ISSN 0378-6471 (Print)⋅ISSN 2092-9374 (Online)
http://dx.doi.org/10.3341/jkos.2016.57.1.63
Original Article
망막정맥폐쇄에서 유리체강내 베바시주맙 주사 후 신경절세포층의 두께 변화
Ganglion Cell Layer Thickness after Anti‐Vascular Endothelial Growth Factor Treatment in Retinal Vein Occlusion
이지영⋅김형찬
Ji Young Lee, MD, Hyung Chan Kim, MD, PhD
건국대학교 의과대학 건국대학교병원 안과학교실
Department of Ophthalmology, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea
Purpose: To evaluate the effect of repeated intravitreal injections of anti-vascular endothelial growth factor (anti-VEGF) on the thickness of the ganglion cell layer (GCL) in patients with retinal vein occlusion.
Methods: The present retrospective study included 60 patients with branch retinal vein occlusion and central retinal vein occlu- sion who received more than 3 anti-VEGF injections. GCL thickness was measured using spectral-domain optical coherence tomography. GCL thickness measurements were made at 9 Early Treatment Diabetic Retinopathy Study grid regions. We eval- uated correlations between changes in the GCL thickness and other factors such as intraocular pressure, times of injection, and changes in central macular thickness (CMT).
Results: As a result of multiple intravitreal anti-VEGF treatments, GCL thickness was significantly decreased from 42.99 ± 5.39 to 38.99 ± 5.53 (p < 0.001). Changes in GCL thickness were correlated with CMT and the number of injections (p = 0.02 and p
= 0.048, respectively). However, multivariate analysis showed the change in mean GCL thickness in the retinal vein occlusion (RVO) was strongly associated only with CMT (p < 0.001).
Conclusions: As a result of multiple intravitreal injections of anti-VEGF, GCL thickness decreased significantly in RVO patients and changes in GCL thickness and CMT were correlated.
J Korean Ophthalmol Soc 2016;57(1):63-70
Key Words: Autosegmentation, Ganglion cell layer, Intravitreal anti-vascular endothelial growth factor injection, Retinal vein occlusion, Spectral domain optical coherence tomography
■Received: 2015. 5. 15. ■ Revised: 2015. 9. 23.
■Accepted: 2015. 11. 20.
■Address reprint requests to Hyung Chan Kim, MD, PhD Department of Ophthalmology, Konkuk University Medical Center, #120-1 Neungdong-ro, Gwangjin-gu, Seoul 05030, Korea
Tel: 82-2-2030-8180, Fax: 82-2-2030-5273 E-mail: [email protected]
ⓒ2016 The Korean Ophthalmological Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
망막정맥폐쇄는 시력상실을 유발하는 망막혈관질환 중 당뇨망막병증 다음으로 흔한 질환이다.1,2 망막정맥폐쇄는
혈관 폐쇄부위에 따라 망막분지정맥폐쇄, 망막중심정맥폐 쇄, 앞쪽 시신경 부위 중심정맥의 한 가지를 침범한 절반 망막정맥폐쇄로 분류할 수 있다.3 망막정맥폐쇄 환자에서 시력저하를 일으키는 가장 흔한 원인은 황반부종으로, 이 는 혈액망막장벽의 파괴, 혈관내피성장인자나 인터루킨-6 등의 혈관투과성을 변화시키는 인자들에 의해 혈관 내에 서 주변조직으로 액체의 이동이 유발되어 발생한다고 알 려져 있다.4-6
황반부종을 동반한 망막분지정맥폐쇄 환자에서 유리체 강내 혈관내피성장인자의 농도가 증가하여 있고 이것이 황
반 부종의 정도 및 망막모세혈관 비관류 면적과 상관관계 가 있음이 알려져 있다. 많은 연구에서 황반부종을 동반한 망막정맥폐쇄 환자에서 유리체강내 베바시주맙주사를 통 해 시력의 호전이 있음을 보고하였고,7-11 망막정맥폐쇄 환 자에서 유리체내 베바시주맙 주입술의 2년 임상결과를 보 고한 연구에서도 시력의 유의한 호전이 유지되었음을 확인 하였다.12 여러 연구에서 혈관내피성장인자의 신경보호작 용 및 망막을 포함한 신경조직의 발달과 성숙을 촉진하는 작용을 가지고 있음을 보고하였고,13,14 항혈관내피성장인자 주입술로 인해 망막 신경절세포의 사멸이 진행됨을 보고한 연구도 있었다.15
녹내장은 망막신경절세포의 손실 및 망막신경섬유층의 두께 감소가 나타나는 질병으로16,17 시신경유두 주위 망막 신경섬유층의 두께 측정으로 초기 녹내장의 구조변화를 측 정할 수 있다.18-20 Tan et al21은 녹내장에서 시야변화보다 망막신경섬유층과 신경절세포층 및 내망상층의 두께 변화 가 먼저 나타남을 보고하였다.
