTape was attached beneath the sinus membrane, which was lifted and held with a long tissue forceps.
After grafting, an implant fixture of 4.1 mm in diame- ter and 11.5 mm in length (SS type, Osstem Implant, Seoul, Korea) was installed. The original bony window
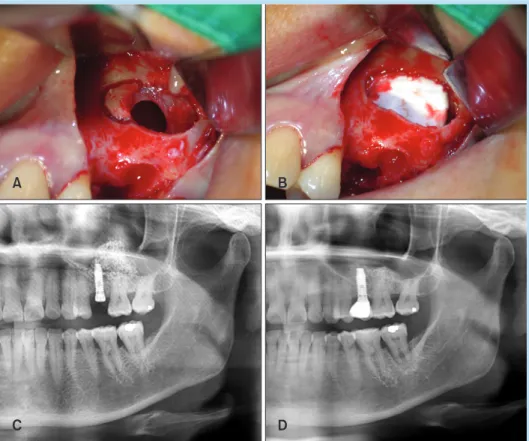
Fig. 1. (A) An accessory window was prepared next to the membrane tear site. (B) The sinus membrane was lifted, and the perforation area was covered with collagen membrane. (C) Post-operative panoramic view: dome-shaped sinus grafting can be seen, with mild graft material scattering. (D) 20-months after surgery: the stabilized graft area can be seen.
In-Seong Jeon et al. : Application of a Simple Repair Technique for Small-Sized Perforations of Schneiderian Membranes: Case Report. Implantology 2013
were removed 10 days postoperatively, and no sign of infection was observed. Prosthetic restoration was accomplished at 5 months postoperatively, and bone formation around the fixture was observed on radio- graphic examination at 1 year after the prosthetic res- toration (Fig. 1).
2. Case 2
A 63-year-old man visited the clinic for rehabilita- tion of an edentulous maxillary left posterior area. He was a non-smoker and had no specific medical histo- ry. The upper left dentition from the first premolar to the second molar was lost due to periodontitis, and
therefore, immediate implantation of two dental implant fixtures with sinus grafting was planned.
A horizontal incision was made from the left maxil- lary tuberosity to the distal surface of left canine, with a vertical incision made at each end of the horizontal incision. A full-thickness mucoperiosteal flap was ele- vated to expose the lateral side of the left maxillary sinus, and a bony window was prepared. The bony window was detached from the sinus membrane, and sinus lifting was attempted. During sinus lifting, the sinus membrane was torn at the anterior margin of the bony window. An accessory window, extended from the originally prepared window area, was created and
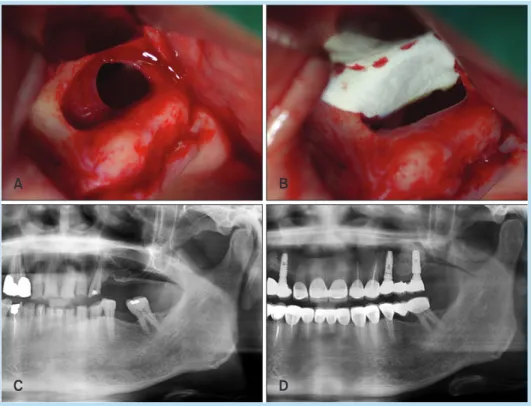
Fig. 2. (A) An intact sinus membrane along the extended bony window can be seen. (B) Collagen membrane was inserted beneath the lifted sinus membrane. (C) Pre-operative panoramic view: the edentulous ridge area of the upper left posterior region with compromised vertical dimension of alveolar bone. (D) 5-months after surgery: the stabilized sinus grafting area can be seen.
In-Seong Jeon et al. : Application of a Simple Repair Technique for Small-Sized Perforations of Schneiderian Membranes: Case Report. Implantology 2013
Case Reports
detached; therefore, an intact membrane was visible all around the margin of the bony window.
The sinus membrane was lifted with cautious han- dling, so as not to enlarge the size of the perforation area, by handling only the intact membrane. Drilling for implant fixture installation was undertaken at the upper left first premolar and the first molar region.
The perforation area was covered with moisturized col- lagen membrane (CollaTape), and sinus grafting was accomplished with alloplastic bone substitute material (Cerasorb), while the collagen membrane was lifted and held with a long tissue forceps. Dental implant fixtures (SS fixture of 4.1 mm in diameter and 11.5 mm in length; GS fixture of 5.0 mm in diameter and 11.5 mm in length; Osstem Implant) were installed, and the detached bony window was repositioned; a suture was made with 4-0 nylon. A second surgery and prosthetic restoration were accomplished at 5 months postopera- tively. On radiographic examination, newly formed radiopaque hard tissue around the implant fixtures was observed (Fig. 2).
III Discussion
Maxillary sinus perforation occurring during sinus lifting procedures has been reported to be a common complication of sinus lifting, and the incidence has ranged from 11% to 56% in previous stuidies6-8. There are many risk factors for perforations, such as sinus floor irregularities, septa, thin membranes, previous sinus operations, adhesion of the Schneiderian mem-
brane, and an absence of bone between the sinus mucosa and oral mucosa3,9-12. In this report, a sinus floor irregularity at the upper premolar apex in case 1 and a thin Schneiderian membrane in case 2 were the main causative factors of membrane perforation.
