Long-term Follow-up Sonography of Benign Cystic Thyroid Nodules after a Percutaneous Ethanol Injection:
The Incidence of Malignancy-mimicking Nodules
1Ji Sung Park, M.D., Dong Wook Kim, M.D., Choong Ki Eun, M.D., Seok Jin Choi, M.D., Myung Ho Rho, M.D.2
1Department of Radiology, Busan Paik Hospital, Inje University School of Medicine, Busan, South Korea.
2Department of Radiology, Masan Samsung Hospital, Sungkyunkwan University School of Medicine, South Korea.
This work was supported by the Inje Research and Scholarship Foundation in 2003.
Received August 18, 2007 ; Accepted November 7, 2007
Address reprint requests to : Dong Wook Kim, M.D., Department of Radiology, Busan Paik Hospital, Inje University School of Medicine, Busan, South Korea, 633-165, Gaegeum-dong, Busanjin-gu, Busan, South Korea
Tel. 82-51-890-6543 Fax. 82-51-896-1085 E-mail: [email protected]
Purpose: To evaluate the incidence of malignancy-mimicking sclerosed thyroid nod- ules, from long-term follow-up ultrasonography (US) after an US-guided percutaneous ethanol injection (PEI).
Materials and Methods: We examined 86 benign cystic thyroid nodules from 80 pa- tients. The nodules were classified into two groups based on whether an aspiration (Group A, n=26) or non-aspiration (Group B, n=60) of infused ethanol was per- formed. The final follow-up US over 12 months was performed in all patients.
Results: Of the 86 nodules, the cystic portion of 82 (95.3%) cases, from 76 patients, completely disappeared subsequent to the first follow-up US (Group A, n=24, Group B, n=58) (Chi-square test, p>0.05). Moreover, 46 sclerosed thyroid nodules showed two or more of the ‘five sonographic criteria’ upon a follow-up US (Group A, n=13, 50.0%, Group B, n=32, 53.3%). A higher ratio of the cystic portion of the nodules was associated with a higher incidence of the ‘five sonographic criteria’ for malignancies detected via a follow-up US (p<0.01; Student’s t-test).
Conclusion: For the long-term follow-up US, the ‘five sonographic criteria’ were ob- served in half the patients who received US-guided PEI. Also, by acknowledging the possibility that sonographic findings mimic a malignancy, since the sclerosed thyroid nodule, patients may avoid an unnecessary biopsy.
Index words :Thyroid nodule Ethanol sclerotherapy Ultrasonography Sclerotherapy
Ultrasonography (US)-guided percutaneous ethanol injection (PEI) is a popular treatment method for cystic or solid benign thyroid nodules because it is simple, in- expensive, highly successful, and safe. In fact, several reports exist describing the efficacy and safety of US- guided PEI for the treatment of benign cystic thyroid nodules (1-8). In spite of this, several unnecessary US- guided fine-needle aspiration biopsy (FNAB) have been performed for the treatment of sclerosed thyroid nod- ules which mimick malignancy on follow-up US.
Hence, the goal of this study is to determine the inci- dence of malignancy-mimicking sonographic findings in sclerosed thyroid nodules after US-guided PEI and eval- uate the difference in the incidence of malignancy-mim- icking sonographic findings in the sclerosed nodules based on the cystic percent make-up of the thyroid nod- ules. To the best of our knowledge, no previous studies have examined the possibility of malignancy-mimicking in benign cystic thyroid nodules by long-term follow-up US after an US-guided PEI has not been reported. In ad- dition, we compared the incidence of malignancy-mim- icking sonographic findings in the nodules that were or were not subjected to the aspiration of infused ethanol during US-guided PEI.
Subjects and Methods
Eighty-six biopsy-proven benign cystic thyroid nod- ules were examined in 80 patients (13 males, 67 fe- males, age range 12-75 years, mean 42.9 years), who have received US-guided PEI. As for the complex cystic thyroid nodules, we performed an US-guided FNAB for the cystic and solid components of the nodule.
Moreover, for the purely cystic thyroid nodules, we as- pirated all of the fluid, and immediately smeared it, and sent the remaining fluid into the pathologic department for the preparation of cell blocks. We obtained informed consent from all patients for all the US-guided FNA and PEI.