스펙트럼영역 빛간섭단층촬영은 망막신경절세포를 포함 한 망막의 전층을 자동측정할 수 있는 장비로 Takagishi et al22은 스펙트럼영역 빛간섭단층촬영을 이용한 신경절복합 체 두께 측정이 시간영역 빛간섭단층촬영을 이용한 황반의 망막두께 측정보다 더 정확함을 발표하였다.
몇몇의 연구들에서 항혈관내피세포성장인자 주입술의 장기적인 안정성에 대한 연구를 진행하였고, Park et al23 은 반복적인 유리체강내 항혈관내피성장인자 주입술이 의미 있는 망막신경섬유층의 두께 변화를 일으키지는 않 는다고 보고하였다. 한편 Martinez-de-la-Casa et al24은 습 성 황반변성 환자에서 항혈관내피성장인자를 반복적으로 유리체내 주입하였을 때 직접적인 약물독성 및 안압의 변 화로 인해 망막신경섬유층의 두께를 변화시킴을 보고하 였다.
항혈관내피성장인자의 안정성에 대한 많은 보고들이 있 었지만 망막혈관폐쇄 환자에서 반복적인 유리체내 항혈관 내피성장인자 주입술이 망막 신경절세포에 미치는 영향에 대한 보고는 없었다. 이에 본 연구는 3회 이상의 베바시주 맙주입술을 받은 망막혈관폐쇄에서 치료 전후 망막신경절 세포층의 두께 변화를 스펙트럼영역 빛간섭단층촬영을 이 용하여 비교하고자 하였다
대상과 방법
2010년 1월부터 2013년 9월까지 망막정맥폐쇄에 동반된 망막부종으로 유리체강내 베바시주맙(Avastin®, Genetech Inc., San Francisco, CA, USA) 주입술을 3회 이상 시행 받
은 환자를 대상으로 후향적 의무기록 분석을 시행하였다. 망막분지정맥폐쇄 35안, 망막중심정맥폐쇄 25안을 대상으 로 하였고 심한 망막부종이나 백내장 등의 매체혼탁으로 인 해 spectral domain optical coherence tomography (SD-OCT) 로 망막의 구조를 확인하기 어려운 환자들을 제외하였다. 그 외에도 백내장 수술을 제외한 유리체절제술, 녹내장 수 술 등 다른 안과적인 수술의 과거력이 있는 경우, 다른 망 막질환을 가지고 있는 경우, 시력이나 망막상태에 영향을 줄 수 있는 다른 질병을 가지고 있는 경우는 대상에서 제외 하였다. 모든 환자는 시술을 받기 전 최대교정시력과 안압 을 측정하였고 세극등현미경검사, 안저검사, 형광안저혈관 촬영, 빛간섭단층촬영을 시행하였다.
유리체강내 베바시주맙 주입술은 수술실에서 시행되었 다. 시술 방법은 점안 마취 후 5% providone iodine으로 눈 주위 및 안구를 소독하고 각막 윤부로부터 수정체 안에서 는 3.5 mm, 인공수정체 안에서는 3.0 mm 떨어진 하이측 부위에 30 G 주사 바늘을 이용하여 유리체강내로 베바시주 맙(Avastin®, 1.25 mg/0.05 mL)을 주입하였다. 유리체강내 주입술 후 moxifloxacin hydrochloride 0.5% (Vigamox, Alcon Laboratories, Fort Worth, TX, USA)를 1주간 점안하 게 하였다.
유리체강내주입술 후 4-6주 간격으로 최대교정시력과 빛 간섭단층촬영을 시행하였으며 경과관찰 기간 중 황반 부종 이 지속되거나 재발하는 경우에는 4-6주 간격으로 추가 유 리체강내 베바시주맙 주입술을 시행하였다.
SD-OCT measurement
신경절세포층 및 망막두께는 스펙트럼영역 빛간섭단층촬 영(SD-OCT; Spectralis, Heidelberg Engineering, Heidelberg, Germany)을 이용해서 측정하였다. Spectralis OCT는 레이저 검안경검사를 동시에 시행할 수 있는 고해상도 스펙트럼영 역 빛간섭단층촬영으로 광원으로는 50 nm의 bandwidth와 840 nm의 파장을 가진 다이오드 레이저를 사용한다. 황반부 를 중심으로 7 μm의 축 해상도로 초당 40,000개의 A-scan을 조사한다. Raster scan 방식으로 황반을 중심으로 수평, 수 직이 각각 768 pixel (8.7 mm) × 496 pixel (1.9 mm)로 이 루어진 25개의 B-scan 방식으로 황반부 8.8 × 5.9 mm에 해 당하는 부위의 cross-sectional image를 얻었다. Eye track- ing을 하는 automatic real-time (ART) 기능을 사용하여 눈 움직임에 의한 오류를 보정하였다.
