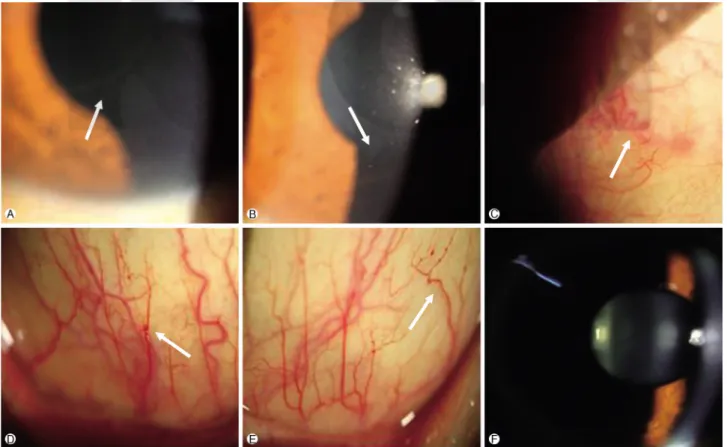
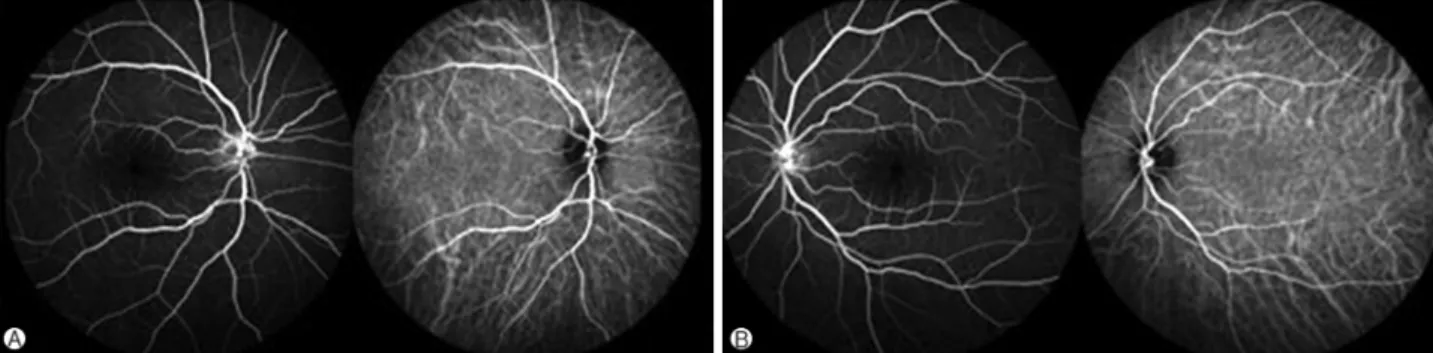
Ocular manifestations in a patient with de novo Fabry disease
4
0
0
전체 글
(2)
(3)
(4)
수치
관련 문서
This book contains hundreds of complete, working examples illustrating many common Java programming tasks using the core, enterprise, and foun- dation classes APIs.. Java Examples
De-assertion causes the NB or external clock generator to turn on the processor, and that takes place (a) in a sleep state: after a wake-up event is triggered; (b) in
As a result of the study, it was confirmed that only human resource competency had a positive(+) effect on the intercompany cooperation method of IT SMEs,
[r]
Activating mutation in the tyrosine kinase JAK2 in polycythemia vera, essential thrombocythemia and myeloid metaplasia with myelofibrosis.. A gain-of-function
A stress component is positive when it acts in the positive direction of the coordinate axes, and on a plane whose outer normal points in one of the positive coordinate
The philosophy behind the Symbiosis is that the six companies: Energy E2 Asnæs Power Station, the plasterboard factory BPB Gyproc A/S, the pharmaceutical plant Novo Nordisk
As a result of comparing with the temperature change, the coldest month mean temperature (January, February, December) showed positive value in the whole
