Cervical transforaminal epidural steroid injections (TFESIs) play an important role in the conservative
treatment of the symptoms of neck pain with a radicular component secondary to cervical herniated interverte- bral disc (HIVD) or spinal stenosis (1-3). Although some investigators have reported no serious complications re- sulting from the use of cervical TFESIs, recent reports emphasize the risks of this procedure, including a high incidence of intravascular penetration (4) and serious brain and spinal cord injury (5-7). Therefore, it is impor- tant to consider the risks and benefits of TFESI.
MR imaging of the cervical spine combined with plain radiography represents the reference-standard examina-
Cervical Transforaminal Epidural Steroid Injection (TFESI): Role of MR Imaging and Epidurography1
Soo-Jung Choi, M.D., Jae Hong Ahn, M.D., Chunghwan Kim, M.D.2, Jae Seok Song, M.D.3, Seung Moon Jung, M.D., Dae Sik Ryu, M.D., Man Soo Park, M.D., Jong Hyeog Lee, M.D.
1Department of Radiology, GangNeung Asan Hospital, University of Ulsan College of Medicine
2Department of Orthopedic Surgery, GangNeung Asan Hospital, University of Ulsan College of Medicine
3Department of Preventive Medicine, University of Kwandong College of Medicine
Received May 31, 2010 ; Accepted October 5, 2010
Address reprint requests to : Soo-Jung Choi, M.D., Department of Radiology, Asan Foundation, GangNeung Asan Hospital, University of Ulsan, College of Medicine, 415 Bangdong-ri, Sacheon-Myeon, Gangneung-si, Gangwon-do 210-711, Korea.
Tel. 82-33-610-3485 Fax. 82-33-610-3111 E-mail: [email protected]
Purpose: To evaluate the relationship between MR/epidurographic findings and the clinical outcome after a fluoroscopy-guided transforaminal epidural steroid injection (TFESI) in patients with cervical radicular pain.
Materials and Methods: Forty-five patients who had taken a cervical TFESI in our de- partment were included in this study. We retrospectively reviewed MR and epiduro- graphic findings to see if there was a relationship between these methods and the amount of pain relief, by way of a multiple regression analysis.
Results: On MR imaging, there was significant relationship between the amount of pain relief and location of herniated intervertebral disc (HIVD, central: 54.4%, lateral recess: 69.4%, foraminal: 59%; p = 0.048). There was no significant difference regard- ing the other MR findings. On epidurographic findings, there was significant differ- ence in the amount of pain relief with the extent of the contrast (epidural and epineur- al space, 65.3%; epineural space only, 64.2%; p = 0.03) and location of the needle tip (in the foramen, 59.4%; outside the foramen, 68.4%; p = 0.002).
Conclusion: The results indicate that TFESI could be more useful in patients with cer- vical HIVD in lateral recess rather than another location. Contrast spread into epidural reflux appears to be a favorable injection pattern. Needle tip location is recommended outside the foramen rather than in the foramen.
Index words :Fluoroscopy
Magnetic Resonance Imaging Spine
Injection, Epidural
tion for the work-up of patients with cervical radicular pain (8, 9). Moreover, recent reports have attempted to evaluate whether MR imaging findings of the spine can predict the effectiveness of pain relief following epidural injections and assist in appropriate patient selection (10- 12).
Fluoroscopic needle placement and epidurographs with contrast can also provide visual confirmation of ac- curate needle placement and the distribution and extent of drug delivery during the procedure (13-15). However the detailed techniques are not standardized and various epidurographic findings are observed during the proce- dure. The purposes of the present study were to evalu- ate which MR findings are indicators that a patient will likely benefit from cervical TFESI, and to suggest suit- able epidurographic findings and needle position while performing the procedure.