신경절세포층은 망막신경섬유층의 외측경계에서 내망상 층의 내측경계까지의 영역을 측정하였고, 이는 자동적으로 망막의 10개층을 구분지어 주는 Spectralis software version 6.0을 통해 얻었으며, 심각한 망막내액 등으로 인해 정확한
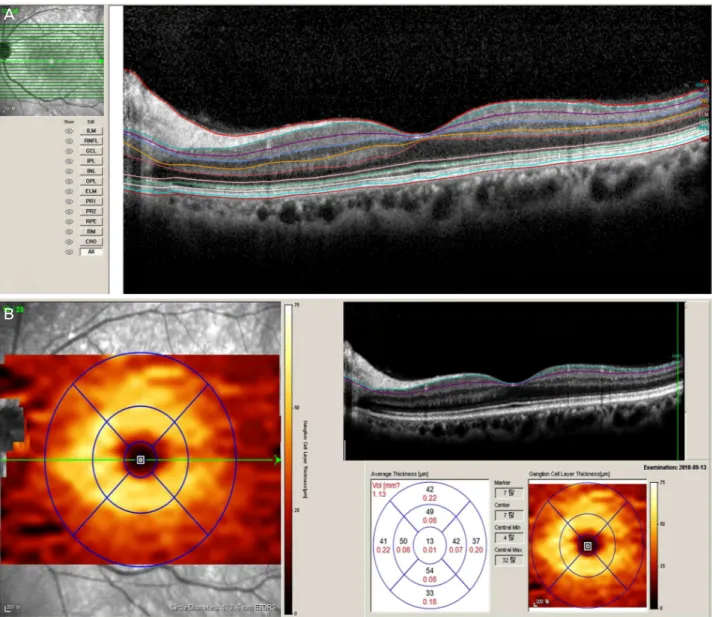
Figure 1. Automatic segmentation of retina by SD-OCT. (A) Segmentation editor view of retina by SD-OCT Spectralis software ver-
sion 0.6. A segmentation line marks and belongs to either a certain retinal structure (ILM, ELM, PR1, PR2, RPE, BM) or the outer boundary of a retinal or sub-retinal layer (RNFL, GCL, IPL, INL, OPL, ONL, CHO). (B) Thickness map of GCL, RNFL, and IPL.ILM = internal limiting membrane; RNFL = retinal nerve fiber layer; GCL = ganglion cell layer; IPL = inner plexiform layer; INL
= inner nuclear layer; OPL = outer plexiform layer; ELM = external limiting membrane; PR1 = first photoreceptor layer; PR2 = second photoreceptor layer; RPE = retinal pigment epithelium; BM = Bruch's membrane; CHO = choroid; ETDRS = Early Treatment Diabetic Retinopathy Study; SD-OCT = spectral domain optical coherence tomography; ONL = outer nuclear layer.
층의 경계가 구분되지 않은 경우에 한해서 경계를 보정해 주었다. SD-OCT 영상에서 fovea를 중심으로 1, 3, 6 mm 떨어진 원으로 구획을 나누었고 망막 신경절세포층의 두께 는 fovea를 중심으로 반지름 1 mm의 원 부위를 ganglion cell layer (GCL) fovea, fovea를 중심으로 반지름 3 mm의 원까지의 부위를 4곳으로 나누어서 각각 sperior-central (SC), nasal-central (NC), inferior-central (IC), temporal-cen- tral (TC), fovea를 중심으로 반지름 6 mm의 원까지를 4곳 으로 나누어 superior-peripheral (SP), nasal-peripheral (NP), inferior-peripheral (IP), temporal-peripheral (TP)로 정하여
각 부위의 평균 두께를 측정한 값으로 구하였다(Fig. 1).
Statistical analyses
통계는 SPSS 프로그램(ver. 18.0; SPSS Inc., Chicago, IL, USA)을 이용하였다. 단변량분석은 paired t-test, Wilcoxon signed-rank test, Chi-square test로 검정하였고, 인자들 사이의 연관관계에 대한 분석은 Pearson correlation analysis를 이용하였다. 0.05 미만의 p값을 통계적으로 유의 하다고 평가하였다.
A
B
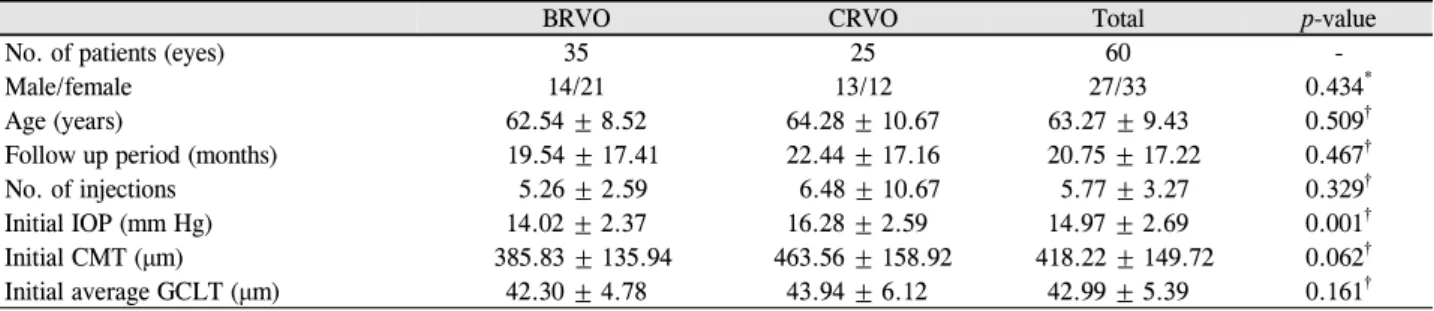
Table 1. Baseline characteristics of patients
BRVO CRVO Total p-value
No. of patients (eyes) 35 25 60 -
Male/female 14/21 13/12 27/33 0.434*
Age (years) 62.54 ± 8.52 64.28 ± 10.67 63.27 ± 9.43 0.509†
Follow up period (months) 19.54 ± 17.41 22.44 ± 17.16 20.75 ± 17.22 0.467†
No. of injections 5.26 ± 2.59 6.48 ± 10.67 5.77 ± 3.27 0.329†
Initial IOP (mm Hg) 14.02 ± 2.37 16.28 ± 2.59 14.97 ± 2.69 0.001†
Initial CMT (μm) 385.83 ± 135.94 463.56 ± 158.92 418.22 ± 149.72 0.062†
Initial average GCLT (μm) 42.30 ± 4.78 43.94 ± 6.12 42.99 ± 5.39 0.161†
Values are presented as mean ± SD unless otherwise indicated.
