Original Article
원고 접수일 2010년 11월 9일, 게재 확정일 2011년 2월 24일 책임저자 김수관
(501-759) 광주시 동구 서석동 375번지, 조선대학교 치과대학원 구강악안면외과학 교실
Tel: 062-220-3819, Fax: 062-228-7316, E-mail: [email protected]
RECEIVED November 9, 2010, ACCEPTED February 24, 2011 Correspondence to Su-Gwan Kim
Department of Oral & Maxillofacial Surgery, School of Dentistry, Chosun University
375, Seosuk-dong, Dong-gu, Gwangju 501-759, Korea
Tel: 82-62-220-3819, Fax: 82-62-228-7316, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
자가치아를 이용한 골이식재의 임상적 유용성: 일차 보고
이정훈ㆍ김수관ㆍ문성용ㆍ오지수ㆍ김영균1
조선대학교 치의학전문대학원 구강악안면외과학교실, 1분당서울대학교병원 치과 구강악안면외과
Abstract
Clinical Effectiveness of Bone Grafting Material Using Autogenous Tooth: Preliminary Report
Jeong-Hoon Lee, Su-Gwan Kim, Sung-Young Moon, Ji-Su Oh, Young-Kyun Kim
1Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University,
1
Department of Oral and Maxillofacial Surgery, Section of Dentistry, Seoul National University Bundang Hospital
Purpose: The purpose of this study was to evaluate the effectiveness of a novel bone grafting material using an autogeneous tooth (AutoBT) and provide the basis for its clinical application. The AutoBT contains organic and inorganic mineral components and is prepared from autogenous grafting material, thus eliminating the risk of immune reactions that may lead to its rejection.
AutoBT can be used as bone material as is has both osteoinduction and osteoconduction activities at guided bone regeneration for implant placement and maxillary sinus graft.
Methods: In a total of 63 patients, guided bone regeneration surgery was performed at the time of implant placement, and tissue samples were harvested at the time of the second surgery with the patient's consent.
Results: There were no complications in guided bone regeneration using autogeneous tooth.
Conclusion: We concluded that AutoBT underwent gradual resorption and was replaced by new bone of excellent quality via osteoinduction and osteoconduction.
Key words: Autogenous tooth, Implant, Guided bone regeneration, Tooth bone
서 론
임프란트 식립을 위한 무치악부 혹은 골결손 부위의 수복을 위해 많은 종류의 골이식재료가 개발되어 임상에서 사용되고
있다[1-10].
이 중 경조직 결손부 재건에 있어서 자가골 이식은 골형성,
골유도 및 골전도 능력을 모두 보유하고 있을 뿐 아니라 면역
거부반응이 없고 빠른 치유를 보이는 장점을 가지고 있기 때문에
Table 1. Implant distribution and survival data
AutoBT Mixed bone graft materials No. of patients Sinus augmentation
GBR Extraction site
Anatomical deficiency site
14 24 3
14 6 2
28 30 5 GBR, guided bone regeneration.
Fig. 1. Pre-operative CT image and 6 months after CT image.
Fig. 2. Maxillary sinus augmentation with AutoBT and immediate
implantation.Fig. 3. Implant placed in a extraction socket.
gold standard로 여겨지고 있다. 따라서, 골이식 시 가장 먼저 고려될 수 있으나 자가골 이식은 채취량이 제한적이고 이식 후 예측 불가능한 흡수와 공여부에 이차결손을 유발하는 단점을 가지 고 있다[8,11]. 이와 같은 단점을 극복하고자 동종골, 이종골 및 합성골의 골대체 물질이 개발되어 임상에서 사용되고 있으나 동종 골과 이종골, 합성골은 감염의 확산문제와 임상적인 적용에 있어 높은 비용 등의 문제가 있다. 이러한 자가골과 골대체 물질이 가진 한계를 극복할 이상적 골이식재료에 대한 연구가 활발히 진행되고 있으며 최근 이러한 이상적인 골이식재료의 대안으로 자가치아이식재가 개발되었다. 자가치아이식재는 우수한 골전도, 골유도능을 가지며 자가골 이식과 조직학적 치유과정이 유사하다
고 보고되었다[1,12].
자가치아이식재는 기존의 골대체물질들이 가지고 있었던 감염 의 가능성, 높은 비용, 골형성 능력의 한계 등의 문제점을 해결함으 로써 자가골을 대체할 수 있는 이상적인 골이식재료로 평가받고 있다. 그러나, 자가치아이식재를 이용한 임상연구가 아직 미흡하여 본 연구에서는 자가치아골이식재를 이용하여 임프란트 식립을 위한 골이식을 시행하여 임상적, 방사선학적 평가를 통해 임프란트 식립 을 위한 골대체 물질로서의 임상적 효용성을 평가하고자 하였다.