The US-guided PEI was performed with a 128 XP/10 scanner (Acouson, Mountain View, CA U.S.A.) using a 7-MHz linear probe. Furthermore, the follow-up US was executed with an HDI 3000 scanner (Advanced Technology Laboratories, Bothwell, WA U.S.A.) or a 128 XP/10 scanner.
US-PEI
The cystic percentage of the thyroid nodules was de- termined using the following formula:
Equation 1: (Volume of the cystic portion: length × width × height × π/6) /
(Volume of the entire cystic thyroid nodule: length
× width × height × π/6) × 100
Under ultrasonographic guidance, an 18- to 23- gauge needle, which was selected according to the fluid viscos- ity of the cystic nodule, was inserted into the lumen of the cystic thyroid nodule to aspirate as much cystic fluid as possible. A local anesthetic was not routinely applied unless requested by the patient. Moreover, an appropri- ate amount of 99.9% ethanol was slowly instilled into the nodule cavity to a volume of 20-100% of the aspi- rated fluid without removing the needle. The thyroid nodules were classified into two patients groups based on whether aspiration (Group A, n=26) or non-aspira- tion (Group B, n=60) of infused ethanol was performed.
For the Group A nodules (n=26), the instilled ethanol was nearly completely evacuated from the nodule using a second needle after 10 min. For the Group B nodules (n=60), an US-guided PEI was completed within 10 min, (i.e. the instilled ethanol was not evacuated). An US-guided PEI was not performed in the solid portions of the thyroid nodules in this study.
Follow-up US
Multiple follow-up sonographic examinations were performed after US-guided PEI. We arbitrarily defined a successful US-guided PEI, for a benign cystic thyroid nodule, as the complete loss of the cystic portion of a thyroid nodule following the first follow-up sonogram.
All cases with a complete disappearance of the cystic portion of the thyroid nodule after US-guided PEI re- vealed a purely solid nodule following the first follow- up US, a gradual decrease in size for a subsequent fol- low-up US and disappearance without recurrence for a long-term follow-up US.
The recently accepted sonographic findings for malig- nant thyroid nodules demonstrate positive predictive value, despite low sensitivity, and make up the ‘five sonographic criteria’, which include hypoechogenecity, an irregular margin, microcalcification, intranodule vas- cularity and a more tall than wide formation (9-13). We arbitrarily adopted these songraphic findings as ‘sono- graphic criteria’ and examined their incidence in post- instilled thyroid nodules for follow-up US.
Over the course of more than 12 months of follow-up USs, the success rate and incidence of the ‘five sono- graphic criteria’ in the study patients was investigated.
The incidence of ‘five sonographic criteria’ was correlat- ed with the cystic percentage of the initial thyroid nod- ules. Also, the incidence of the ‘five sonographic crite- ria’ was compared for Groups A and B thyroid nodules.
Results
Of the 86 thyroid nodules, 68 were complex cysts and 18 were pure cysts. In a single nodule, the cystic portion was greater than half of the volume of the nodule in all cases. A simultaneous sclerotic therapy was performed in four cases (two nodules in three cases and four nod- ules in one case) for multiple benign cystic thyroid nod- ules. Table 1 and 2 lists the clinical data, the results of the sclerotherapy, and the incidence of the ‘five sono- graphic criteria’ in all of the treated patients.
US-PEIT
For the thyroid nodules belonging to Group A, the ini- tial cystic volumes ranged from 2 to 20 mL (mean, 5.5 mL) before sclerotherapy. Moreover, the infused
ethanol volumes ranged from 2.0 to 12.0 mL (mean, 4.7 mL). Further, the cystic percentage ranged from 50 to 100% (mean, 82.5%). For Group B nodules, the initial cystic volumes, before sclerotherapy, ranged from 1.0 to 96.0 mL (mean, 9.8 mL), whereas the infused ethanol volumes ranged from 1.0 to 20.0 mL (mean, 6.4 mL).
The cystic portion of the thyroid nodules ranged from 50.0 to 100.0% (mean, 86.9%).
US-guided PEIs were well tolerated in all patients, with no significant complications related with the proce- dure.