Materials and Methods
Patients
Institutional review board approval and written in- formed consent were obtained for this study. Between January 2004 and August 2006, 51 consecutive patients (31 males and 20 females: mean age, 38 years; age range, 33-66 years) were treated at our department by cervical transforaminal epidural steroid injection (TFE- SI) for unilateral cervical radicular pain. All of 51 pa- tients underwent cervical spine MR imaging before the injection (interval range, 1 day to 2 months). The indica- tion for TFESI was unilateral cervical radicular pain without significant motor/sensory deficit. The level of the injection site was decided by consensus between an orthopedic surgeon and a musculoskeletal radiologist af- ter considering the patient’s history as well as the results of physical examinations, plain radiographs, MR imag- ing findings, and electrodiagnostic studies. In the case of bilateral cervical radicular pain, interlaminar ESIs were performed instead of TFESIs. Exclusion criteria were as follows: 1) clinically or MR documented myelopathy, 2) progressive neurological deficits, 3) recent epidural steroid injections, and 4) an allergic reaction to local anesthetics/contrast/corticosteroids or a blood coagula- tion disorder.
Forty-five of 51 patients (26 males and 19 females:
mean age, 26 years; age range, 33-66 years) underwent a short-term follow-up within 1 month after the injec- tion (mean interval, 18 days = 2.6 weeks; range, 7-28 days). Follow-ups for the remaining 5 of 51 patients
were lost. All patients were requested to state their visu- al analogue scale (VAS) ranging from 1 to 10 at every vis- it before and after injection: the pain relief according to VAS after injection was calculated as a percentage (%) compared with that before injection.
Injection Technique
All cervical TFESIs were performed as outpatient pro- cedures by a musculoskeletal radiologist with experi- ence in spinal interventions since March 2000. All pro- cedures were performed in a sterile manner and under fluoroscopic guidance. Patients were placed in the supine position on the fluoroscopy table with the head turned to the asymptomatic side. The C-arm was rotated to an ipsilateral oblique angle with respect to the sus- pected foramen. Lidocaine (1%) was used for cutaneous and needle tract anesthesia. A 22-gauge spinal needle was aimed at a superior articular process to avoid the vertebral artery, before being introduced along the pos- terior border of the neural foramen. The C-arm was ro- tated to the anterior-posterior (AP) angle to confirm the depth of the needle. Epidurography was obtained by in- jecting 1-2 mL of Omnipaque 300 contrast material (OHEXOL, 300 mg of iodine per milliliter; Amersham Health, Princeton, NJ, USA). At least two AP epiduro- graphs were obtained. After confirming contrast filling in the periradicular space in the absence of vascular fill- ing, 0.5 mL of triamcinolone acetonide suspension (Triamcinolone 40 mg; Dongkwang, Seoul, Korea) was injected as a long-acting steroid after slowly injecting 0.3 mL of 0.2% ropivacaine (Naropin 0.2%; AstraZeneca, Westborough, MA, USA).
Analysis of MR Images and Epidurographs
Cervical spine MR images were performed at our in- stitution for all 45 patients using 1.0 T (Impact Expert;
Siemens Medical Solutions, Erlangen, Germany) or 3.0 T (Intera Achieva 3T; Philips Medical Systems, Best, Netherlands) MR units. All MR images were retrospec- tively reviewed in consensus by two radiologists using a picture archiving and communication system (PACS) working station (Marosis M-view 4.0; Marotech, Seoul, Korea). The reviewers were informed of the patients’
symptoms and the level of cervical TFESI. The MR find- ings were assessed at the level of the TFESI with regard to the causes, degree, and sites of nerve root compres- sion, presence or absence of herniated intervertebral disc (HIVD), location of HIVD, and the presence or ab- sence of foraminal/canal stenosis. The causes of nerve
root compression were classified as HIVD, foraminal stenosis, or mixed. The degree of nerve root compres- sion was classified as 1 (abutment), 2 (displacement), or 3 (entrapment) for intra-spinal canal lesions, and classi- fied as 1 (foraminal encroachment < 1/3 foraminal di- ameter), 2 (1/3-1/2), or 3 (> 1/2) for a foraminal lesion.
The sites of nerve root compression were classified as lateral recess or foraminal. Location of HIVD was classi- fied as central, lateral recess, or foraminal. Foraminal stenosis was diagnosed when the findings of uncoverte- bral joint hypertrophy and encroachment of the neural foramen and spinal canal stenosis were diagnosed when the sagittal diameter of the cervical canal was 10 mm or less.
