서 론
근감소증(sarcopenia)은 신체 위약의 대표적인 특징으로서 근육 의 양과 근력의 감소로 정의1)되는 개념으로 다양한 원인에 의해 발 생한다. The European Working Group on Sarcopenia in Older People (EWGSOP)2)는 근감소증을 일차성 근감소증과 이차성 근감소증으 로 구분하였는데, 일차성 근감소증은 노화 이외에 다른 원인이 없는
경우로 정의하였고, 이차성 근감소증은 노화 이외의 다른 원인(좌식 생활에 의한 신체활동의 감소, 영양 불균형, 암, 심뇌혈관질환 등의 중증 질환)에 의해 발생한 경우로 정의하였다. 이러한 근력의 저하는 당뇨, 심혈관질환 등 만성 질환자에서 더 크게 발생3,4)하고, 근감소증 은 각종 신체기능의 감소 및 장애를 유발해 삶의 질에 영향을 미치 게 된다.
최근에는 건강이란 개념5)이 단순한 생명 연장뿐 아니라 삶의 질 Received March 8, 2017 Revised July 30, 2017 Accepted August 7, 2017
Corresponding author Ji-Ho Choi Tel: +82-32-890-3547, Fax: +82-32-890-2195 E-mail: [email protected]
Copyright © 2017 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2017.7.6.870 eISSN 2233-9116
Korean J Fam Pract. 2017;7(6):870-876
Korean Journal of Family Practice
KJFP
한국 성인의 근감소증과 건강 관련 삶의 질과의 연관성:
제5기 국민건강영양조사 자료 이용(2010-2011년)
오정민, 최지호*, 이연지, 이유림, 윤남희, 송현진
인하대학교 의과대학 가정의학교실
Association between Sarcopenia and Health-Related Quality of Life in Korean Adults: Based on the Fifth Korean National Health and Nutrition Examination Survey (2010-2011)
Jeong Min Oh, Ji-Ho Choi*, Yeon Ji Lee, Yu Rim Lee, Nam Hee Youn, Hyeun Jin Song Department of Family Medicine, Inha University College of Medicine, Incheon, Korea
Background: Sarcopenia is defined as a loss of muscle mass leading to decreased muscle strength, physical activity, and increased mortality. Health- related quality of life (HRQoL) has been identified as a factor in various medical outcomes including death, and has become an important consideration in health care. We aimed to analyze the association between sarcopenia and HRQoL in Korean adults older than 19 years.
Methods: We included 2,300 men and 2,849 women who participated in the Korea National Health and Nutrition Examination Survey from 2010 to 2011. Sarcopenia was defined as appendicular skeletal muscle mass divided by weight (%) below 2 standard deviations of the sex-specific mean for young adults. The cutoff point for sarcopenia was 29.1% in men and 23.0% in women. HRQoL was measured with the Euro quality of life-5 dimension (EQ-5D) instrument. Logistic regression analysis was performed to evaluate the relationship between sarcopenia and HRQoL.
Results: The prevalence of sarcopenia was 14.5% in men and 19.7% in women. The EQ-5D index score was significantly lower and the rate of difficulty with individual components of HRQoL was higher in the sarcopenic group. After adjustment for age, body mass index, lumbar spine BMD, chronic disease, smoking, alcohol, regular exercise, and education, the odds ratios for problems with mobility were 1.62 in men and 1.31 in women;
however, the difference was not statistically significant for women.
Conclusion: Sarcopenia was associated with poor quality of life, especially with regard to mobility and depression/anxiety. Greater consideration of sarcopenia is needed at a younger age to prevent and manage poor quality of life at an older age.
Keywords: Sarcopenia; Euro Quality of Life-5 Dimension; Health-Related Quality of Life
오정민 외. 한국 성인의 근감소증과 건강 관련 삶의 질과의 연관성 Korean Journal of Family Practice
KJFP
을 중시하는 방향으로 나아가고 있는데, 건강 관련 삶의 질(health related quality of life, HRQoL)이 사망이나 재입원 같은 다양한 의료 결과에 영향을 미치는 독립요인으로 알려지면서6,7) 보건의료 중재의 중요한 고려사항이 되고 있다.
근감소증은 보통 노년층에서 논의되고 있는 문제이지만, seden- tary lifestyle에 익숙한 청장년층에서도 이차성으로 발생할 수 있는 건강 문제로, 본 연구에서는 우리나라 만19세 이상의 전체 성인 인구 를 대상으로 하여 남성과 여성을 나누어 각각에서 근감소증과 건강 관련 삶의 질의 관계를 알아보고, 각 연령대별로 근감소증과 건강 관련 삶의 질과의 연관성에 어떤 차이가 있는지를 파악하고자 한다.
방 법
1. 연구 대상
본 연구는 제5기 1, 2차년도 국민건강영양조사(2010–2011년)에 참 여한 만19세 이상의 대한민국 성인 남녀를 대상으로 하였다. 전체 17,476명 중 신체계측 및 dual energy X-ray absorptiometry (DEXA) 미 시행자, EuroQoL 5 dimension (EQ-5D) 설문 항목 무응답자, 삶의 질 에 영향을 줄 수 있는 중증질환(악성종양 및 신부전, 뇌혈관질환, 심 장혈관질환, 간경변증)을 가진 경우를 제외하고, 근감소증에 영향을 줄 수 있는8) 비만도, 흡연 여부, 교육수준, 규칙적 운동에 대한 정보 를 얻을 수 있는 남성 2,300명, 여성 2,849명, 총 5,149명을 분석대상으 로 하였다.