Follow-up US
The first follow-up US was performed between 1 and 12 months after a US-guided PEI (mean, 6.6 months for Group A and 4.4 months for Group B), whereas the last follow-up was performed between 12 and 45 months af- ter US-guided PEI (mean, 25.1 months for Group A and 19.6 months for Group B). We obtained an excellent success rate for the US-guided PEI in both groups (95.3%; 92.3% in Group A and 96.7% in Group B) as
Table 1. Clinical Data, Results of US-guided PEI and Incidence of ‘Five sonographic criteria’ in Group A
Sex Age Cystic First Infused First follow-up Last follow-up ‘Five sonographic
(yrs) portion (%) aspirate (ml) ethanol (ml) (month) (month) criteria’ Complications
F 46 100 02 02 18 45 a,b,c mild pain
F 32 090 04 04 20 45 a,b
F 31 050 02 02 02 30 mild pain
F 35 100 07 07 39 45 a,b,c,d
F 60 100 02 02 01 44 mild pain
F 32 100 02 02 38 45 c,d
F 24 080 08 05 01 12
F 74 090 02 02 08 20 a,b mild pain
F 41 075 04 04 02 45
F 31 085 08 06 01 37 a,b,c
F 42 055 05 05 03 22
F 29 050 04 04 14 38
F 60 095 08 09 03 23
F 43 095 02 02 04 24 a,b,c,e
F 62 050 20 12 01 12
M 55 095 04 04 01 15 a,b,c,e
F 46 050 04 04 01 15 mild dizziness
F 20 090 02 02 01 12 a,b,c mild pain & facial palsy
F 49 085 04 04 01 14 a,b
M 43 085 05 05 01 14 a,b mild pain
F 47 090 17 10 01 13
F 68 090 04 04 03 16 b mild pain
F 45 085 08 08 02 12
F 30 090 02 02 01 12 b,d
F 28 080 03 03 03 22
F 67 090 10 08 01 20 a,b,e
Mean 43.8 82.5 5.5 4.7 6.6 25.1
‘five sonographic criteria’* - a: hypoechogenecity, b: irregular margin, c: microcalcification, d: intranodule vascularity, e: a shape taller than wide
Table 2. Clinical data, Results of US-guided PEI and Incidence of the ‘five sonographic criteria’ in Group B Sex Age Cystic First Infused First follow-up Last follow-up ‘Five sonographic
(yrs) portion (%) aspirate (ml) ethanol (ml) (month) (month) criteria’ Complications
M 47 070 04 04 04 14 a,b
F 45 090 02 02 05 42 a,b,d mild pain
M 71 095 30 12 02 12 a,b,e
M 49 080 02 02 08 15
F 45 095 05 05 03 24 b,c headache
F 41 085 03 03 02 30 a,
F 41 090 02 02 02 30 a,
F 57 060 08 08 03 12 mild pain
F 38 075 10 07 07 14 b
M 43 090 12 09 14 14 b,c
F 43 095 05 05 08 28 a,b,c
F 61 080 14 09 06 30 a,b
F 29 055 01 01 03 13 mild pain
F 49 100 16 12 01 12
F 51 100 02 02 05 12 a,b,c mild pain
M 49 100 05 05 03 23 a,b,c mild pain
M 49 090 04 04 03 23 a,b,c
F 55 080 02 02 03 30 a,b
F 55 060 09 09 03 30
F 44 090 04 04 05 24 a,b,e moderate pain
F 44 080 01 01 12 29 b moderate pain
F 32 095 06 06 03 12 a
F 17 090 04 04 02 12 a,b mild pain
F 39 085 06 06 04 28 mild pain
M 46 095 15 10 03 26 a,b,c
M 52 100 04 04 06 12
F 45 080 04 03 06 12 a,b,c mild pain
F 66 095 40 05 01 12
F 28 095 07 06 07 25
F 38 065 05 05 03 15 b,c,d mild pain
F 52 075 03 03 03 27 a,b,c
F 44 100 12 09 10 25 a,b,c
F 47 070 13 11 03 12
F 21 090 11 11 09 24 a,b,c mild pain & headache
F 21 100 09 09 09 24 a,b mild pain & headache
F 21 090 02 02 09 24 mild pain & headache
F 21 100 03 03 09 24 mild pain & headache
F 49 100 04 04 02 12 a,b,c
F 29 050 04 04 08 24
F 39 090 07 07 04 28
M 43 090 29 16 02 13 a,b
F 32 080 08 08 02 12 mild pain
F 49 090 08 08 01 12
F 44 080 02 03 01 26 c,e mild pain
F 12 100 06 06 06 30 a,b
M 46 090 10 07 03 17 a,b mild pain
F 35 090 04 04 03 28 mild pain
F 75 100 20 12 03 12 a,b
F 47 095 31 15 07 19 a,b,c
F 45 090 05 05 02 18 a,b
F 46 100 01 01 01 18 a,b,e
F 31 085 03 03 06 12 a,c mild pain
F 35 070 20 17 01 16 mild pain
F 36 060 10 04 01 17
F 45 100 05 05 02 16
F 47 080 07 06 03 16 moderate pain
M 62 095 17 17 03 12 a,c
M 16 100 96 20 01 20 a
F 24 100 03 03 03 12
F 42 095 04 04 08 12 a,b,e
Mean 42.1 86.9 9.8 6.4 4.4 19.6
‘five sonographic criteria’* - a: hypoechogenecity, b: irregular margin, c: microcalcification, d: intranodule vascularity, e: a shape taller than wide
well as successfully sclerosed nodules for the purely sol- id nodule without any remnant cystic portion after a fol- low-up US (Figs. 1, 2). Further, we found no thyroid nodule recurrence for the successfully post-instilled thy- roid nodules in our study. However, US-guided PEIs failed to obliterate the cystic portion of the four thyroid nodules (4.7%; two nodules in Group A and two nod- ules in Group B).
