서 론
요통이 있는 환자에서 요천추 신경근병증의 정확한 임상적 혹은 전기진단학적 평가는 환자의 진단 및 치료
에 중요하다. 임상적으로, 슬개건 반사는 요추 4번 신 경근병증을, 아킬레스건 반사는 천추 1번 신경근병증을 진단하는데 도움을 주는 것으로 알려져 있다.1 그러나 요추 5번 신경근병증을 정확히 평가할 수 있는 믿을 만
Address reprint requests to Seung Yeol Lee, MD
Department of Physical Medicine and Rehabilitation Medicine, Soonchunhyang University College of Medicine 22, Daesagwan-gil, Yongsan-gu, Seoul, 140-743, South Korea
TEL: 82-2-709-9260, FAX: 82-2-709-9265, E-mail: [email protected] 투고일: 2010년 7월 9일, 수정일: 2010년 10월 6일, 게재 확정일: 2010년 10월 6일
�No commercial party has a direct financial interest in the results of the research supporting this article, which has not and will not con- fer any benefits to the authors or any organization with which the authors are associated.
요추 5번 신경근병증 환자의 전기진단학적 후경골근 반사
순천향대학교 의과대학 재활의학교실
이양균∙박지웅∙이승열
– Abstract –
Electrodiagnostic Measurement of Posterior Tibial Reflex in Patients with L5 Radiculopathy
Yang Gyun Lee, M.D., Ji Woong Park, M.D., Seung Yeol Lee, M.D.
Department of Physical Medicine and Rehabilitation, Soonchunhyang University College of Medicine
Objective: To evaluate whether the electrodiagnostical posterior tibial reflex (PTR) will play an adjuvant role in diagnosis of L5 radiculopathy.
Methods: Fourteen L5 radiculopathy patients confirmed by routine electrodiagnostic study and age- and sex-matched 14 healthy controls were participated in this study. By using patellar hammer, latencies of PTR were evoked in both legs of each group. Average of 5 repeated PTR latencies were calculated and the difference of the PTR latencies between right and left leg (PTR-D) were compared between two groups. Receiver operating characteristic (ROC) curve was used to determine optimal cut off values of PTR-D in diagnosing L5 radiculopathy.
Results: Mean PTR latency in affected legs showed significantly longer value than that in unaffected legs in unilateral L5 radiculopathy group (p<0.05). And, mean value of PTR-D in L5 radiculopathy group was significantly greater than that in control group (p<0.05). PTR-D threshold of 10.0 ms yielded the greatest sensitivity (93%) and specificity (93%) for the diagnosis of L5 radiculopathy.
Conclusion: As the PTR latency represented large inter-individual differences, the PTR-D can be used as an optimal parameter for the inter-individual comparison. Furthermore, PTR-D with 10.0 ms threshold gives best diagnostic discrimination for the diagnosis of L5 radiculopathy.
Key Words: Posterior tibial reflex, Electrodiagnostic measurement, Radiculopathy
한 심부건 반사는 없다. 내측 슬굴곡근,2,3 비골근,4 전 경골근,5 무지신근6의 신장 반사 등이 이전에 연구되었 지만, 요추 5번 신경근병증에 대한 민감도나 특이도가 정확하게 정의되지 않았다. 이후에 단무지신근 반사에 대한 연구가 있었지만, 민감도가 낮았고, 요추 5번과 천추 1번 신경근병증을 감별할 수 없었다.7 후경골근 반 사는 임상적으로 요추 5번 신경근병증을 감별하는 데 민감한 반사로 알려져 있으나,8 정량적으로 전기진단학 적 방법을 통해 검사한 연구는 현재까지 보고된 바가 없다.
본 연구의 목적은 요추 5번 신경근병증 환자군과 정상 대조군을 대상으로 하여 전기진단학적 후경골근 반사 (posterior tibial reflex, PTR)를 측정해 봄으로써, 이 검사가 요추 5번 신경근병증의 진단에 특이성이 있는 지를 밝히고, 통상적인 전기진단방법 외에 사용될 수 있 는 유용한 보조적 검사 방법인지를 확인하는데 있다.