2. 근감소증의 정의
현재 근감소증을 정의하는 여러 기준이 제시되고 있지만, 표준화 된 진단 기준은 없는 실정으로, 본 연구에서는 이중 에너지 방사선 흡수 계측기(DEXA)로 양측 상하지 근육량(appendicular skeletal muecle)을 측정하였으며, 제4기 국민건강영양조사 자료를 이용한 Kim 등9)의 근감소증 진단법에 따라 양측 상하지 근육량을 체중으 로 나눈 후 100을 곱한 값이 젊은 성별 기준 집단 평균값의 2 표준편 차 미만인 값을 근감소증으로 정의하였고, 절단값(cutoff value)은 남 성 29.1%, 여성 23.0%를 적용하였다.
3. 건강 관련 삶의 질 측정
건강 관련 삶의 질(HRQoL)을 측정하는 도구로 EQ-5D10)를 사용 하였다.
EQ-5D는 EuroQol 그룹에서 개발한 선호도 기반 HRQoL 측정도 구로써 현재의 건강상태를 묻는 5개의 문항으로 구성된 EQ-5D와 온 도계 형식의 시각 아날로그 척도인 Euro quality of life-visual analogue
scale (EQ-VAS), 그리고 우리나라 평가 기준을 적용하여 가중치를 계 산한 EQ-5D index11,12)로 평가하였다.
EQ-5D는 ‘운동능력’, ‘자가관리’, ‘일상활동’, ‘통증/불편’, ‘불안/우울’
로 각 5개 차원에 대하여 ‘문제없음, 다소 문제 있음, 심각한 문제 있 음’의 3가지 수준으로 평가13)하고, EQ-VAS는 오늘 자신의 전반적인 건강수준을 최저 건강상태인 0점부터 최고의 건강상태인 100점까 지로 20 cm 수직자 막대에 표시하여 나타냈다. EQ-5D index는 완전 한 건강상태 1부터 가장 낮은 점수 –0.171까지의 가중 지표값으로 계 산한다.
본 연구에서는, EQ-5D 5개 차원의 3가지 응답을 다시 2가지로 분 류(문제없음, 문제 있음)하여 문제를 호소한 분율과 EQ-VAS, EQ-5D index의 평균과 표준편차를 제시하였다.
4. 국민건강영양조사 자료 활용 방법
제5기 1, 2차년도 국민건강영양조사(2010–2011년) 원시자료 중 건 강면접조사와 보건의식행태 조사자료에 포함된 나이, 비만도, 운동, 흡연, 음주, 소득수준을 이용하였고, 골밀도 체지방 검사를 이용하 였다.
음주는 한 달에 1회 이상 술을 마시는 경우로, 비음주는 한 달에 1 회 미만으로 마시는 경우로 구분하였으며, 1989년 세계보건기구 (World Health Organization)가 개발한 alcohol use disorder identifica- tion test (AUDIT)13) 10문항 자가보고용 설문을 시행해 10개 항목 점 수 총합이 12점 이상을 문제 음주군, 12점 미만을 정상 음주군으로 분류하였다. 흡연력은 설문 응답에 따라 과거 흡연, 현재 흡연, 비흡 연자로 분류하였으며, 운동행태는 international physical activity ques- tionnaire 를 참고하여, 격렬한 신체활동을 1회 20분 이상, 주 3회 이상 실천하거나 중등도 신체활동을 1회 30분 이상, 주 5회 이상 실천한 경우에 규칙적 운동을 한 것으로 정의하였다. 교육수준은 교육을 받은 기간에 따라 9년 이하, 10–15년, 16년 이상의 그룹으로 분류하 였다. 신체계측은 이동 검진 차량에서 직접 계측을 하였으며, 신장과 체중은 각각 0.1 cm과 0.1 kg까지 측정하였고, 체질량지수는 (체중 [kg]/신장의 제곱[m2]) 식을 이용하여 계산하였다.
5. 통계 분석
통계분석은 질병관리본부의 국민건강영양조사 원시자료 이용지 침에 따라 가중치를 사용하여 survey 분석을 시행하였다. 근육량은 성별에 따라 차이가 있어 남녀 간 절대적 비교가 어려워 본 연구는 근감소증과 건강 관련 삶의 질의 관계를 성별을 나누어 각각 분석하 였다. 각 성별에 따른 연구 대상자들의 일반적 특성을 연속변수는 독립표본 t-검정을 이용하여 평균±표준오차로 제시하였고, 범주변
Original Article
Korean Journal of Family Practice
Jeong Min Oh, et al. Association between Sarcopenia and HRQoL in Korean Adults
Korean Journal of Family Practice
KJFP
수는 카이제곱검정을 이용하여 빈도(백분율)로 제시하였다. 각각 남 성과 여성의 연령그룹별 근감소증과 HRQoL과의 연관성을 파악하 기 위해 독립표본 t-검정과 일원분산분석을 이용해 평균±표준오차 로 제시하였으며, 근감소증과 EQ-5D의 연관성을 확인하기 위해 로 지스틱 회귀분석을 이용하여 분석하였고, 연령, 체질량지수, 요추 골 밀도를 보정한 모형(model 1), model 1에 만성 질환 현재 유병 유무(고 혈압, 이상지질혈증, 관절염, 갑상선질환, 천식, 폐결핵, 아토피피부염) 을 보정한 모형(model 2), model 2에 흡연력, 음주력, 규칙적 운동 여 부, 교육수준을 보정한 모형(model 3)을 이용하여 유의성을 확인하 였다.