The greater the cystic portion of the thyroid nodule before US-guided PEI begins, the higher the incidence of the ‘five sonographic criteria’, which are detected by long-term follow-up US (p<0.01; Student’s t-test) (Table 3). Six nodules (6.9%; two in Group A and four in Group B) showed a complete disappearance as seen on long- term follow-up US.
For Groups A and B, three or more ‘five sonographic criteria’ were revealed in 7 (26.9%) and 17 cases (28.3%), respectively. Two or more of the ‘five sono- graphic criteria’ were detected on US in 13 (50%) and 32 cases (53.3%), respectively. One or more of the ‘five sonographic criteria’ were revealed by a US in 14 (53.8%) and 38 cases (63.3%), respectively, and no ‘five sonographic criteria’ were observed following an US in 12 (46.2%) and 22 cases (36.7%), respectively (Table 4).
The results indicates a high incidence rate of ‘five sono- graphic criteria’ in the sclerosed thyroid nodules in the two groups, and there was no statistical difference in the incidence rate of ‘five sonographic criteria’ between the two groups (p>0.05, chi-square test) (Table 4 & 5).
A B C
D E F
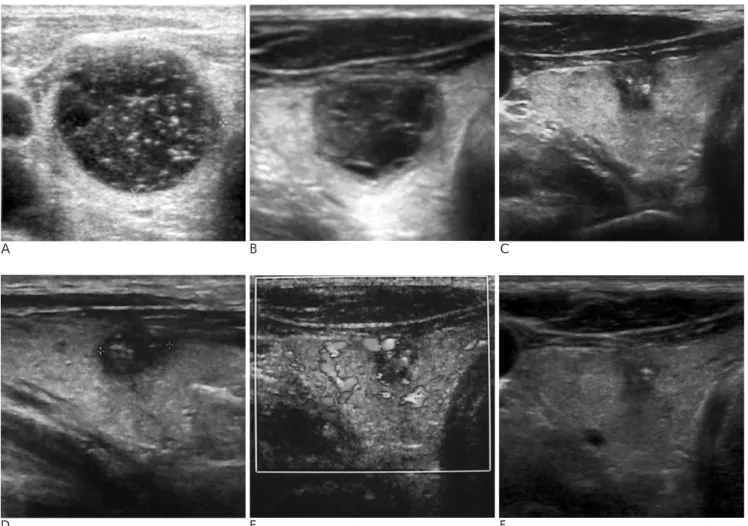
Fig. 1. A 55-year-old man with a cystic thyroid nodule in the right lobe.
A. A transverse US obtained before sclerotherapy shows a pure thyroid cyst filled with colloid material.
B. A transverse US obtained one month after sclerotherapy reveals the loss of the cystic portion of the thyroid nodule and replace- ment with hypoechoic and other echogenic portions.
C-E. A transverse, sagittal and color Dopper US obtained 15 months after sclerotherapy shows hypoechogenecity, an irregular margin, microcalcification, and a taller than wide thyroid nodule. However, this nodule shows no vascularity on a color Doppler study.