연구 대상 및 방법
1) 연구 대상
요추 5번 신경근병증 환자군의 선택 기준은 최근에 요통이나 하지로의 방사통이 있는 환자 중에서 1) 비대 칭적인 요추 5번 신경의 피부분절에 감각저하, 2) 요추 5번 신경의 지배를 받는 근육의 비대칭적 근력저하, 3) 하지 직거상 검사의 양성 소견 중 적어도 하나 이상의
임상 소견이 관찰되고, 컴퓨터 단층 촬영이나 자기 공 명 영상에서 요추 4, 5번 추간판 탈출을 확인하고 침근 전도 검사에서 요추 5번 신경근의 지배를 받는 근육의 비정상자발전위를 관찰한 경우로 하였다. 본 연구에는 상기 기준을 만족하는 32명의 요추 5번 신경근병증 환 자군 중 말초 신경병증 혹은 포착성 신경병증 등의 말 초 신경이상이나 말초 혈관 질환, 양측성 신경근병증, 요추 5번 이외의 다른 레벨의 신경근병증이 동반된 환 자를 제외하였고, 후경골근 반사가 양하지 또는 병변 측 하지에서 발현되지 않은 경우도 대상에서 제외하여 총 14명의 환자가 최종적으로 분석의 대상이 되었다.
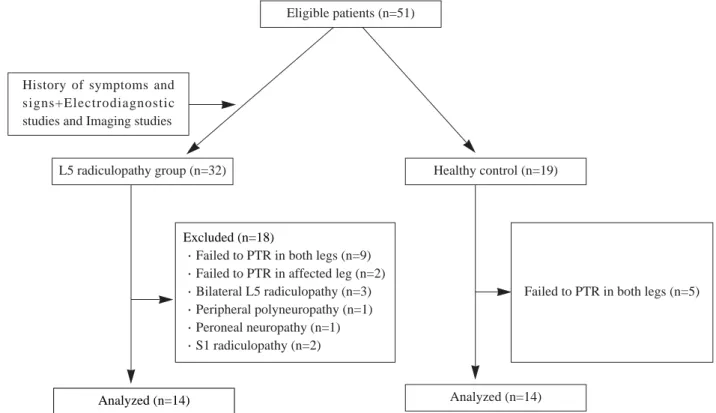
정상 대조군은 환자군과 성별 및 연령을 맞추어 선정 하였고, 이들은 최근 6개월 이내의 요통, 당뇨, 주 5회 이상의 음주 습관, 신경근병증, 말초 혈관 질환, 말초 신경병증, 이전의 요추부위의 수술 경험, 감각 저하, 하지 근력 약화가 없는 자로 하였고, 총 19명의 참여자 중 양측 하지에서 후경골근 반사가 관찰된 14명을 대상 으로 하였다(Fig. 1).
2) 후경골근 반사(PTR)의 검사방법
우선 대상자를 편안하게 앙와위로 눕힌 상태에서 동 심바늘전극을 후방 접근법을 이용하여, 경골 거친면에 서 한 손 너비만큼 하방, 그리고 내측 경골 모서리에서 한 손가락 너비만큼의 간격을 두고 삽입하여 후경골근 에 위치 시켰고, 전기 자극을 주어 발목의 내전이 나타
Fig. 1. Flow chart of the study.
Analyzed (n=14)
Excluded (n=18)
∙Failed to PTR in both legs (n=9)
∙Failed to PTR in affected leg (n=2)
∙Bilateral L5 radiculopathy (n=3)
∙Peripheral polyneuropathy (n=1)
∙Peroneal neuropathy (n=1)
∙S1 radiculopathy (n=2)
Failed to PTR in both legs (n=5)
Analyzed (n=14) Eligible patients (n=51)
History of symptoms and signs+Electrodiagnostic studies and Imaging studies
L5 radiculopathy group (n=32) Healthy control (n=19)
나는지 확인하였다.9,10 주상골 근처의 후경골근 힘줄을 patella hammer (VIASYS Healthcare, War- wick, United kingdom)로 가볍게 두들겨 후경골근 반사를 유발하였고(Fig. 2), 유발된 후경골근 반사는 동심바늘전극을 통하여 기록되었다. 상기 검사는 두 군 모두 양측 하지에서 각각 측정하였다. 후경골근 반사의 잠시(latency)는 자극 후 파형이 변화하기 시작하는 지
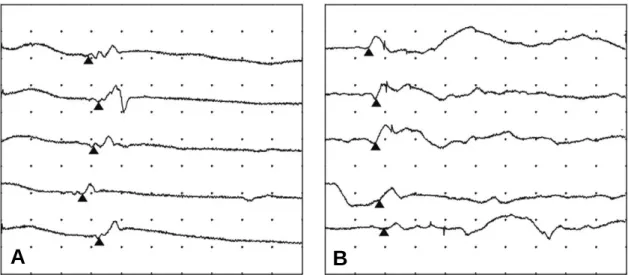
점까지의 시간으로 하였고, 모양이 비슷한 파형을 5번 반복하여 측정한 후 이들의 평균값을 구하여‘PTR-잠 시’로 정하였다(Fig. 3). 이 때 진폭(amplitude)은 측 정 시 마다 매우 다양하게 나타났기 때문에 분석에서 제외하였다. 그 후 양 하지에서 측정된 PTR-잠시 간의 차이를 계산하여‘PTR-편차’로 정하였다.