분석결과에는 교차비와 95% 신뢰구간을 제시하였다. 통계분석은
IBM SPSS statistics ver 22.0 (IBM Co., Armonk, NY, USA)을 이용하여 시행하였고, 통계적 유의수준은 P-value<0.05로 하였다.
결 과
1. 연구 대상자의 일반적인 특성
Table 1에서 연구 대상자들의 일반적 특성을 성별로 나누어 표기 하였다. 남성 2,300명, 여성 2,849명으로, 남성은 평균 연령은 49.02±15.777세, 사지근육량 22.06±3.365 kg, 근감소증 유병률은 14.5%
였으며, EQ-5D에서 통증/불편 문제 호소 비율이 17.4%로 가장 높았 고, 그 다음으로 운동능력의 문제 호소비율이 9.8%로 나타났다. 여성 의 평균 연령은 45.49±14.830세, 사지근육량 14.36±2.144 kg, 근감소증 유병률은 각각 19.7%, EQ-5D 중 통증/불편 문제 호소비율이 24.7%로 가장 높고, 그 다음으로 운동능력의 문제가 12.8%로 나타났다.
Table 1. Baseline characteristics of study population according to sex from KNHANES 2010–2011
Chracteristic Male
(n=2,300)
Female (n=2,849)
Mean age (y) 49.02±15.777 45.49±14.830
Age categories (y)
19–39 745 (32.4) 1,158 (40.6)
40–59 884 (38.4) 1,137 (39.9)
≥60 671 (29.2) 554 (19.4)
Body mass index (kg/m2) 23.98±3.093 23.13±3.436 Appendicular skeletal muscle (kg) 22.06±3.365 14.36±2.144 Skeletal muscle index*(%) 31.96±2.782 25.15±2.446
Sarcopenia 333 (14.5) 562 (19.7)
Osteoporosis (T–score≤–2.5) 79 (3.4) 289 (10.1) EQ–5D
EQ–5D index 0.96±0.096 0.94±0.112
EQ–VAS 75.63±15.762 73.09±17.505
Problem of mobility 225 (9.8) 364 (12.8)
Problem of self care 60 (2.6) 83 (2.9)
Problem of usual activity 131 (5.7) 238 (8.4) Problem of pain/discomfort 401 (17.4) 705 (24.7) Problem of anxiety/depression 131 (5.7) 345 (12.1) Education (y)
≥16 739 (32.1) 705 (24.7)
10–15 961 (41.8) 1257 (44.1)
≤9 600 (26.1) 887 (31.1)
Alcohol (≥1 time/mo) 1,850 (80.4) 1,361 (47.8)
AUDIT (score≥12) 857 (37.3) 184 (6.5)
Smoking
Non–smoker 413 (18.0) 2487 (87.3)
Ex–smoker 923 (40.1) 197 (6.9)
Current smoker 964 (41.9) 165 (5.8)
Regular exercise
Regular 1,172 (51.0) 1,301 (45.7)
Irregular 1,128 (49.0) 1,548 (54.3)
Values are presented as number (%) or mean±standard error.
KNHASNES, Korean national health and nutrition examination survey; EQ–5D, Euro quality of life–5 dimension; EQ–VAS, Euro quality of life–visual analogue scale; AUDIT, alcohol use disorder identification test.
*Appendicular skeletal muscle/weight (kg).
Table 2. Mean SMI and prevalence of sarcopenia according to age of the gender
Variable Male (n=2,300) Female (n=2,849) Age (y)
19–39
SMI 32.687±2.838 25.801±2.392
Sarcopenia 73/745 (9.8) 145/1,158 (12.5) 40–59
SMI 31.918±2.548 24.850±2.250
Sarcopenia 115/884 (13.0) 247/1,137 (21.7) ≥60
SMI 31.207±2.809 24.383±2.604
Sarcopenia 145/671 (21.6) 170/554 (30.7) Values are presented as mean±standard error or number (case/total, %).
SMI, skeletal muscle index (%)=appendicular skeletal muscle/weight (kg).
P–values represent prevalence of sarcopenia according to age group by analysis of variance for continuous variable and chi–square test (P<0.05).