All epidurographic findings were retrospectively re- viewed by the radiologist who had performed the TFESIs. The extent of contrast spread was classified based on the visualization of the contrast in the epidural
space (both epidural and epineural spaces), or only in the epineural space (epineural space only) (Fig. 1). The location of the needle tip was evaluated, either in the foramen or outside the foramen on a frontal radiogra- phy.
Statistical Analysis
A multiple regression analysis with a control for age, sex, and follow-up periods was performed to determine factors of MRI or epidurographic findings contributing to significant pain relief. Data were analyzed by using the SAS system for Windows 9.12 (SAS, Cary, SC, USA).
A Pearson’s correlation was used to evaluate the rela- tionship among the variables.
Results
Mean pain relief after cervical TFESI was 65% on VAS
A
Fig. 1. Anterior-posterior (AP) projec- tion epidurographs for the extent of contrast spread.
A. Visualization of the contrast both in the epidural and epineural spaces.
B. Contrast filling only in the epineural space.
B
at short term follow-up (mean interval, 2.6 weeks;
range, 7 - 28 days). Thirty-seven of 45 patients (82.2%) showed pain relief greater than 50% after cervical TFESIs at the same follow-up periods. Left-side injec-
tions were performed in 29 of 45 patients and right-side injections were performed in 16 patients. The most fre- quently injected level was C5-6 (23 patients): The C6-7 level was injected in 17 patients, while the C4-5 level
A B C
Fig. 2. MRI and epidurography of a 39-year-old female patient with left posterior shoulder and arm pain.
A, B. T2-weighted sagittal (A) and T1-weighted axial (B) MR images show lateral recess HIVD (arrows) with grade III nerve root compression. The site of nerve root compression is at the lateral recess level.
C. Epidurography shows smooth contrast spread with contrast filling only in the epineural space. The needle tip is located outside the foramen. The patient achieved about 71% pain reduction, 2 weeks after a left C6 TFESI.
A B C
Fig. 3. MRI and epidurography of a 40-year-old female patient with left radiating pain.
A, B. T2-weighted sagittal (A) and gradient echo axial (B) MR images show foraminal HIVD (arrows). The degree of nerve root com- pression was graded I.
C. Epidurography shows smooth contrast spread with lateral epidural extension (curved arrow). The needle tip is located outside the foramen. The patient achieved about 80% pain reduction, 2 weeks after a left C5 TFESI.
was injected in 5 patients. There were no reported side effects of neurologic deficit, vertigo, seizure like motion, dural puncture, bleeding or infection.
An MR analysis revealed a significant relationship be- tween the degree of pain relief and the location of HIVD (central, 54.4 %; lateral recess, 69.4%; foraminal, 59%; p
= 0.048) (Fig. 2). None of the other MR parameters were significantly associated with pain relief (Table 1).
An epidurography analysis revealed significant rela- tionships between the degree of pain relief and extent of contrast (both epidural and epineural spaces, 65.3%;
epineural space only, 64.2 %; p = 0.03) (Fig. 3) as well as the location of the needle tip (in the foramen, 59.4%;
outside the foramen, 68.4 %; p = 0.002) (Table 2, Fig. 4).