3) 통계 분석
본 연구의 자료는 SPSS for Windows (version 14.0)을 사용하여 분석하였다. 각 군의 PTR-잠시와 PTR-편차를 비교하기 위해서는 독립표본 t 검정을 사 용하였다. 요추 5번 신경근병증의 정량적인 진단을 위 하여 receiver operating characteristic (ROC) 곡 선을 이용하여 PTR-편차의 역치값에 대한 민감도와 특 이도를 측정하였다. 연령과 PTR-잠시, 그리고 유병기 간과 PTR-편차에 대한 상관관계를 분석하기 위해 피어 슨 상관계수(Pearson’s correlation coefficient)를 이 용하였다. 통계적 유의수준은 p값 0.05 미만인 경우로 정하였다.
결 과
요추 5번 신경근병증 환자군은 총 14명으로 남자는 7 Fig. 2. Posterior tibial reflexes (PTR) were evoked by tap-
ping the tibialis posterior tendon near navicular bone with a patellar hammer. The PTR latencies were recorded by concentric needle electrode inserted in the tibialis posterior muscle belly.
Fig. 3. Electrodiagnostic PTR latencies were indicated in affected leg (A) and unaffected leg (B) of right L5 radicu- lopathy patient (solid triangles). Settings: sweep speed, 100 ms per division; sensitivity, 200 μV per division; high frequency filter, 5 kHz.
A B
Table 1. Baseline Demographics
L5 radiculopathy (n=14) Healthy control (n=14) p value
Age (year) 48.4±13.1 47.4±15.6 0.856
*Sex (male:female) 7:7 7:7 Matched
Duration (day) 126.8±184.3 Not applicable
Values are mean±standard deviation and *number of subjects
명, 여자는 7명이었고, 평균 나이는 48.4±13.1세 (27~71세)이었으며, 평균 유병기간은 126.8±184.3일 (27~660일)이었다. 정상 대조군은 총 14명으로 남자 가 7명, 여자가 7명이었고, 평균 나이는 47.4±15.6세 (20~73세)이었다(Table 1).
PTR-잠시는 요추 5번 신경근병증환자의 경우는 병변 측에서 43.84±17.45 ms, 건측에서 23.81±12.42 ms 로 병변측에서 유의하게 증가되어 있었으나(p=0.002;
95% CI, 8.26~31.80), 정상 대조군의 경우에서는 우 측에서 30.71±5.50 ms, 좌측에서 28.00±6.74 ms로 양측 하지에서 차이가 관찰되지 않았다(p=0.256; 95%
CI, -2.08~7.49) (Fig. 4).
편측 요추 5번 신경근병증 환자군의 평균 PTR-편차 값은 20.03±11.24 ms였고, 정상 대조군의 평균 PTR- 편차 값은 3.33±4.29 ms로 환자군에서 대조군 보다 유의하게 높았다(p<0.001, 95% CI, 9.91~23.49) (Fig. 5).
정상 대조군의 양하지와 환자군의 건측 하지에서 측 정한 PTR-잠시와 연령과의 상관관계를 분석하였을 때 유의한 연관성은 보이지 않았다(r=0.190, p=0.228).
또한 요추 5번 신경근병증환자의 PTR-편차와 유병기 간과의 상관관계에서도 유의한 연관성은 관찰되지 않았 다(r=0.229, p=0.431).
요추 5번 신경근병증을 진단하기 위한 정량적 PTR-
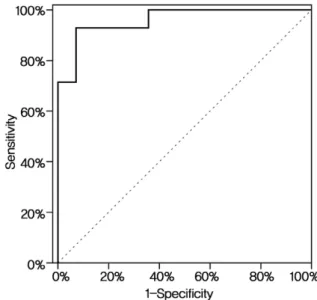
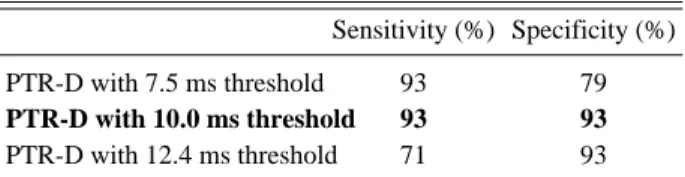
편차의 역치값을 구하였는데, ROC 곡선 분석을 하였 을 때 PTR-편차의 역치값이 10.0 ms일 때 민감도가 93%, 특이도가 93%로 가장 높게 나타났다(Table 2, Fig. 6).