연구방법
2008년부터 2010년까지 조선대학교 치과병원 구강악안면외 과 및 치주과에 임프란트 식립을 위해 내원한 환자를 대상으로 하였다. 환자는 총 63명으로 이 중 남자는 48명, 여자는 15명이었 으며, 연령은 18세부터 73세였다. 상악동거상술에 사용된 경우는 28증례였고, 임플란트 식립을 위한 골이식이 시행된 증례는 35예 였다 (Table 1). 그 외에 조절되지 않는 당뇨나 골다공증과 같은 예후에 영향을 미칠 수 있는 전신질환을 가진 환자는 본 연구에서 제외하였으며, 낭이나 종양과 같은 병리학적 원인으로 발생한 골결손부 또한 제외하였다. 시술 전 자가치아골이식 및 모든 시술 과정에 대한 충분한 설명과 동의를 구한 후 진행되었다.
술 전 CT 촬영을 시행하여 잔존골의 높이를 확인하고 통상적인
방법으로 상악동 거상술을 시행하였으며, 상악동 거상술 시 골이
식재로로 자가 치아골이식재를 이용하였다(Fig. 1, 2). 잔존골
Fig. 4. Guided bone regeneration using Auto BT.
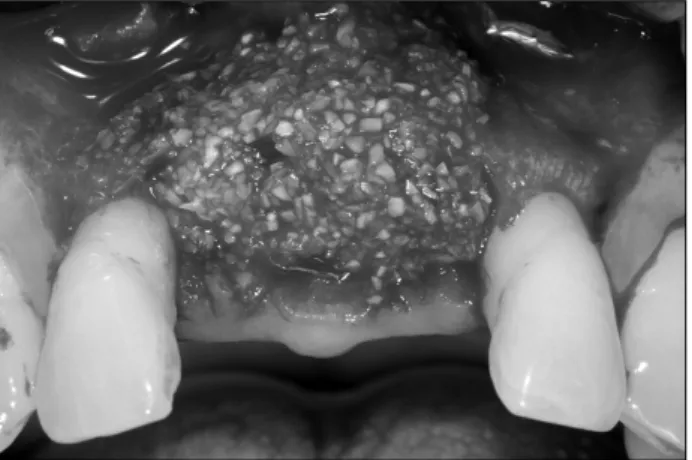
Fig. 5. Bone regeneration was observed after 6 months. Fig. 7. Guided bone regeneration with AutoBT.
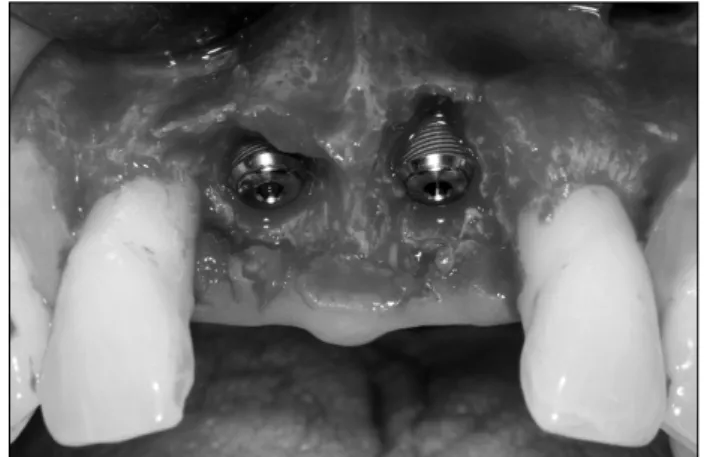
Fig. 6. Implant fixture exposure.
Fig. 8. 8 months later bony remodeling appearance.
높이가 5 mm 이하일 때 lateral window opening technique을 사용하였으며, 그 이상일 때는 Socket lift technique을 사용하였 다[13-15].
골유도 재생술에서는 발치 후 치아의 골이식재로의 재처리 과정에 소요되는 약 7∼10일 경과한 이후 다시 발치 부위를 개방 시켜 육아조직을 제거하고 임프란트를 식립과 동시에 골이식을 시행하거나(Figs. 3∼5), 임프란트 식립 시 노출된 나사선의 골이 식시에 자가치아 이식재를 사용하였다(Figs. 6∼8).