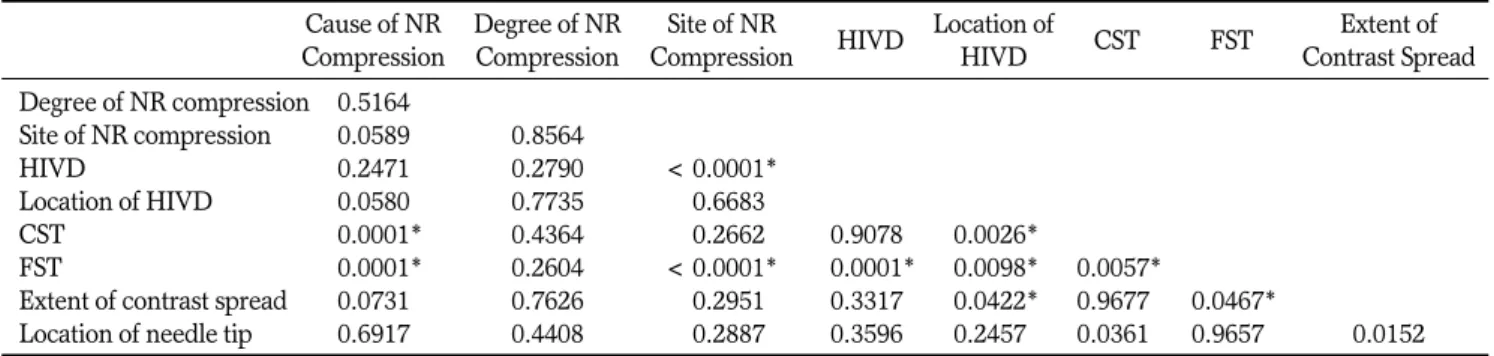
However, a Pearson’s correlation test revealed a signifi- cant relationship between the location of HIVD and the
extent of contrast, but there was no correlation between the location of HIVD and the location of the needle tip (Table 3). We also evaluated the relationship between
Table 1. Association of MR findings and Pain Relief After a Cervical TFESI
Cause of NR Degree of NR Site of NR Location of Compression Compression Compression HIVD
HIVD CST FST
HIVD FST Mixed 1 2 3 LR Foramen A P Central LR Foramen A P A P
No. of Pts. 17 19 9 8 17 20 19 26 17 28 5 19 4 12 34 17 28
Mean pain
relief (%) 64.1 66.8 63.5 59.9 62.5 69.2 68.8 62.5 67 64.5 54.4 69.4 59 65.5 63.5 64.1 65.6
p value 0.266 0.125 0.3935 0.152 0.048* 0.088 0.737
Note.─TFESI = transforaminal epidural steroid injection, NR = nerve root, HIVD = herniated intervertebral disc, CST = canal stenosis, FST = foraminal stenosis, LR = lateral recess, A = absence, P = presence, No. = number, Pts = patients. * Indicates a statistically signif- icant value (p < 0.05, multiple regression analysis).
Table 2. Association of Epidurographic Findings and Pain Relief After a Cervical TFESI
Extent of Contrast Spread Location of Needle Tip Both epidural Epineural In the Outside the and epineural space only foramen foramen
spaces
No. of Pts. 36 9 17 28
Mean pain
relief (%) 65.3 64.2 59.4 68.4
p value 0.03* 0.002*
Note.─TFESI = transforaminal epidural steroid injection, No. = number, Pts = patients.* Indicates a statistically significant value (p < 0.05, multiple regression analysis).
A B C
Fig. 4. MRI and epidurography of a 53-year-old male patient with radicular pain on his right side.
A, B. T2-weighted sagittal (A) and gradient echo axial (B) MR images show uncovertebral joint hypertrophy with foraminal stenosis (arrows) and grade III nerve root compression in right C5-6.
C. Epidurography shows contrast spread with epidural extension (arrowheads). The needle tip is located in the foramen and the patient achieved about a 40% reduction in pain, 2 weeks after a right C6 TFESI.
the location of HIVD and extent of the contrast (Table 4), which revealed the tendency of the contrast medium to be confined to the epineural space in the foraminal lo- cating disc herniation. However, the degree of pain re- lief was not affected by the extent of the contrast.
Discussion
Two routes are commonly used for cervical epidural steroid injections: interlaminar and transforaminal injec- tions. Although appropriate indications for both tech- niques are not standardized, interlaminar techniques are usually preferred in patients with bilateral radicular pain, while transforaminal techniques are preferred in patients with unilateral or foraminal disease. The trans- foraminal technique has a theoretical advantage in that it delivers the drug directly around the nerve root.
However, following recent reports of the risks of TFESI (5-7), it is becoming increasingly necessary to conduct studies to assess which patients will most benefit from TFESI, regardless of the risk.
The present study identified a significant relationship between the location of the HIVD on MR images and the degree of pain relief after a TFESI. This result sug- gests that a TFESI can be more useful in patients with HIVD in the lateral recess rather than other HIVD loca- tions or stenosis patients. In addition, nerve root com-
promise at the lateral recess showed greater pain relief compared to the foraminal level in the present study, even though the result was not statistically significant.