BRVO = branch retinal vein occlusion; CRVO = central retinal vein occlusion; IOP = intraocular pressure; CMT = central macular thick- ness; GCLT = ganglion cell layer thickness.
*Chi-square test; †Mann-Whitney test.
Table 2. Changes in GCL and CMT before and after treatment
Total (BRVO + CRVO)
Pre-treatment Post-treatment p-value*
GCLT
Fovea (μm) 22.20 ± 10.02 18.25 ± 8.25 0.038
SC (μm) 54.47 ± 7.93 50.02 ± 9.97 <0.001
SP (μm) 37.37 ± 5.95 34.42 ± 7.57 0.003
NC (μm) 54.97 ± 7.46 50.97 ± 8.18 <0.001
NP (μm) 41.55 ± 5.48 40.43 ± 5.80 0.099
IC (μm) 54.15 ± 11.34 47.98 ± 13.24 <0.001
IP (μm) 35.60 ± 6.46 33.20 ± 6.72 0.003
TC (μm) 49.85 ± 8.38 41.87 ± 8.59 <0.001
TP (μm) 38.05 ± 6.72 33.78 ± 7.08 <0.001
Average 42.99 ± 5.39 38.99 ± 5.53 <0.001
CMT (μm) 418.22 ± 149.72 306.93 ± 89.02 <0.001
Values are presented as mean ± SD unless otherwise indicated.
GCL = ganglion cell layer; CMT = central macular thickness; BRVO = branch retinal vein occlusion; CRVO = central retinal vein occlu- sion; GCLT = ganglion cell layer thickness; SC = superior-central; SP = superior-peripheral; NC = nasal-central; NP = nasal-peripheral;
IC = inferior-central; IP = inferior-peripheral; TC = temporal-central; TP = temporal-peripheral.
*Paired t-test.
Table 3. Correlation of changes in GCLT with other variables
Variables r p-value*
Age (years) 0.129 0.326
Changes in IOP 0.082 0.535
Changes in CMT 0.392 0.002
No. of injections 0.256 0.048
GCLT = ganglion cell layer thickness; IOP = intra ocular pres- sure; CMT = central macular thickness.
*Spearman correlation test.
결 과
대상 환자는 총 60명 66안이었으며 이 중 남자가 27안, 여자가 33안, 평균 연령은 62.5세였다. 평균 주사횟수는 5.8
± 3.3회였고, 평균 경과관찰 기간은 20.7 ± 17.2개월이었다.
치료 전 환자정보는 Table 1에 나타내었다. 전체 환자 중 망막분지정맥폐쇄가 35명, 망막중심정맥폐쇄가 25명이었 고 치료 전 시력 및 중심망막두께, 망막 신경절세포층 두께 등은 두 군 간 유의한 차이가 없었으며, 안압만이 중심정맥 폐쇄에서 유의하게 높게 측정되었다
망막 신경절세포층의 두께 변화는 전체 환자에서 GCL NP 부위를 제외한 모든 영역에서 치료 전에 비해 치료 후 유의한 감소를 보였고, 신경절세포층의 평균 두께도 유의 한 감소를 나타냈다(Table 2). 하위그룹 분석에서 평균 신 경절세포층 두께가 망막분지정맥폐쇄에서는 치료 전 42.30
± 4.78 µm에서 치료 후 38.71 ± 4.45 µm로 유의하게 감소
하였고(p<0.001, Fig. 2), 망막중심정맥폐쇄에서도 치료 전 43.94 ± 6.12에서 치료 후 39.3 ± 6.85로 통계적으로 유의 한 감소를 보였다(p<0.001, Fig. 3).
Spearman 상관분석을 통해 유리체내 베바시주맙 주입술 후 망막 신경절세포층의 두께에 영향을 미치는 인자들을 분 석한 결과, 치료 전후 중심망막두께의 변화가 클수록, 유리 체내 주입술 횟수가 많을수록 신경절세포층의 두께가 치료
Table 4. Multivariate regression analysis
* of variables associated with GCL thicknessVariables 95% CI* R-square* p-value*
Changes in CMT 0.0264-0.0577 0.048 <0.001
GCL = ganglion cell layer; CI = confidence interval; CMT = central macular thickness.