Table 3. The association of sarcopenia and HRQoL according to the age of the gender
Age Male Female
EQ-5D index EQ-VAS EQ-5D index EQ-VAS Normal (y)
19–39 0.98±0.06* 77.39±12.93* 0.98±0.06* 75.33±14.27* 40–59 0.97±0.08* 77.84±14.75* 0.96±0.08* 75.31±16.21* ≥60 0.92±0.14* 72.46±8.25* 0.86±0.18* 66.04±22.81* Sarcopenia (y)
19–39 0.97±0.07* 71.89±16.07 0.97±0.06* 72.70±15.69* 40–59 0.96±0.09* 73.03±16.09 0.93±0.11* 71.48±17.42* ≥60 0.93±0.11* 71.21±19.21 0.84±0.16* 66.64±22.74* Values are presented as mean±standard error.
HRQoL, health related quality of life; EQ–5D, Euro quality of life–5 dimension;
EQ–VAS, Euro quality of life–visual analogue scale.
*P–values represent differences between age group in each gender (P<0.05). P–
value were obtained by analysis of variance.
오정민 외. 한국 성인의 근감소증과 건강 관련 삶의 질과의 연관성 Korean Journal of Family Practice
KJFP
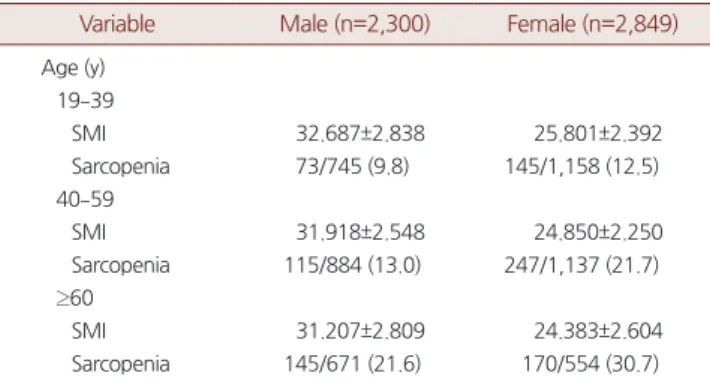
2. 연령 증가에 따른 평균 SMI와 근감소증 유병률
Table 2는 남, 여 각각에서 연령 그룹별 skeletal muscle index (SMI) 평균값과 표준편차와 근감소증 유병률을 나타낸 결과로, 남, 여 모 두에서 연령이 증가함에 따라 SMI 평균값은 유의하게 감소하였고, 근감소증 유병률은 유의하게 증가하였다(P<0.05).
3. 연령 증가에 따른 근감소증과 건강 관련 삶의 질 지표와의 연관성
Table 3은 남, 여 각각의 정상 그룹과 근감소증 그룹에서의 연령별 EQ-5D index와 EQ-VAS의 t-test 결과로 평균과 표준편차를 나타냈다.
남성의 경우 정상 그룹에서는 연령이 높아질수록 EQ-5D index와 EQ-VAS 값이 감소하였고, 통계적으로도 유의하였다. 근감소증 그룹 에서는 연령이 증가함에 따라 EQ-5D index가 유의하게 감소하였으 나, EQ-VAS는 통계적 유의성이 없었다.
여성의 경우, 정상인 그룹에서는 연령이 높아질수록 EQ-5D index 와 EQ-VAS가 감소하였고 통계적으로 유의하였으며, 근감소증 그룹
에서도 연령이 증가함에 따라 EQ-5D index와 EQ-VAS가 감소하였고, 통계적으로도 유의하였다.
결론적으로 남성, 여성 모두에서 근감소증 그룹에서 정상그룹에 비해 건강 관련 삶의 질 지표가 낮았고, 연령이 증가함에 따라 건강 관련 삶의 질 만족도가 낮게 나타났다(P<0.05).
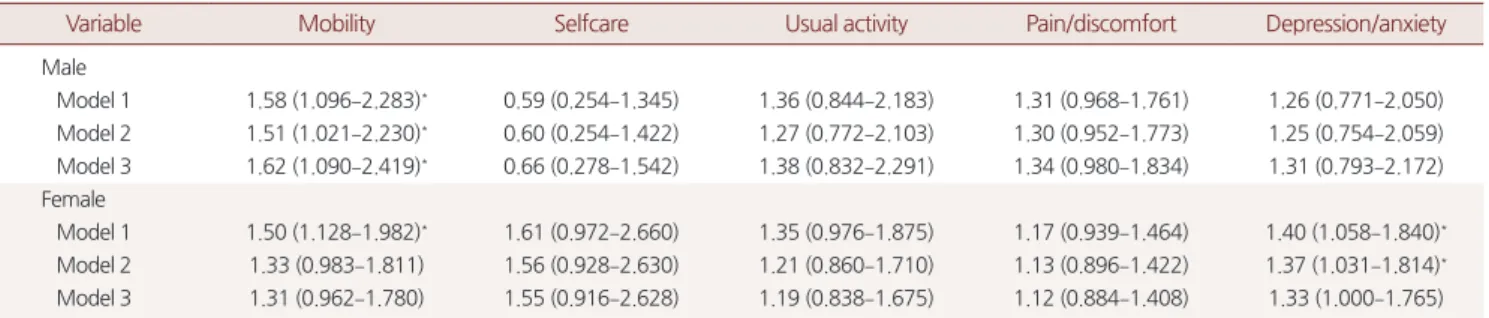
4. 근감소증과 EQ-5D와의 관계
Table 4는 성별에 따른 근감소증과 EQ-5D의 연관성에 관한 로지 스틱 회귀분석 결과이다.