고 찰
이전의 연구를 살펴보면, 신경근병증 환자에서 임상
Fig. 4. Mean values with standard deviation bars were demon- strated. The mean values of PTR-lat were compared between affected and unaffected leg in L5 radiculopathy group, and between right and left leg in control group. In L5 radiculopathy group, prolonged latency was found in affected leg than unaf- fected leg.
PTR-lat: latency of posterior tibial reflex, L5 rad: L5 radicu- lopathy group. *p<0.05
Fig. 5. Mean values with standard deviation bars were demon- strated. The mean values of PTR-D were compared between the L5 radiculopathy group and the control group. Greater value was found in L5 radiculopathy group than that in control group.
PTR-D: the difference of the posterior tibial reflex latencies between right and left leg, L5 rad: L5 radiculopathy group.
*p<0.05
Fig. 6. Receiver operating characteristic (ROC) curve of the PTR-D (solid line) is illustrated to predict L5 radiculopathy.
An area under the curve (AUC) of 1.0 is characteristic of an ideal test, whereas an AUC of 0.5 or less indicates a test of no diagnostic value. The AUC of PTR-D was 0.959.
적으로는 정상 심부건 반사를 보인 환자들이 전기진단 학적으로 측정된 건반사에서는 종종 잠시가 연장되어 나타났다는 보고가 있었고,11 만성 탈수초 다발성 신경 병증 환자에서도 임상적인 건반사보다 전기진단학적으 로 측정된 슬개건 혹은 아킬레스건 반사가 더 자주 이 상소견을 보였었다는 것에 주목할 필요가 있다.12
Felsenthal과 Reischer2는 요추 5번 신경근병증을 예측할 수 있는 비대칭적인 내측 슬굴곡근 반사가 있다 고 하였으나, 대상 개체수가 7명으로 적어 제한점이 있 었다. 하지만 Rico와 Jonkman13은 요추 5번 신경근을 반영하는 적당한 단일연접반사는 없으며, 이 때문에 요 추 5번 신경근병증을 진단하는데 가장 좋은 것은 침 근 전도 검사라고 발표하기도 하였다. 이후, Jensen3은 요 추 5번 신경근병증의 진단을 위해 내측 슬굴곡근 반사 를 이용하여 85~89%의 양성 예측치와 51~61%의 음 성 예측치를 보고 하였고, Stam5은 전기진단학적으로 전경골근 반사를 측정하였는데, 32번의 타진을 한 후 평균값을 구하여 요추 5번 신경근병증을 진단하였을 때, 72%의 민감도를 보고 하였다. 이 때, 각각의 측정 시 마다 진폭과 잠시는 모두 다양하게 나타났다고 하였 는데, 이번 연구에서도 후경골근 반사의 진폭과 잠시는 매우 다양하게 나타났다.
본 연구에서는 확인된 정량적인 전기진단학적‘PTR- 잠시’는 개인간의 차이가 매우 크기 때문에 이 값을 직 접적으로 진단에 적용하는 것은 불가능하다고 판단하 여, 이를 보정하기 위하여 저자들은 개인의 좌측과 우 측의 후경골근 반사의 잠시간의 차이인‘PTR-편차’를 이용하여 두 군의 결과를 분석하였다.
요추 5번 신경근병증 환자군의 평균 PTR-편차 값은 정상 대조군 보다 유의하게 높았으며(p<0.001), PTR- 편차의 역치값이 10.0 ms일 때 가장 높은 민감도와 특 이도를 보였다. 이는 이전 연구와 비교하였을 때, 요추 5번 신경근병증을 진단하는 데 있어서 상대적으로 높은 민감도와 특이도를 보인 것으로 전기진단학적인 후경골 근 반사가 이전에 연구되었던 다른 건반사보다 임상적 인 가치가 더 있다 할 수 있겠다. 또한 임상적 후경골 근 반사에서는 슬개건 반사나 아킬레스 건반사처럼 눈 으로 확인될 만큼의 뚜렷한 반사가 일관되게 나타나지 않는 경우에도 전기진단학적 방법으로 유의한 검사값을
얻을 수 있다는 점에서 의미가 있다.