*Multivariate regression analysis after univariate regression 10% selection, backward elimination.
A B
C D
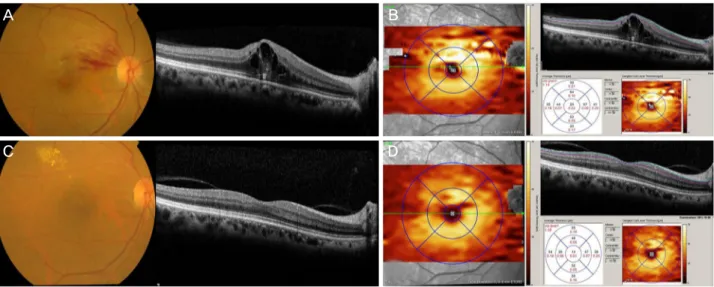
Figure 2. Changes in GCL thickness after multiple anti-VEGF injections in BRVO. Right eye of a 60-year-old woman with BRVO.
(A) Initial fundus photography and SD-OCT image with retinal hemorrhage at ST area and cystoid macular edema. (B) Initial thick- ness map of GCL in BRVO patient. (C) Fundus photography and SD-OCT image after 7 anti-VEGF injections show reduction of retinal hemorrhage and macular edema. (D) Thickness map of GCL in BRVO patient after 7 anti-VEGF injections. ETDRS = Early Treatment Diabetic Retinopathy Study; GCL = ganglion cell layer; VEGF = vascular endothelial growth factor; BRVO = branch retinal vein occlusion; SD-OCT = spectral domain optical coherence tomography; ST = superotemporal.
후 유의하게 감소하였다(각각 p=0.002, p=0.048) (Table 3).
하지만 경과관찰 기간을 보정하였을 때는 유리체내 주입술 횟수와 신경절세포층의 두께 변화가 유의한 관계를 보이지 는 않았다(p=0.093).
위의 두 인자들을 대상으로 다변량 선형회귀분석을 시행 한 결과 신경절세포층의 두께 변화는 중심망막두께(central macular thickness, CMT)의 변화에 영향을 받는 것으로 나 타났다(p=0.001) (Table 4).
고 찰
본 연구에서 저자들은 망막정맥폐쇄에서 유리체내 항혈 관내피성장인자 주입술 전후의 망막 신경절세포층의 두께 감소를 후향적인 연구를 통해 확인하였다. 기존의 연구들 을 살펴보면 망막정맥폐쇄에서 망막 신경절세포층에 비해 망막신경섬유층의 두께 변화에 대한 연구들이 더 많았
다.25-27 Shin et al28은 망막정맥폐쇄를 포함한 다양한 망막
질환에서 반복적인 항혈관내피성장인자 주입술 후 망막신 경섬유층 두께 변화에 큰 영향을 끼치지 않음을 보고하였 다.
많은 동물모델을 이용한 연구를 통해 혈관내피성장인자 가 비혈관세포에서 신경보호작용을 한다는 것을 보고하였 고 망막을 포함한 신경조직의 발달과 성숙에 주요한 역할 을 함이 알려져 있다.13,14 Foxton et al15은 녹내장질환모델 을 이용한 연구에서 혈관내피성장인자-A가 망막 신경절세 포의 생존을 촉진시키는 역할을 하며 혈관내피성장인자-A 가 차단되면 현저한 신경세포의 사멸이 진행됨을 보고하였 다. 또한 Brar et al14은 분화된 망막 신경절세포 모델에서 베바시주맙이 혈관내피성장인자의 산화스트레스에 대한 억제기능을 감소시킨다는 것을 밝혔다.27 또 다른 연구에서 는 항혈관내피성장인자가 쥐에서 직접적인 망막독성이 있 음을 보고하였다.28 하지만 형혈관내피성장인자 주입술이 망막 신경절세포층에 대해 미치는 영향을 기능적인 측면이 나 해부학적인 측면으로 보고한 연구는 없었다.
