ISSN: 1229-6538
Korean J Clin Geri 2013;14(2):83-86
CASE REPORT
Received: July 29, 2013 Revised: December 2, 2013 Accepted: December 14, 2013.
Corresponding author: Myoung-Keun Shin
Department of Anesthesiology and Pain Medicine, Samsung Changwon Hospital, 158, Palyong-ro, Masanhoiwon-gu, Chanwon 630-723, Korea Tel: +82-55-290-6078, Fax: +82-55-290-6578, E-mail: [email protected]
Copyright Ⓒ 2013 The Korean Academy of Clinical Geriatrics
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/ licenses/by-nc/3.0) which
permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Headache without Cerebrospinal Fluid Leakage
Haeng-Seon Shim
1, Sung-Il Bae
1, Seung-Won Choi
2, Chang-Jin Oh
2, Myoung-Keun Shin
1
Department of Anesthesiology and Pain Medicine,
1Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon,
2Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Headache can occur after a lumbar epidural block. There are several reasons for the development of headache such as hypotension, postdural puncture, vascular injection, subarachnoid hemorrhage and pneumocephalus. We report a case of a 63-year-old male patient who developed a severe headache without neurologic symptoms after a lumbar epidural block with the loss of resistance technique (LORT) using air. We excluded the possibility of postdural puncture headache because there was no cerebrospinal fluid (CSF) leakage. Brain CT was performed and it revealed pneumocephalus. After conservative treatment, the patient recovered and was discharged on the fourth day of hospitalization.
Key Words: Cerebrospinal fluid leakage, Headache, Loss of resistance technique, Lumbar epidural block, Pneumocephalus
INTRODUCTION
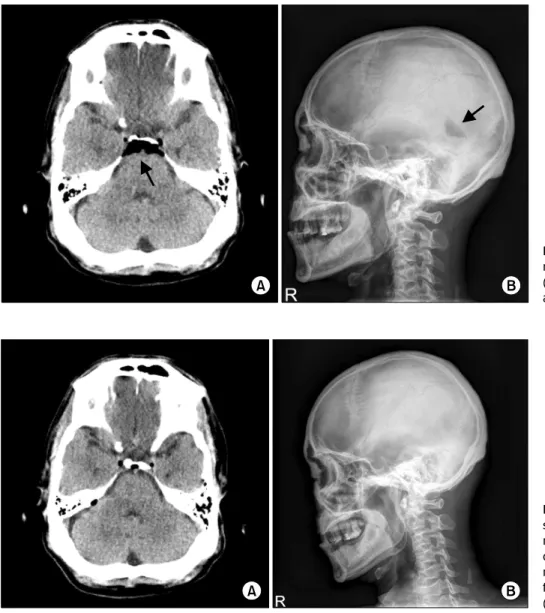
Headache can occur due to several reasons after a lumbar epidural block. Postdural puncture headache is the most common complication of unintentional dural puncture with an epidural needle. In most of the cases, headache after a lumbar epidural block is usually due to CSF leakage through the dural puncture site. If there is headache without CSF leakage after a lumbar epidural block with the loss of resist- ance technique (LORT) using air, we can consider pneumo- cephalus. We experienced a case of severe headache in a pa- tient after a lumbar epidural block and brain CT demon- strated pneumocephalus. We report a case of pneumocephalus with literature review.
CASE REPORT
A 63-year-old male patient was diagnosed with herniated intervertebral disc during orthopaedic examination. He weigh- ed 67 kg and was 169 cm tall. He complianed of numb- ness in both legs since the last 1 year. The pain in his legs was aggravated since the last 1 week. He was admitted to the orthopedics ward. He was then transferred to the pain clinic. He had no systemic diseases. He complained of a low back pain, numbness in both legs, and radicular pain.
Hence, we performed a lumbar epidural block. In the sitting
position, axenic disinfection of the back and local infiltration
with 2% lidocaine at the L4/5 level were performed. Lumbar
epidural block was performed at the L4/5 interspace with a
22 G Tuohy needle via the median approach with the LORT
using air. After the LORT using 3 ml air, an extra 3 ml air