남자의 경우 근감소증이 있는 사람이 정상인과 비교했을 때 운동 능력의 문제 발생 위험이 1.62배 증가하였다(odds ratio [OR], 1.62; 95%
confidence interval [CI], 1.090–2.419). 여성에서는 model 1에서만 근감 소증 그룹에서 정상 그룹에 비해 운동능력 문제 발생 위험이 1.50배 증가하였고(OR, 1.50; 95% CI, 1.128–1.982), model 1, 2에서 근감소증 그룹에서 불안/우울의 문제 발생 위험이 각각 1.40배(OR, 1.40; 95%
CI, 1.058–1.840), 1.37배(OR, 1.37; 95% CI, 1.031–1.814) 증가하였다.
Table 4. Adjusted odds ratio for individual components of EQ-5D descriptive system in subjects with sarcopenia compared to subjects without sar- copenia
Variable Mobility Selfcare Usual activity Pain/discomfort Depression/anxiety
Male
Model 1 1.58 (1.096–2.283)* 0.59 (0.254–1.345) 1.36 (0.844–2.183) 1.31 (0.968–1.761) 1.26 (0.771–2.050) Model 2 1.51 (1.021–2.230)* 0.60 (0.254–1.422) 1.27 (0.772–2.103) 1.30 (0.952–1.773) 1.25 (0.754–2.059) Model 3 1.62 (1.090–2.419)* 0.66 (0.278–1.542) 1.38 (0.832–2.291) 1.34 (0.980–1.834) 1.31 (0.793–2.172) Female
Model 1 1.50 (1.128–1.982)* 1.61 (0.972–2.660) 1.35 (0.976–1.875) 1.17 (0.939–1.464) 1.40 (1.058–1.840)* Model 2 1.33 (0.983–1.811) 1.56 (0.928–2.630) 1.21 (0.860–1.710) 1.13 (0.896–1.422) 1.37 (1.031–1.814)* Model 3 1.31 (0.962–1.780) 1.55 (0.916–2.628) 1.19 (0.838–1.675) 1.12 (0.884–1.408) 1.33 (1.000–1.765) Values are presented as odds ratio (95% confidence interval) by using logistic regression analysis. Model 1 was adjusted for age, body mass index, L–spine bone mineral density. Model 2 was adjusted for hypertension, dyslipidemia, arthritis, thyroid disease, asthma, pulmonary tuberculosis, atopic dermatitis in addition to the factors of model 1. Model 3 was adjusted for smoking, alcohol, regular exercise, education in addition to the factors of model 2.
EQ–5D, Euro quality of life–5 dimension.
*P–value<0.05.
Table 5. Adjusted risk of impaired components of EQ-5D according to age in sarcopenia
Age Mobility Selfcare Usual activity Pain/discomfort Depression/anxiety
Male (y)
19–39 7.49 (1.989–28.181)* 2.01 (0.176–23.015) 2.50 (0.242–25.785) 2.26 (1.153–4.413)* 3.63 (1.287–10.248)* 40–59 2.62 (1.286–5.349)* 2.33 (0.382–14.225) 1.94 (0.630–5.982) 1.65 (0.973–2.814) 0.41 (0.119–1.429) ≥60 1.16 (0.710–1.908) 0.35 (0.117–1.039) 1.30 (0.733–2.300) 0.95 (0.596–1.502) 1.40 (0.705–2.798) Female (y)
19–39 3.68 (1.237–10.932)* N/A 0.69 (0.078–6.165) 1.55 (0.962–2.485) 1.10 (0.587–2.043)
40–59 1.36 (0.842–2.211) 1.34 (0.401–4.449) 1.16 (0.647–2.071) 0.90 (0.631–1.296) 1.68 (1.102–2.559)* ≥60 1.21 (0.791–1.839) 1.65 (0.909–3.009) 1.39 (0.881–2.178) 1.27 (0.851–1.894) 1.17 (0.700–1.961) Values are presented as odds ratio (95% confidence interval). Odds ratios and 95% confidence intervals were obtained by logistic regression analysis. Adjusted by age, body mass index, L–spine bone mineral density, dyslipidemia, arthritis, thyroid disease, asthma, pulmonary tuberculosis, atopic dermatitis, smoking, alcohol, regular ex- ercise and education.
EQ–5D, Euro quality of life–5 dimension; N/A, not available value.
*P–value<0.05.
Jeong Min Oh, et al. Association between Sarcopenia and HRQoL in Korean Adults
Korean Journal of Family Practice
KJFP
5. 연령 그룹 별 근감소증과 EQ-5D와의 연관성
Table 5는 연령그룹별 근감소증에 따른 EQ-5D 발생과의 연관성을 보기 위한 로지스틱 회귀분석 결과이다.