본 연구는 Spectralis software version 6.0을 이용해 자동 으로 측정되는 망막 신경절세포층의 두께를 치료 전후로 비교하였다. 이 software는 망막의 10개층을 자동으로 측정 하여 두께를 color map으로 표현하여 주므로 각 층별 두께 를 분석하는 데 많은 도움이 된다. 하지만 망막 신경절세포 층의 두께를 자동으로 측정한 것 중에서 황반 부종이 심해
A B
C D
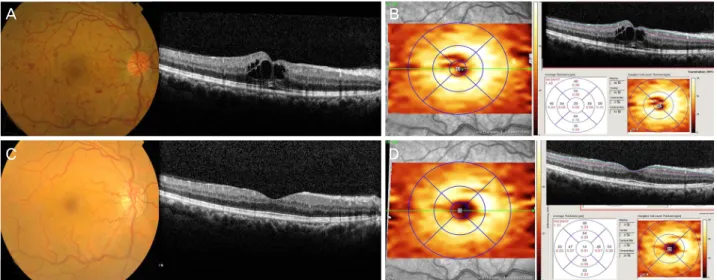
Figure 3. Changes in GCL thickness after multiple anti-VEGF injections in CRVO. Right eye of a 54-year-old man with CRVO. (A)
Initial fundus photography and SD-OCT image with diffuse retinal hemorrhage at ST area and cystoid macular edema. (B) Initial thickness map of GCL in CRVO patient. (C) Fundus photography and SD-OCT image after 4 anti-VEGF injections show reduction of retinal hemorrhage and macular edema. (D) Thickness map of GCL in CRVO patient after 4 anti-VEGF injections. ETDRS = Early Treatment Diabetic Retinopathy Study; GCL = ganglion cell layer; VEGF = vascular endothelial growth factor; CRVO = central retinal vein occlusion; SD-OCT = spectral domain optical coherence tomography; ST = superotemporal.망막 신경절세포층의 경계가 부정확한 경우 2명의 안과의 사가 각각 보정하여 평균을 내어 망막 신경절세포층 두께 를 측정하였다.
망막분지정맥폐쇄와 망막중심정맥폐쇄로 나누어서 하위 그룹 분석을 시행해 보았을 때도 두 군 모두 3회 이상의 유 리체내 항혈관내피성장인자 주입술 후 망막 신경절세포층 의 두께가 유의하게 감소하였다. 초기의 망막분지정맥폐쇄 환자와 망막중심정맥폐쇄 환자 간의 망막 신경절세포층 두 께의 두 군 간 차이가 유의하지 않은 것은 발병 초기 신경 절세포층 두께에 영향을 주는 요소들이 크게 차이가 없음 을 의미한다. 두 군 간의 측정값들 중에서는 치료 전 안압 이 망막중심정맥폐쇄 환자에서 망막분지정맥폐쇄 환자에 비해 유의하게 높았다. 이는 망막중심정맥폐쇄에서 망막중 심정맥이 사상판을 통과하는 부위에서 압박을 받는 경우도 있고, 망막중심정맥의 낮은 혈액 속도, 감소된 직경, 점성의 증가 등에 의해 안압이 상승한다고 알려져 있다.29
상관관계 분석을 통해 알아본 반복적인 유리체내 항혈관 내피성장인자주입술 후 망막 신경절세포층 두께의 변화에 영향을 미치는 인자로는 중심망막두께의 변화와 유리체내 주입술의 횟수였다(Table 3). 치료 전후 중심망막두께가 많 이 감소할수록 치료 전후 망막 신경절세포층의 두께가 더 많이 감소하였다. 망막정맥폐쇄 환자에서는 OCT 상의 수 직스캔에서 망막부종의 위치가 당뇨망막병증이나 황반변 성에 비해 조금 더 내망막 쪽에 위치함이 알려져 있으므 로,30 망막정맥폐쇄에서 망막부종의 감소가 내망막 쪽에 위
치한 망막 신경절세포층에 영향을 미친 것으로 생각된다. 유리체내 베바시주맙 주입술의 횟수 또한 치료 후 망막 신 경절세포층에 영향을 미치는 요인이었으나, 다변량 선형회 귀분석을 시행한 결과 신경절세포층의 두께 변화는 중심망 막두께(CMT)의 변화에만 영향을 받는 것으로 나타났다 (p=0.001). 또한 망막정맥폐쇄의 유병기간이 길어질수록 망 막신경절세포층이 얇아지는 것을 고려하여 경과관찰 기간 을 보정하여 분석하였을 때 유리체내 베바시주맙 주입술의 횟수와 신경절세포층의 두께 변화는 유의한 관계를 보이지 않았다(p=0.093).
혈관내피성장인자의 신경보호작용 및 망막을 포함한 신 경조직의 발달과 성숙을 촉진하는 기능이 있음은 이미 밝 혀져 있고,13,14 항혈관내피성장인자 주입술로 인해 망막 신 경절세포의 사멸이 진행됨을 보고한 연구도 있다.15 이에 반복적인 항혈관내피성장인자 주입술이 신경절세포층의 두께 및 기능에 영향을 줄 수 있을 것이라 예상해 볼 수 있 으나, 본 연구의 결과에서는 반복적인 항혈관내피성장인자 주입술 후 망막 신경절세포층의 두께 감소는 주입술의 횟 수와 유의한 관계가 없었고, 중심망막두께의 감소와 유의 한 연관성이 있었다. 하지만 본 연구는 3회 이상 주사치료 를 한 환자를 대상으로 하였고, 이미 알려진 혈관내피성장 인자의 기능을 고려했을 때 추후 주사횟수가 더 많이 늘어 나는 환자들을 대상으로 망막 신경절세포층의 두께뿐만 아 니라 기능적인 변화를 관찰할 필요가 있다. 또한 망막정맥 폐쇄 환자에서 항혈관성장인자 주입술을 반복적으로 시행
할 때 망막 신경절 세포의 변화 및 기능에 대한 고려도 필 요할 것으로 생각된다.