모든 증례에서 임상적, 방사선적 경과관찰을 위하여 술 전, 술 후, 3개월, 6개월 간격으로 내원시켰으며 내원시 골과 임프란 트 사이의 골유착관계를 파악하기 위해 임상적, 방사선적 검사를 시행하였다. 임상적으로 통증이나 감염의 유무, 신경학적 변화, 그리고 임프란트 동요도를 관찰하였고 방사선적 평가를 위해 표준
구내방사선사진과 파노라마, CT를 촬영하였다.
결 과1. Maxillary sinus augmentation
술 중 두 명의 환자에서 상악동막의 천공이 발생하였으며, 흡수
성 차단막을 이용한 후 상악동 거상술을 시행하였고, 술 후 합병증
Table 2. Mean+/−SD and paired t test of resorption of bone height by bone materials during different observation periods
Resorption of vertical bone height (mm)Only AutoBT AutoBT+Bone materials
P value
After 3 months After 6 months
1.29+/−0.474 1.50+/−0.289
0.57+/−0.297 0.6+/−0.245
0.226 0.048
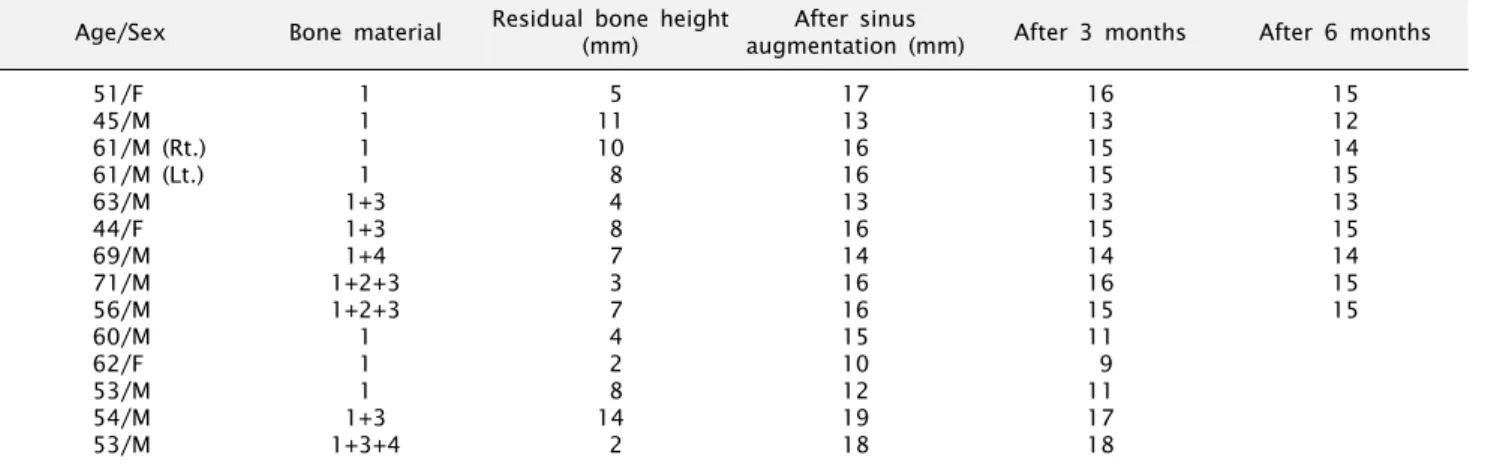
Table 3. Bone height change after maxillary sinus augmentation
Age/Sex Bone material Residual bone height(mm) After sinus
augmentation (mm) After 3 months After 6 months 51/F
45/M 61/M (Rt.) 61/M (Lt.) 63/M 44/F 69/M 71/M 56/M 60/M 62/F 53/M 54/M 53/M
1 1 1 1 1+3 1+3 1+4 1+2+3 1+2+3
1 1 1 1+3 1+3+4
5 11 10 8 4 8 7 3 7 4 2 8 14 2
17 13 16 16 13 16 14 16 16 15 10 12 19 18
16 13 15 15 13 15 14 16 15 11 9 11 17 18
15 12 14 15 13 15 14 15 15
1, AutoBT; 2, OSTEON; 3, Tutoplast; 4, Bio-oss.
은 발생하지 않았으며, 6개월 후에도 방사선 검사 및 임상적 검사 에서 어떤 합병증이나 실패의 증거가 관찰되지 않았다(Fig. 1).