F. A transverse US obtained 22 months after sclerotherapy shows a moderate decrease in nodule size.
Discussion
Instead of the surgical removal of benign cystic thy- roid nodules, several therapeutic methods, such as per- cutaneous simple aspiration, thyroid hormone suppres-
sion therapy, percutaneous tetracycline instillation, or US-guided PEI, have been utilized (14, 15). At present, a US-guided PEI has become the first line treatment method for benign cystic or solid thyroid nodules be- cause of its ease and safety (1-8).
The instilled ethanol in the nodule, induces complex
Table 4. Incidence of the ‘Five Sonographic Criteria’ in Group A, Group B, and Total Cases (Chi-square test p>0.05 between Group A and B).
No. of Malignant Group A Group B Total cases sonographic findings (n=26) (n=60) (n=86)
≥3 07 (26.9%) 17 (28.3%) 24 (27.9%)
≥2 13 (50.0%) 32 (53.3%) 45 (52.3%)
≥1 14 (53.8%) 38 (63.3%) 52 (60.5%) 0 12 (46.2%) 22 (36.7%) 34 (39.5%) Table 3. Incidence of the ‘Five Sonographic Criteria’ according to
the Percentage of Cystic Portion in Thyroid Nodules Cystic portion Group A Group B Total
(%) (n=26) (n=60) (n=86)
50-59 0/5 (0%) 0/2 (0%) 0/7 (0%)
60-69 0/0 (0%) 0/4 (0%) 0/4 (0%)
70-79 0/1 (0%) 2/5 (40%) 2/6 (33.3%) 80-89 3/6 (50%) 5/11 (45.5%) 8/17 (47.1%) 90-100 10/14 (71.4%) 23/38 (60.5%) 33/52 (63.5%)
A B C
D E F
Fig. 2. A 46-year-old man with a cystic thyroid nodule in the left lobe
A. A transverse US obtained before sclerotherapy shows a large hemorrhagic thyroid nodule with a 90% cystic portion and with- out vascularity.
B. A transverse US obtained 3 months after sclerotherapy reveals a complete disappearance of the previous cystic portion of the thyroid nodule filled with a non-vascularized, hypoechoic component.
C-E. A transverse, sagittal and color Dopper US obtained 26 months after sclerotherapy shows hypoechogenecity, microcalcifica- tion, some blurred margins, a taller than wide sclerosed thyroid nodule with no vascularity.
F. A transverse US obtained 34 months after sclerotherapy shows a mild decrease in nodule size.
thyroid tissue damage, including coagulative necrosis, vascular thrombosis, and a hemorrhagic infarction.
Moreover, the treated areas were replaced by granula- tion tissue, which causes scarring and progressive shrinkage of the nodules (16, 17).
In the present study, we defined a ‘recurrence’ as a new cyst formation in the sclerosed portion of a thyroid nodule, following a long-term follow-up US, and a suc- cessful US-guided PEI because we focused the loss of the cystic portion in thyroid nodule. However, although an US-guided PEI, which failed to obliterate the cystic portion of the four thyroid nodules (4.7%; two nodules in Group A and two nodules in Group B), we did not ob- serve any recurring cases.
Also, among the sclerosed thyroid nodules observed in our study, 86 were observed after a first follow-up US over 12 months with a total of 45 cases revealing two or more of the ‘five sonographic criteria’ (52.3%). The high rate for the ‘five sonographic criteria’ in known benign cystic thyroid nodules, after a US-guided PEI, has a di- rect relationship with the high percentage of cystic pro- portion of these nodules. The reason for the high inci- dence of ‘five sonographic criteria’ stems from purely cystic or non-vascularized thyroid nodules, with a 90%
or greater percentage of the cystic component after the US-PEIT is uncertain. However, this result strongly sug- gests that the main component for a possible malignan- cy-mimicking, is fibrosis. Also, because of the sclerosed thyroid nodules, with a purely cystic component, ap- pear we have a high incidence of the ‘five sonographic criteria’ on US.
We evaluated the differences in success rate, compli- cations, and incidence of the ‘five sonographic criteria’,based on the aspiration or non-aspiration of in- fused ethanol, and found that no significant differences was found between the two groups.
As a result, we performed several unnecessary US- guided FNAB of benign sclerosed thyroid nodules, asso- ciated with the presence of the ‘five sonographic crite- ria’ as detected by long-term follow-up USs. In two cas-
es, we lost the patient history of the US-guided PEI.