남성에서는 20–30대 그룹에서 근감소증일 때 ‘운동능력’, ‘통증/불 편’, ‘불안/우울’의 문제 발생 위험도가 각각 OR, 7.49 (95% CI, 1.989- 28.181), 2.26 (95% CI, 1.153–4.413), 3.63 (95% CI, 1.287–10.248)로 유의하 게 높았으며, 40–50대 그룹에서는 근감소증일 때 ‘운동능력’ 문제 발 생 위험도가 OR, 2.62 (95% CI, 1.286–5.349)로 유의하게 높았고, 60대 이상에서는 근감소증과 EQ-5D의 통계적으로 유의한 연관성은 없 었다(P<0.05).
여성에서는 20-30대 그룹에서 근감소증일 때 ‘운동능력’의 문제 발 생 OR, 3.68 (95% CI, 1.237–10.932), 40–50대 그룹에서 근감소증일 때
‘불안/우울’의 문제 발생 OR, 1.68 (95% CI, 1.102–2.559)로 유의하게 높 았으며, 60대 이상에서는 근감소증과 EQ-5D는 통계적으로 유의한 연관성은 없었다(P<0.05).
고 찰
근감소증은 1988년에 Rosenberg14)에 의해 처음 도입된 개념으로, 최초 Baumgartner 등15)이 신장으로 보정한 근감소증 진단 기준을 제 시한 이후 다양한 연구가 이루어지고 있는데 현재 근감소증 유병률 은 진단 기준과 성별에 따라 매우 다른 결과를 나타낸다. 가장 많이 사용되는 Baumgartner 등15)이 제시한 진단 기준은 절대적인 근육량 을 비교한 것으로, 체지방이 많은 사람이 근육량도 많다는 것을 반 영하지 못해 체지방량이 많을수록 근감소증으로 분류될 가능성이 낮아진다는 단점이 있다.15,16) 따라서 남성보다 상대적으로 체지방량 이 더 많은 여성에게 적용하기에 제한이 있어 이런 단점을 극복한 Janssen17)의 진단법을 이용한 Kim 등9)에 의해 제시된 체중으로 보정 한 진단 기준을 사용하였다.
최근에는 근감소증의 진단 기준으로 신장과 체중 두 가지 모두를 반영하는 body mass index로 보정하는 진단 기준18)에 대한 연구가 이 루어지고 있으며, 이 진단 기준에 따른 근감소증은 어느 한 가지로 보정했을 때보다 신체 기능의 감소와 더 큰 상관관계를 보였다는 연 구결과가 있었다. 한국인을 대상으로 한 연구18,19)도 있으나 남성, 여 성 모두를 포함한 연구와 대표성을 띤 절단점을 제시한 연구는 없어 앞으로도 지속적인 연구가 필요할 것으로 보인다.
이전 Go 등20)의 신장으로 보정한 진단 기준을 적용한 한국 남성에 서 골밀도와 근감소증과 건강 관련 삶의 질의 연관성을 본 연구에서 는 근감소증이 동반될수록 ‘운동능력’, ‘자가관리’, ‘일상활동’, ‘불안/
우울’ 항목에서 문제가 발생할 위험도가 더 높다는 결과를 밝혔는
데, 체중 보정 진단 기준을 사용한 본 연구에서는 남자에서 근감소 증이 동반될수록 ‘운동능력’ 문제 발생 위험도만 높게 나타났다. 여 러 진단 기준을 비교한 Kim 등19)의 연구에 따르면 신장 보정 진단 기 준은 신체적 장애 혹은 신체적 허약과 연관성이 크며,15,21) 체중 보정 진단 기준은 기능적 손상과 장애와 더 큰 연관성9,17,22)이 있다고 밝히 고 있어 이러한 연구결과의 차이는 적용한 진단 기준의 차이에서 발 생한 것으로 판단된다.
본 연구에서는 남성과 여성에서 근감소증이 건강 관련 삶의 질에 미치는 영향에 차이가 있었는데, 남성의 경우 신체적 기능 측면(운 동능력)에 영향을 미쳤지만, 여성의 경우 신체적 기능(운동능력)뿐 아니라 정신 건강(불안/우울) 측면에도 영향을 미쳤다. 특히, ‘불안/우 울’ 영역은 model 3에서 유의하지 않게 나온 것으로 미루어 여성에서 의 불안/우울감은 근감소증보다 다른 생활요인들(흡연, 음주, 규칙 적 운동, 교육수준)이 더 큰 영향을 미치는 것으로 판단된다(P<0.05).
또한, 연령대별로 근감소증과 EQ-5D의 관계가 다르게 나타났는 데, 20–30대 남성에서 근감소증이 동반되어 있을 때 정상인에 비해
‘운동능력’, ‘통증/불편’, ‘불안/우울’ 문제 발생 위험도가 높았고, 여성 에서는 ‘운동능력’ 문제 발생 위험도가 높았는데, 가장 활발하게 사 회생활을 해야 하는 청장년층의 근감소증은 신체적 영역뿐 아니라 정신 건강 영역까지 영향을 미치는 것으로 나타났다.