There have been many studies and reports of repair techniques; however, most of these studies have rec- ommended delaying the installation of dental implant fixtures. Khoury13 recommended that simultaneous implant placement should be avoided when severe per- forations occur because new bone formation around the fixtures within the sinus cavity would be unpre- dictable. On the other hand, some reports have pro- posed that bone grafts would not be affected if ade- quate repair were conducted5,14. The authors of the current study also performed simultaneous (immedi- ate) implantation, although there was a perforation of the sinus membrane.
Inadequate handling of small-size perforations of the Schneiderian membrane can enlarge the perfora- tions; therefore, they should be repaired carefully. In case 1 and 2 in this report, the extension technique was suggested to repair a small-sized perforation as follows. When the perforation was small and at the margin of the lateral window, an accessory bony win- dow was created next to the perforation site. The size of the accessory window was large enough to allow for the gap distance to handle the instrument, avoiding the perforation point of the Schneiderian membrane.
After extension of the window, the accessory window was detached from the membrane, and the perforation site was surrounded by an intact membrane.
Meticulous sinus lifting was performed so as not to
lifted perforation area, and bone grafting was per- formed. CollaTape has the physical property of expanding when moistened with water; therefore, it is very helpful to completely seal the perforation area.
Furthermore, the entire margin of the CollaTape was retained and supported by an intact sinus membrane.
The original bony window and the accessory window were repositioned, and finally implant fixture was installed.
The presence of several millimeters of intact sinus membrane around the tear region might be a key for successful repair for small-sized perforations. The extension of the bony window at the margin of the perforation is useful in such situations. If the thick- ness of the sinus membrane is adequate, there should be no more tearing. A sufficient amount of membrane lifting can cause membrane folding; therefore, the size of the perforation is minimized. Short-acting, resorb- able collagen membrane, such as CollaTape, is suitable for the successful repair of injured membranes. In cases of simultaneous implantation, implant drilling should be performed before the sinus membrane per- foration is sealed with collagen membrane. Long tissue forceps are useful for temporarily holding the CollaTape during bone grafting. After grafting and window repositioning, implant fixture installation is performed.
In conclusion, extension of the bony window and the use of moisturized collagen membrane, such as CollaTape, can be very useful for accidental perfora- tions of the Schneiderian membrane during sinus lift- ing procedures.
References
1. Wallace SS, Froum SJ. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann Periodontol. 2003; 8: 328-343.
2. Del Fabbro M, Testori T, Francetti L, et al. Systematic review of survival rates for implants placed in the grafted maxillary sinus. Int J Periodontics Restorative Dent. 2004; 24: 565-577.
3. Ardekian L, Oved-Peleg E, Mactei EE, et al. The clinical significance of sinus membrane perforation during augmentation of the maxillary sinus.
J Oral Maxillofac Surg. 2006; 64: 277-282.
4. Boyne PJ. Analysis of performance of root-form endosseous implants placed in the maxillary sinus. J Long Term Eff Med Implants. 1993; 3:
143-159.
5. Pikos MA. Maxillary sinus membrane repair: report of a technique for large perforations. Implant Dent. 1999; 8: 29-34.
6. Schwartz-Arad D, Herzberg R, Dolev E. The prevalence of surgical complications of the sinus graft procedure and their impact on implant survival. J Periodontol. 2004; 75: 511-516.
7. Barone A, Santini S, Sbordone L, et al. A clinical study of the outcomes and complications associated with maxillary sinus augmentation. Int J Oral Maxillofac Implants. 2006; 21: 81-85.
8. Kasabah S, Krug J, Simůnek A, et al. Can we predict maxillary sinus mucosa perforation? Acta Medica (Hradec Kralove). 2003; 46: 19-23.
9. Becker ST, Terheyden H, Steinriede A, et al. Prospective observation of 41 perforations of the Schneiderian membrane during sinus floor
Case Reports
elevation. Clin Oral Implants Res. 2008; 19: 1285-1289.
10. van den Bergh JP, ten Bruggenkate CM, Disch FJ, et al. Anatomical aspects of sinus floor elevations. Clin Oral Implants Res. 2000; 11: 256- 265.
11. Berengo M, Sivolella S, Majzoub Z, et al. Endoscopic evaluation of the bone-added osteotome sinus floor elevation procedure. Int J Oral Maxillofac Surg. 2004; 33: 189-194.
12. Watzak G, Tepper G, Zechner W, et al. Bony press-fit closure of oro-
antral fistulas: a technique for pre-sinus lift repair and secondary closure.
J Oral Maxillofac Surg. 2005; 63: 1288-1294.
13. Khoury F. Augmentation of the sinus floor with mandibular bone block and simultaneous implantation: a 6-year clinical investigation. Int J Oral Maxillofac Implants. 1999; 14: 557-564.
14. Karabuda C, Arisan V, Özyuvaci H. Effects of sinus membrane perforations on the success of dental implants placed in the augmented sinus. J Periodontol. 2006; 77: 1991-1997.