Also, in four of the cases, we performed US-guided FNAB to rule out the presence of a new malignancy in the known sclerosed thyroid nodule. In all six cases, no malignant cells were present, despite the complete per- formance of the consecutive US-guided FNAB. In our hospital, a US-guided FNAB for a thyroid nodule is per- formed according to Yokozawa’s method (18). In addi- tion, we have achieved a high percentage of the satisfac- tory cytological results (over 90% in the first US-guided FNAB) for thyroid nodules, except for the purely cystic thyroid nodule. We are convinced that the possibility of a newly developed malignancy after a US-guided PEI was ruled out because most sclerosed nodules, with their aberrant sonographic findings, showed a gradual decrease in size after an initial follow-up US. We con- firmed several malignancy-mimicking nodules as a be- nign nodule by at least one or more satisfactory cytolog- ic results by consecutive US-guided FNAB.
In addition, over the four years of this study, we ob- served several benign cystic thyroid nodules that ap- peared as malignancy-mimicking nodules after the spontaneous collapse on long-term follow-up US.
The limitations of this study include access to regular and close long-term follow-up US for the identification of the sclerosed thyroid nodules. The laboratory correla- tions were insufficient for the purely solid or predomi- nantly solid thyroid nodules after the US-guided PEI were not included in this analysis
Conclusion
We confirmed that the long-term follow-up US of scle- rosed thyroid nodules was made in (i.e. in our hospital).
Next, the ‘fiive sonographic criteria’ were observed in half of the patients. received US-guided PEI for known benign cystic thyroid nodules. By acknowledging the possibility that sonographic findings mimic a malignan- cy the sclerosed thyroid nodule, patients may avoid an unnecessary biopsy.
References
1. Verde G, Papini E, Pacella C, Gallotti C, Delpiano S, Strada S, et al.
Ultrasound guided percutaneous ethanol injection in the treatment of cystic thyroid nodules. Clin Endocrinol 1994;41:719-724 2. Cho YS, Lee HK, Ahn IM, Lim SM, Kim DH, Choi CG, et al.
Sonographically guided ethanol sclerotherapy for benign thyroid cysts: results in 22 patients. AJR Am J Roentgenol 2000;174:213-216 3. Kim DW, Rho MH, Kim HJ, Kwon JS, Sung YS, Lee SW.
Percutaneous ethanol injection for benign cystic thyroid nodules:
Table 5. Incidence of the ‘Five Sonographic Criteria’ in the Sclerosed Thyroid Nodules
‘Five sonographic Group A Group B Chi-square
criteria’ (n=26) (n=60) test
Hypoechogenicity 11 (42.3%) 32 (53.3%) p>0.05 Irregular margin 13 (50%).0 31 (51.7%) p>0.05 Microcalcification 07 (26.9%) 17 (28.3%) p>0.05 Intranodule vascularity 03 (11.5%) 2 (3.3%) p>0.05 Shape: more tall than wide 03 (11.5%) 5 (8.3%) p>0.05
is aspiration of ethanol-mixed fluid advantagenous? AJNR Am J Neuroradiol 2005;26:2122-2127
4. Kim JH, Lee HK, Lee JH, Ahn IM, Choi CG. Efficacy of sono- graphically guided percutaneous ethanol injection for treatment of thyroid cysts versus solid thyroid nodules. AJR Am J Roentgenol 2003;180:1723-1726
5. Yasuda K, Ozaki O, Sugino K, Yamashita T, Toshima K, Ito K, et al. Treatment of cystic lesions of the thyroid by ethanol instillation.