국민건강영양조사 자료의 한계로 인해 20–30대의 근감소증이 어 떠한 원인에 의해 발생했는지를 파악할 수는 없었으나, 근감소증은 노년층뿐 아니라 젊은 성인에게도 건강 관련 삶의 질에 영향을 미칠 수 있다는 점을 고려하여 청장년 시기부터 장기적인 의료적 개입이 필요할지에 대해서는 더 연구가 필요할 것으로 생각된다.
또한, 고령일수록 근감소증과 HRQoL의 관계가 밀접할 것이라고 예상했던 것과는 달리 남녀 모두 60세 이상 군에서 근감소증과 HRQoL 사이에 통계적 유의성이 없었다. 그 원인으로는 근감소증 단 일 요인보다는 노화에 따라 동반되는 만성 질환들(model 2-chronic disease)과 개개인의 통증관리 능력(model 3-lifestyle 및 socioeconomic factor)이 HRQoL에 더 큰 영향을 미치기 때문으로 판단된다.
이번 연구에는 몇 가지 제한점을 가지고 있다.
첫째, 이번 연구는 단면 연구이기 때문에 근감소증과 건강 관련 삶의 질의 시간적 선후관계를 알 수 없어 인과관계를 밝히기 어려우 며, 청장년층의 근감소증이 노년기에 영향을 미치는지에 대한 선후 관계를 알기 어렵다.
둘째, 근감소증을 진단하는 기준이 표준화되어 있지 않아 각 진단 방법에 따른 연구의 결과를 직접적으로 비교하기엔 한계가 있었으 며, 연구에 적용하는 진단 기준에 따라 결과가 달라질 수 있다는 한 계가 있다.
오정민 외. 한국 성인의 근감소증과 건강 관련 삶의 질과의 연관성 Korean Journal of Family Practice
KJFP
셋째, 국민건강영양조사 자료의 부족으로 이차성 근감소증의 원 인과 신체적 기능에 영향을 줄 수 있는 유년기와 학동기 시절의 건 강상태와 신체활동, 골절 사고 등에 대한 정보를 확인할 수 없었다.
그럼에도 불구하고 본 연구는 다음과 같은 장점이 있다.
첫째, 우리나라 인구 전체의 대표성을 가진 국민건강영양조사 자 료를 이용하여 혼란변수를 보정한 후 근감소증과 건강 관련 삶의 질 의 연관성을 분석하였다는 점이다.
둘째, 근감소증과 관련된 위험인자의 자료를 모아 model 1에서 model 3까지 보정을 하여 분석을 하였고, 나아가 연령집단별로 근감 소증이 건강 관련 삶의 질에 미치는 영향까지 분석했다는 점이다.
결론적으로, 이 연구는 대한민국 만19세 이상의 성인에서 근감소 증은 건강 관련 삶의 질에 영향을 미치며, 남성의 경우 신체 기능 장 애를 유발하고, 여성의 경우 신체 기능적 측면뿐 아니라 정신 건강 측면까지도 영향을 미친다는 것을 확인하였다.
이번 연구결과를 토대로 근감소증과 건강 관련 삶의 질의 인과관 계를 밝히는 것뿐 아니라 더 나아가 청장년층의 이차성 근감소증이 노년기 근감소증과 건강 관련 삶의 질에 미치는 영향에 대한 전향적 연구가 필요할 것으로 판단된다.
요 약
연구배경:
본 연구는 우리나라 성인 인구를 대상으로 근감소증과 건강 관련 삶의 질의 관계에 대한 연구를 시행하였다.방법:
제5기 국민건강영양조사에 참여한 만19세 이상 성인 남녀를 대상으로 DEXA로 측정한 양 사지근육량의 합을 체중으로 보정한 값으로 근감소증을 정의하였고, 절단점은 남 29.1%, 여 23.0%로 근감 소증을 진단하였다. 건강 관련 삶의 질 평가는 EQ-5D를 사용했으며, 현재의 건강상태를 묻는 EQ-5D, EQ-VAS, 그리고 우리나라 평가 기 준을 적용한 EQ-5D index를 평가하였다. 근감소증에 따른 건강 관 련 삶의 질의 연관성을 파악하기 위해 chi-square, analysis of variance, t-test, logistic regression analysis를 이용하였다.결과:
남성과 여성 각각 근감소증 유병률은 14.5%, 19.7%였으며, 남녀 모두에서 연령이 증가함에 따라 근감소증 유병률은 유의하게 증가 하였고, EQ-5D index는 감소하였다. 근감소증과 EQ-5D의 로지스틱 회귀분석에서 남성은 근감소증 그룹에서 ‘운동능력’ OR, 1.62 (95%CI, 1.090–2.419)였고, 여성에서는 ‘운동능력’ OR, 1.31 (95% CI, 0.962–
1.780), ‘불안/우울’ OR, 1.33 (95% CI, 1.111–1.765)였으나, 통계적 유의성 은 없었다. 남성의 경우, 20-30대 그룹에서 근감소증일 때 ‘운동능력’,
‘통증/불편’, ‘불안/우울’ OR가 각각 7.49, 2.26, 3.63였고, 40–50대 그룹 에서는 근감소증일 때 ‘운동능력’ OR는 2.62였다. 여성의 경우 20–30
대 그룹에서 근감소증일 때 ‘운동능력’ OR는 3.68, 40–50대 그룹에서 는 ‘불안/우울’ OR는 1.68였다.
