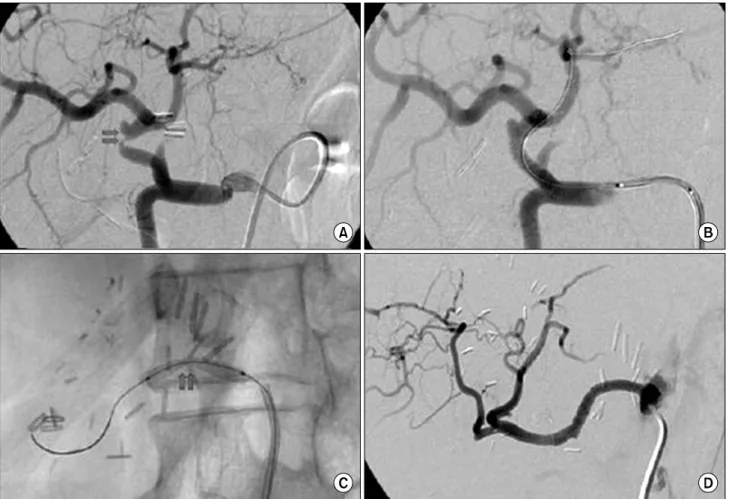
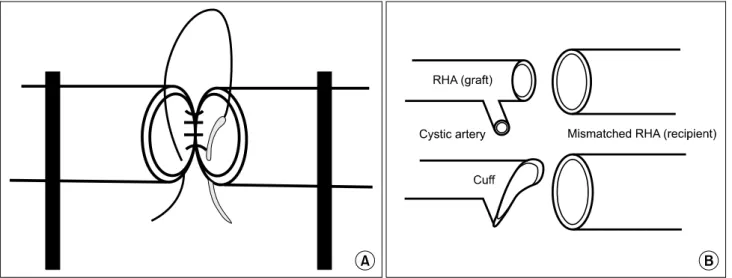
Hepatic Arterial Complications after Liver Transplantation: A Single-Center Experience
8
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
수치

관련 문서
The associations of hepatic steatosis and fibrosis using fatty liver index and BARD score with cardiovascular outcomes and mortality in patients with new‑onset type 2
In this study, we investigated the time course of neutrophil recruitment and infiltration in the early stages of arterial throm- bosis using an FeCl 3 -induced carotid
Background: Incidence of complications related extracorporeal membrane oxygenation (ECMO) support as a bridge to lung transplantation (BTT) and its association with the
MAFLD, metabolic dysfunction-associated fatty liver disease; NAFLD, nonalcoholic fatty liver disease; CVD, cardiovascular disease; CI, confidence interval; Model 1,
cACLD = compensated advanced chronic liver disease, dACLD = decompensated advanced chronic liver disease, LS = liver stiffness, LS-SIR = liver-to-spleen signal intensity
Undiagnosed malignancy in patients with deep vein thrombosis: incidence, risk indicators, and diagnosis.. Monreal M, Fernandez-Llamazares J, Perandreu
The locations of aneurysms were middle cerebral artery in 15 patients, cerebral artery in 15 patients, cerebral artery in 15 patients, cerebral artery in
Department of Education, National Center for Educational Statistics, Adult Literacy in America, National Adult Literacy Survey, 1992, Table 1.1b, p.. In addition, the United