본 연구의 제한점은 다음과 같다. 첫째, 몇 몇 환자에 서는 타진 시 심한 압통을 호소하여 반복 검사 시 어려 움이 있었다. 둘째, 전기진단학적 후경골근 반사 검사 에서 정상 대조군의 26.3%(5/19)에서 검사 시 반응을 보이지 않았는데 이는 후경골근 반사를 이용한 검사법 이 모든 환자에서 적용될 수 없음을 나타낸다. 이러한 이유는 후경골근의 힘줄이 상대적으로 크기가 작고, 후 경골근이 접합하는 주상골이 상대적으로 돌출되어 있어 정확히 후경골근의 힘줄을 타진하기가 힘들기 때문인 것으로 생각된다. 셋째, 본 연구에서 건측의 하지에서 는 전기진단학적 후경골근 반사가 유발되었으나 환측 하지에서는 유발되지 않은 환자가 2명이 있었는데, 이 는 후경골근 반사가 유발되지 않을 정도의 심한 신경근 병증을 가지는 환자는 이 검사 방법을 적용할 수 없다 는 제한점을 시사한다. 마지막으로 요추 5번 이외의 요 추 3, 4번과 천추 1번 신경근병증 환자를 대상으로 하 지 않았기 때문에 이 검사법이 과연 요추 5번 신경근병 증 환자에서만 민감한 검사인지는 확인하지 못하였다.
향후 보다 많은 요추 5번 신경근병증 환자를 대상으 로 하고, 요추 5번 주변 다른 레벨의 신경근병증 환자 를 대상군에 추가하여 요추 5번 신경근병증 환자의 결 과와 비교하는 연구가 필요할 것으로 생각된다.
결 론
임상적으로 진단이 쉽지 않은 요추 5번 신경근병증의 진단에 있어 기존 전기진단학적 검사 방법 외에 후경골 근 반사의 검사가 보조적인 진단방법으로 이용될 수 있 겠고, 이 중 PTR-편차 값이 민감도와 특이도가 높은 유용한 검사 지표로 사용될 수 있으리라 생각된다.
참고문헌
1. Hoppenfeld S, Hutton R: Physical examination of the spine and extremities, 1st ed, East Norwalk: Appleton- Century-Crofts, 1976, pp251-253.
2. Felsenthal G, Reischer MA: Asymmetric hamstring reflex- es indicative of L5 radicular lesions. Arch Phys Med Rehabil 1982: 63: 377-338.
3. Jensen O: The medial hamstring reflex in the level-diagno- sis of a lumbar disc herniation. Clin Rheumatol 1987: 6:
570-574.
4. Berlin L: A peroneal muscle stretch reflex. Neurology 1971: 21: 1177-1178.
5. Stam J: The tibialis anterior reflex in healthy subjects and in L5 radicular compression. J Neurol Neurosurg Psychia- try 1988: 51: 397-402.
Table 2. Sensitivity and Specificity of the Measuring Parame- ters in Diagnosing L5 Radiculopathy
Sensitivity (%) Specificity (%)
PTR-D with 7.5 ms threshold 93 79
PTR-D with 10.0 ms threshold 93 93
PTR-D with 12.4 ms threshold 71 93 PTR-D: the difference of the posterior tibial reflex latencies between right and left leg
6. Taylor TK, Wienir M: Great-toe extensor reflexes in the diagnosis of lumbar disc disorder. Br Medl J 1969: 2: 487- 489.
7. Marin R, Dillingham TR, Chang A, Belandres PV: Exten- sor digitorum brevis reflex in normals and patients with radiculopathies. Muscle Nerve 1995: 18: 52-59.
8. Palmer ML, Epler ME: Fundamentals of musculoskeletal assessment techniques, 2nd ed, Philadelphia: Lippincott Williams & Wilkins, 1998, pp363.
9. Geiringer SR, Davidson S: Anatomic localization for nee- dle electromyography, 2nd ed, Philadelphia: Hanley &
Belfus, 1999, pp104-105.
10. Perotto AO, Delagi EF, Iazzetti J, Morrison D: Anatomi-
cal guide for the electromyographer: The limbs and trunk, 4th ed, Springfield: Charles C Thomas, 2005, pp194-196.
11. Malcolm DS: A method of measuring reflex times applied in sciatica and other conditions due to nerve-root compres- sion. J Neurol Neurosurg Psychiatry 1951: 14: 15-24.
12. Kuruoglu HR, Oh SJ: Tendon-reflex testing in chronic demyelinating polyneuropathy. Muscle Nerve 1994: 17:
145-150.
13. Rico RE, Jonkman EJ: Measurement of the Achilles ten- don reflex for the diagnosis of lumbosacral root compres- sion syndromes. J Neurol Neurosurg Psychiatry 1982: 45:
791-795.