결론:
본 연구를 통해 우리나라 만19세 이상의 성인 남녀에서 근감 소증은 건강 관련 삶의 질과 관계있으며, 남성에서는 신체적 기능 장 애, 여성에서는 신체적 기능 장애와 정신적 측면에 영향을 미친다는 것을 확인하였다.중심단어:
근감소증; EuroQoL-5 Dimension; 건강 관련 삶의 질REFERENCES
1. Hong S, Choi WH. Clinical and physiopathological mechanism of sarcope- nia. Korean J Med 2012; 83: 444-54.
2. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al.
Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in older people. Age Ageing 2010;
39: 412-23.
3. Morley JE. Diabetes, sarcopenia, and frailty. Clin Geriatr Med 2008; 24: 455- 69, vi.
4. Kim TN, Park MS, Yang SJ, Yoo HJ, Kang HJ, Song W, et al. Prevalence and determinant factors of sarcopenia in patients with type 2 diabetes: the Kore- an Sarcopenic Obesity Study (KSOS). Diabetes Care 2010; 33: 1497-9.
5. Testa MA, Simonson DC. Assessment of quality-of-life outcomes. N Engl J Med 1996; 334: 835-40.
6. Otero-Rodríguez A, León-Muñoz LM, Balboa-Castillo T, Banegas JR, Ro- dríguez-Artalejo F, Guallar-Castillón P. Change in health-related quality of life as a predictor of mortality in the older adults. Qual Life Res 2010; 19: 15- 23.
7. Rodríguez-Artalejo F, Guallar-Castillón P, Pascual CR, Otero CM, Montes AO, García AN, et al. Health-related quality of life as a predictor of hospital readmission and death among patients with heart failure. Arch Intern Med 2005; 165: 1274-9.
8. Lee SK, Lee JA, Kim JY, Kim YZ, Park HS. The risk factors of sarcopenia among Korean elderly men: based on 2009 Korean national health and nu- tritional examination survey data. Korean J Obes 2014; 23: 23-31.
9. Kim YS, Lee Y, Chung YS, Lee DJ, Joo NS, Hong D, et al. Prevalence of sarco- penia and sarcopenic obesity in the Korean population based on the Fourth Korean National Health and Nutritional Examination Surveys. J Gerontol A Biol Sci Med Sci 2012; 67: 1107-13.
10. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med 2001; 33: 337-43.
11. Korean Centers for Disease Control and Prevention. The report of quality weighted health related quality of life. Seoul: Korean Centers for Disease Control and Prevention; 2007.
12. Lee YH, Choi JS, Rhee JA, Ryu SY, Shin MH, Kim JH. A study on the appli- cation of the Korean valuation weights for EuroQoL-5 dimension. Korean J Health Educ Promot 2009; 26: 1-13.
13. Kim JS, Oh MK, Park BK, Lee MK, Kim GJ. Screening criteria of alcoholism
Jeong Min Oh, et al. Association between Sarcopenia and HRQoL in Korean Adults
Korean Journal of Family Practice
KJFP
by alcohol use disorders identification test (AUDIT) in Korea. J Korean Acad Fam Med 1999; 20: 1152-9.
14. Rosenberg IH. Sarcopenia: origins and clinical relevance. J Nutr 1997; 127(5 Suppl): 990S-991S.
15. Baumgartner RN, Koehler KM, Gallagher D, Romero L, Heymsfield SB, Ross RR, et al. Epidemiology of sarcopenia among the elderly in New Mexi- co. Am J Epidemiol 1998; 147: 755-63.
16. Kwon HJ, Ha YC, Park HM. Prevalence of sarcopenia in the Korean woman based on the Korean National Health and Nutritional Examination Surveys.
J Bone Metab 2016; 23: 23-6.
17. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarco- penia) in older persons is associated with functional impairment and physi- cal disability. J Am Geriatr Soc 2002; 50: 889-96.
18. Meng NH, Li CI, Liu CS, Lin WY, Lin CH, Chang CK, et al. Sarcopenia de- fined by combining height- and weight-adjusted skeletal muscle indices is closely associated with poor physical performance. J Aging Phys Act 2015;
23: 597-606.
19. Kim KM, Jang HC, Lim S. Differences among skeletal muscle mass indices derived from height-, weight-, and body mass index-adjusted models in as- sessing sarcopenia. Korean J Intern Med 2016; 31: 643-50.
20. Go SW, Cha YH, Lee JA, Park HS. Association between sarcopenia, bone density, and health-related quality of life in Korean men. Korean J Fam Med 2013; 34: 281-8.
21. Liu LK, Lee WJ, Liu CL, Chen LY, Lin MH, Peng LN, et al. Age-related skele- tal muscle mass loss and physical performance in Taiwan: implications to diagnostic strategy of sarcopenia in Asia. Geriatr Gerontol Int 2013; 13: 964- 71.
22. Delmonico MJ, Harris TB, Lee JS, Visser M, Nevitt M, Kritchevsky SB, et al.
Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. J Am Geriatr Soc 2007; 55: 769-74.