본 연구의 제한점은 후향적 연구이며 대상수가 적다는 점이다. 또한 망막 신경절세포층의 해부학적인 두께 변화 를 분석하였으나 망막 신경절세포층의 기능적인 변화에 대 한 연구가 이루어지지 못했다는 한계가 있다. 치료 후 망막 신경절세포층의 두께 감소가 녹내장의 발생과 관련이 얼마 나 있는지는 추후 retinal nerve fiber layer (RNFL) 및 시야 검사를 치료 전후로 시행하여 비교하는 연구가 필요하며, 앞으로의 연구는 대상 수를 늘리고 망막 신경절세포층의 기능을 평가하는 전향적 연구가 이루어져야 할 것이다. 또 한 본 연구에는 항혈관내피성장인자 주입술을 받지 않은 대조군이 포함되지 않아, 전체 망막 신경절세포층 두께 감 소 중 질환의 자연 경과에 의해 발생한 두께 감소 정도가 얼마나 차지하는지 알 수 없었다. 이에 치료 받지 않은 대 조군을 포함한 추가 연구가 필요할 것으로 생각된다.
결론적으로 망막정맥폐쇄로 인한 황반 부종에서 반복적 인 유리체내 베바시주맙 주입술 후 치료 전에 비해 망막 신 경절세포층의 두께 감소가 있었고, 이는 중심망막두께의 변화에 의한 영향이 가장 컸다.
REFERENCES
1) Klaver CC, Wolfs RC, Vingerling JR, et al. Age-specific preva- lence and causes of blindness and visual impairment in an older population: the Rotterdam Study. Arch Ophthalmol 1998;116:653-8.
2) Attebo K, Mitchell P, Smith W. Visual acuity and the causes of visu- al loss in Australia. The Blue Mountains Eye Study. Ophthalmology 1996;103:357-64.
3) The Korean Retina Society. Retina, 4th ed. Vol. 1. Seoul: Jin Printing and Communication, 2015;283-305.
4) Rehak J, Rehak M. Branch retinal vein occlusion: pathogenesis, visual prognosis, and treatment modalities. Curr Eye Res 2008;33;111-31.
5) Noma H, Funatsu H, Yamasaki M, et al. Pathogenesis of macular edema with branch retinal vein occlusion and intraocular levels of vascular endothelial growth factor and interleukin-6. Am J Ophthalmol 2005;140:256-61.
6) Yoshimura T, Sonoda KH, Sugahara M, et al. Comprehensive anal- ysis of inflammatory immune mediators in vitreoretinal diseases.
PLoS One 2009;4:e8158.
7) Fujikawa M, Sawada O, Miyake T, et al. Correlation between vas- cular endothelial growth factor and nonperfused areas in macular edema secondary to branch retinal vein occlusion. Clin Ophthalmol 2013;7:1497-501.
8) Hoeh AE, Ach T, Schaal KB, et al. Long-term follow-up of OCT-guided bevacizumab treatment of macular edema due to retinal vein occlusion. Graefes Arch Clin Exp Ophthalmol 2009;
247:1635-41.
9) Prager F, Michels S, Kriechbaum K, et al. Intravitreal bevacizumab (Avastin) for macular oedema secondary to retinal vein occlusion:
12-month results of a prospective clinical trial. Br J Ophthalmol 2009;93:452-6.
10) Ehlers JP, Decroos FC, Fekrat S. Intravitreal bevacizumab for mac- ular edema secondary to branch retinal vein occlusion. Retina 2011;31:1856-62.
11) Hikichi T, Higuchi M, Matsushita T, et al. Two-year outcomes of intravitreal bevacizumab therapy for macular oedema secondary to branch retinal vein occlusion. Br J Ophthalmol 2014;98:195-9.
12) Lee YS, Kim MS, Yu SY, Kwak HW. Two-year results of intra- vitreal bevacizumab injection in retinal vein occlusion. J Korean Ophthalmol Soc 2011;52:1039-47.
13) Carmeliet P, Ruiz de Almodovar C. VEGF ligands and receptors:
implications in neurodevelopment and neurodegeneration. Cell Mol Life Sci 2013;70:1763-78.
14) Brar VS, Sharma RK, Murthy RK, Chalam KV. Evaluation of dif- ferential toxicity of varying doses of bevacizumab on retinal gan- glion cells, retinal pigment epithelial cells, and vascular endothe- lial growth factor–enriched choroidal endothelial cells. J Ocul Pharmacol Ther 2009;25:507-11.
15) Foxton RH, Finkelstein A, Vijay S, et al. VEGF-A is necessary and sufficient for retinal neuroprotection in models of experimental glaucoma. Am J Pathol 2013;182:1379-90.
16) Tan O, Chopra V, Lu AT, et al. Detection of macular ganglion cell loss in glaucoma by Fourier-domain optical coherence tomography.
Ophthalmology 2009;116:2305-14.e1-2.
17) Kim NR, Kim JH, Lee J, et al. Determinants of perimacular inner retinal layer thickness in normal eyes measured by Fourier-domain optical coherence tomography. Invest Ophthalmol Vis Sci 2011;
52:3413-8.