World J Surg 1992;16:958-961
6. Monzani F, Lippi F, Goletti O, Del-Guerra P, Caraccio N, Lipolis PV. Percutaneous aspiration and ethanol sclerotherapy for thyroid cysts. J Clin Endocrinol Metab 1994;78:800-80
7. Bennedbak FN and Hegedus L. Treatment of recurrent thyroid cysts with ethanol: a randomized double-blind controlled trial. J Clin Endocrinol Metab 2003;88:5773-5777
8. Lee SJ, Ahn IM. Effectiveness of Percutaneous Ethanol Injection Therapy in Benign Nodular and Cystic Thyroid Diseases: long- term follow-up experience. Endocrine Journal 2005;52:455-462 9. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S,
Nardi F, et al. Risk of malignancy in nonpalpable thyroid nodules:
predictive value of ultrasound and color-Doppler features. J Clin Endocrinol Metabol 2002;87:1941-1946
10. Kim EK, Park CS, Chung WY, Oh KK, Kim DI, Lee JT, et al. New sonographic criteria for recommending fine-needle aspiration biopsy of non-palpable solid nodules of the thyroid. AJR Am J Roentgenol 2002;178:687-691
11. Frates MC, Benson CB, Doubilet PM, Cibas ES, Marqusee E. Can
color Doppler sonography aid in the prediction of malignancy of thyroid nodules? J Ultrasound Med 2003;22:127-131
12. Iannuccilli JD, Cronan JJ, Monchik JM. Risk of Malignancy of thy- roid nodules as assessed by sonographic criteria: the need for biop- sy. J Ultrasound Med 2004; 23:1455-1464
13. Silver RJ, Parangi S. Management of thyroid incidentalomas. Surg Clin North Am 2004;84:907-919
14. Antonelli A, Campetelli A, Di Vito A, Alberti B, Baldi V, Salvioni G. Comparison between ethanol sclerotherapy and emptying with injection of saline in the treatment of thyroid cysts. Clin Invest 1994;72:971-974
15. Hegedus L, Hansen JM, Karstrup S, Torp-Pedersen S, Juul N.
Tetracycline for sclerosis of thyroid cysts. Arch Intern Med 1988;148:1116-1118
16. Crescenzi A, Papini E, Pacella CM, Rinaldi R, Panunzi C, Petrucci L, et al. Morphological changes in a hyperfunctioning thyroid ade- noma after percutaneous ethanol injection: histological, enzymatic and sub-microscopical alterations. J Endocrinol Invest 1996;19:371- 376
17. Livraghi T, Paracchi A, Ferrari C, Reschini E, Macchi RM, Bonifacino A. The treatment of autonomous thyroid nodules with percutaneous ethanol injection: 4-year experience. Radiology 1994;190:529-533
18. Yokozawa T, Miyauchi A, Kuma K, Sugawara M. Accurate and Simple Method of Diagnosing Thyroid Nodules by the Modified Technique of Ultrasound-Guided Fine Needle Aspiration Biopsy.
Thyroid 1995;5:141-145
대한영상의학회지 2008;58:21-28
낭성 양성 갑상선 결절에 대한 에탄올 경화술 후의 장기 추적 초음파 소견:
악성 유사 초음파 소견의 빈도에 관한 연구
11인제대학교 부산백병원 영상의학과
2성균관대학교 마산삼성병원 영상의학과
박지성・김동욱・은충기・최석진・노명호2
목적: 낭성 양성 갑상선 결절에 대한 에탄올 경화술 후 장기 추적 초음파상 악성 결절의 소견을 보이는 빈도를 알 아보고자 하였다.
대상과 방법: 80명의 환자에서, 양성 결절의 소견을 보이고 적어도 한 번 이상의 세침흡인생검을 시행하여 양성으 로 확인된 갑상선 결절 86예를 대상으로 하였다. 경화술은 결절의 낭성 부위에서만 시행하였고, 시술 시 주입된 에 탄올을 뽑아 준 경우가 26예, 그대로 둔 경우가 60예였으며, 각각 그룹 A와 B로 구분하여 조사하였다. 적어도 12 개월 이상 장기 추적 초음파검사를 하였다.
결과: 86예 중 82예에서 성공적인 낭성 부위의 소실을 볼 수 있었으며, 장기 추적 초음파 에서 낭성 부위의 재발을 관찰되지 않았다. 장기 추적 초음파 에서 다섯 가지 악성 초음파 소견 중 두 가지 이상을 보이는 경우가 그룹 A와 B에서 각각 13예(50.0%)와 32예(53.3%) 이었으며, 발현 빈도에 있어서 두 그룹 간의 통계적 유의성은 관찰되지 않았다(chi-square test, p > 0.05). 또한, 결절의 낭성 부위의 비율이 높으면 높을수록 악성 초음파 소견의 빈도가 높아짐을 알 수 있었다(p < 0.01, Student’s t test).
결론: 성공적인 에탄올 경화술 후 갑상선 결절에 대한 장기 추적 초음파상 절반 이상의 환자에서 적어도 두 가지 이 상의 악성 초음파 소견이 관찰되었다. 따라서, 성공적인 에탄올 경화술 후의 갑상선 결절에 대해서 정기적인 추적 초음파를 하고, 악성 초음파 소견도 보일 수 있음을 인지함으로써 불필요한 세침흡인생검이나 수술을 피할 수 있다.