28명의 상악동거상술 환자중 환자에게 자료 제공동의를 구한 14명의 환자에서 술 후, 술 후 3개월, 술 후 6개월에 CT를 촬영하 여 잔존골의 높이를 분석하였다. 표본의 수가 한정적이어서 거상 량의 분포를 제한하지 못하였지만 현재까지 수집된 자료를 토대로 분석해 보았다. 그 결과 술 후 3개월에서 골의 평균 흡수량은 0.9 mm, 술 후 6개월째 9개의 표본에서 평균흡수량은 1.0 mm를 보여 유의할 만한 차이를 나타내지 않았다. 표본을 다시 자가치아 골이식재만 사용한 경우와 다른 골이식재를 혼합하여 사용한 경우 를 통계학적으로 분석하였을 때 술 후 3개월에 서로 유의한 차이 가 없는 것으로 나타났다(Table 2). 반면 술 후 6개월에서는 서로 통계적 유의성을 나타내어 이식재의 혼합 사용 시 술 후 골흡수량이 감소함을 관찰할 수 있었다( P <0.05)(Table 3).
2. Guided bone regeneration
발치와에 자가치아골이식과 함께 임프란트를 즉시 식립한 30 명의 환자 중 2명에서 술 후 열개가 관찰되었고, 구내소독 및 약물요법과 같은 보존적 처치만 시행하였고 약 3주 후 다른 합병 증 없이 연조직이 이차 유합되었다. 5명의 환자에서 임프란트 식립시 협측 나사선 노출부에 골이식을 시행하였으며, 감염이나 천공, 열개와 같은 부작용 없이 성공적으로 치유되었다. 골이식을 시행한 35명의 환자에서 2차수술 시 나사선의 노출 없이 이식재가
잘 유지되고 있었다(Fig. 5).
고 찰
임프란트 식립 시 잔존골이 부족하거나 상악동의 함기화로 잔존골의 높이가 적절하지 못한 경우 골이식술을 동반하게 된다.
자가골이 가장 이상적이나 여러 단점을 보완하기 위한 골대체 물질들이 개발되었으며, 그 중 하나가 자가치아를 이용한 골이식 재이다.
해부학적 구조의 한계는 임프란트 식립 시 가장 흔히 겪게 되는 문제점 중 하나이고 이를 극복하기 위해 골이식이나 치조제 증강술 등이 사용된다[16,17]. 특히, 상악 전치부에서 좁고 오목한 치조제의 형태로 인해 임프란트 식립시 협측골판의 천공이 관찰되 기도 하며, 또한 얇은 피질골로 이루어져 있어 발치 후 수주 안에 현저한 골흡수가 일어나기 때문에 임프란트 초기고정 및 유지에 어려움이 많은 부위이다[18,19]. 발치와에 즉시 임프란트를 식립 하는 것은 여러 가지 장점이 보고되었다[20]. 가장 큰 장점은 발치 후 즉시 식립을 통해 골조직의 수직적, 수평적 고경을 유지 시켜 발치 이전의 치아위치에 임프란트를 식립할 수 있다는 점이 다[21].
Kim 등[3]은 2009년 연구에서 자가치아 골이식재의 inorganic
component, 표면구조, 치유과정에 대한 조직학적 분석을 통해
자가치아 이식재가 osteoconduction뿐만 아니라 osteoin-
duction의 능력을 지니고 있어 자가골과 비슷한 골형성능을 가진 다고 보고하였다.
이에 본 연구에서는 자가치아를 이용한 골이식의 임상적 효용 성에 대해 알아보고자 하였으며, 자가치아골이식재와 그 외 이종 골, 합성골을 혼합하여 복합이식을 하여 자가치아골이식재의 유 용성을 평가하여 보았다. 자가치아골이식재는 이식재로서 자가치 아 이식재는 술 후 낮은 합병증을 보였고, 임상적으로 양호한 골형성 양상이 관찰되었다.
자가치아를 이용한 골이식술의 임상적 유용성이 확인되었으나 골이식 후 경과 관찰기간이 짧고, 다른 골이식재와의 직접적인 비교 연구가 되지 않은 한계가 있어 향후 장기간의 관찰과 연구를 통한 고찰이 필요하리라 생각된다.
결 론
자가치아뼈이식재의 임상적 유용성에 대해 알아보고자 임프란 트 식립시 골이식이 필요한 환자 63명에게 골이식과 상악동거상 술을 시행하였다.
1. 상악동거상술이 시행된 28명의 환자 중 2명에서 상악동막의 천공이 관찰되었으나 보존적 처치를 통해 다른 합병증 없이 모두 잘 치유됨을 알 수 있었다.
2. 발치와 및 임프란트 나사선 노출 부위에 시행한 골이식 환자 35명 중 2명에서 술 후 열 개가 관찰되었으나 보존적 처치를 통해 정상적인 치유를 보였다.
3. 현재까지의 임상적, 방사선적 검사 시 합병증 없이 모두 잘 치유되고 있었다.
Acknowledgements
이 논문은 2008학년도 조선대학교 학술연구비의 지원을 받아 연구되었음.
References