18) Wollstein G, Schuman JS, Price LL, et al. Optical coherence to- mography (OCT) macular and peripapillary retinal nerve fiber lay- er measurements and automated visual fields. Am J Ophthalmol 2004;138:218-25.
19) Nakatani Y, Higashide T, Ohkubo S, et al. Evaluation of macular thickness and peripapillary retinal nerve fiber layer thickness for detection of early glaucoma using spectral domain optical coher- ence tomography. J Glaucoma 2011;20:252-9.
20) Cho JW, Sung KR, Lee S, et al. Relationship between visual field sensitivity and macular ganglion cell complex thickness as meas- ured by spectral-domain optical coherence tomography. Invest Ophthalmol Vis Sci 2010;51:6401-7.
21) Tan O, Chopra V, Lu AT, et al. Detection of macular ganglion cell loss in glaucoma by Fourier-domain optical coherence tomography.
Ophthalmology 2009;116:2305-14.e1-2.
22) Takagishi M, Hirooka K, Baba T, et al. Comparison of retinal nerve fiber layer thickness measurements using time domain and spectral domain optical coherence tomography, and visual field sensitivity.
J Glaucoma 2011;20:383-7.
23) Park CH, Lee KI, Park HY, et al. Changes in the retinal nerve fiber layer after intravitreal injections of bevacizumab in glaucoma patients. J Korean Ophthalmol Soc 2014;55:693-701.
24) Martinez-de-la-Casa JM, Ruiz-Calvo A, Saenz-Frances F, et al.
Retinal nerve fiber layer thickness changes in patients with age-re- lated macular degeneration treated with intravitreal ranibizumab.
Invest Ophthalmol Vis Sci 2012;53:6214-8.
25) Kim MJ, Woo SJ, Park KH, Kim TW. Retinal nerve fiber layer thickness is decreased in the fellow eyes of patients with unilateral retinal vein occlusion. Ophthalmology 2011;118:706-10.
= 국문초록 =
망막정맥폐쇄에서 유리체강내 베바시주맙 주사 후 신경절세포층의 두께 변화
목적: 망막정맥폐쇄 환자에서 반복적인 베바시주맙 주입술이 망막 신경절세포에 영향을 주는지 알아보고자 하였다.
대상과 방법: 후향적 연구로 치료 기왕력이 없는 60명의 망막정맥폐쇄 환자(망막분지정맥폐쇄 환자 35명 35안, 망막중심정맥폐쇄 환자 25명 25안)를 대상으로 하였다. 3회 이상의 유리체내 베바시주맙 주입술을 시행 받은 전후로 spectral domain optical coherence tomography (SD-OCT)를 이용하여 망막 신경절세포층 두께를 측정하여 비교하였다. 망막신경절세포층의 두께는 9곳의 Early Treatment Diabetic Retinopathy Study (ETDRS) 격자(grid) 영역에서 각각 측정되었고, 그 변화는 나이, 유리체내 주입술의 횟수, 안압 의 변화, 중심망막두께의 변화 등과 연관성이 있는지도 알아보았다.
결과: 반복적인 유리체내 베바시주맙 주사 후 망막 신경절세포층의 평균 두께는 42.99 ± 5.39 μm에서 38.99 ± 5.53 μm로 유의한 감소를 보였다(p<0.001). 망막 신경절세포층의 두께 변화는 중심망막두께의 변화와 유리체내 주입술 횟수와 연관이 있었다 (respectively, p=0.02, p=0.048). 하지만 다변량 선형회귀분석 결과 중심망막두께의 변화만이 치료 후 망막 신경절세포층의 두께 변화에 영향을 미치는 요인으로 나타났다(p<0.001).
결론: 망막정맥폐쇄 환자에서 반복적인 유리체내 항혈관내피성장인자 주입술 후 망막 신경절세포층의 두께는 유의하게 감소하였다.
이는 중심망막두께의 변화가 가장 큰 영향을 끼치는 것으로 보인다.
<대한안과학회지 2016;57(1):63-70>
26) Brar VS, Sharma RK, Murthy RK, Chalam KV. Bevacizumab neu- tralizes the protective effect of vascular endothelial growth factor on retinal ganglion cells. Mol Vis 2010;16:1848-53.
27) Iriyama A, Chen YN, Tamaki Y, Yanagi Y. Effect of anti-VEGF an- tibody on retinal ganglion cells in rats. Br J Ophthalmol 2007;
91:1230-3.
28) Shin HJ, Shin KC, Chung H, Kim HC. Change of retinal nerve fi- ber layer thickness in various retinal diseases treated with multiple
intravitreal antivascular endothelial growth factor. Invest Ophthalmol Vis Sci 2014;55:2403-11.
29) Williamson TH. Central retinal vein occlusion: what's the story? Br J Ophthalmol 1997;81:698-704.
30) Munk MR, Sacu S, Huf W, et al. Differential diagnosis of macular edema of different pathophysiologic origins by spectral domain optical coherence tomography. Retina 2014;34:2218-32.