In a similar study, Strobel et al. had reported that pa- tients with foraminal disc herniation and foraminal nerve root compromise showed the greatest pain amount of relief immediately after a CT-guided cervical nerve root block (10). These results are not do not agree with those of the present study. We assume that this dis- crepancy was caused by the time difference after the in- jection. Because immediate pain relief is caused in most cases by the accompanying local anesthetics, a forami- nal lesion is more likely to benefit immediately after transforaminal drug delivery, compared to a lateral re- cess or other intraspinal lesion; however, the effect of the local anesthetics decreases over time, and that of the steroid begins to act on the lesion. In the present study, we retrospectively reviewed the clinical outcome at short-term follow-up (mean, 2.6 weeks). Although these follow-up periods also do not represent long-term re- sults, we consider that the outcomes of this period are crucial in deciding whether conservative treatment in- cluding repeat injections, should be maintained or not (16).
We also evaluated the relationship between the epidurographic findings and clinical outcome. Although all procedures were technically successful and 37 of 45 patients (82.2%) showed a successful outcome (pain re- lief greater than 50%) after a cervical TFESI at their short-term follow-up periods (mean, 2.6 weeks), con- trast filling around the nerve with epidural reflux showed greater pain relief than epineural contrast filling alone in the present study. However, Pearson’s correla- tion test revealed a significant relationship for extent of contrast, location of HIVD, and foraminal stenosis. In other words, in the cases with the foraminal stenosis or Table 4. Relationship between Location of HIVD and Extent of
Contrast
Extent of Contrast/
Location of HIVD Central Lateral Recess Foraminal Both epidural and
epineural spaces 5 (54.4%) 17 (67.1%) 2 (47.9%) Epineural space only 0 02 (74.2%) 2 (70%)0.
Note.─Data represent the number of patients. Figures in paren- thesis refer to the mean degree of pain relief.
Table 3. Results of a Pearson’s Correlation Analysis
Cause of NR Degree of NR Site of NR Location of Extent of
Compression Compression Compression HIVD
HIVD CST FST
Contrast Spread Degree of NR compression 0.5164
Site of NR compression 0.0589 0.8564
HIVD 0.2471 0.2790 < 0.0001*
Location of HIVD 0.0580 0.7735 <0.6683
CST 0.0001* 0.4364 <0.2662 0.9078 0.0026*
FST 0.0001* 0.2604 < 0.0001* 0.0001* 0.0098* 0.0057*
Extent of contrast spread 0.0731 0.7626 <0.2951 0.3317 0.0422* 0.9677 0.0467*
Location of needle tip 0.6917 0.4408 <0.2887 0.3596 0.2457 0.0361 0.9657 0.0152 Note.─Data are expressed as p-values. * indicates a statistically significant correlation between the variables (p < 0.05). NR = nerve root, HIVD = herniated intervertebral disc, CST = central spinal stenosis, FST = foraminal stenosis
foraminal locating HIVD, there was a tendency for con- trast filling to be limited in the epineural space only, rather than epidural reflux. Therefore, even though we could not say to what extent of contrast is the main pre- dictive variable for the clinical outcome after cervical transforaminal ESI, but we could be sure that contrast spread in both the epidural and epineural spaces ap- pears to be a favorable injection pattern while perform- ing the procedure. In addition, the needle tip location outside the foramen showed greater pain relief rather than needle tip location in the foramen. This result was not significantly affected by other MR variables and could give us methodological grounds for depth of the needle location. The periradicular foraminal space is small and contains some fibrotic tissue. In particular, the superficial layer of the posterior longitudinal liga- ment is connected to the periradicular sheath anchoring the pedicle (17). When the needle tip is located in the small periradicular foraminal space, the contrast could initially collect on one side of the periradicular space without spreading to the other side around the nerve root. In addition, Ma et al. reported that the rate of com- plications associated with deep needle position on the frontal view was slightly higher than for a superficial needle position (18). In those circumstances, we can as- sert that the intentional introduction of the needle tip in- to the neural foramen has no clinical benefit and cannot be necessary.
The present study had several limitations. First, the follow-up periods of the patients after TFESI were not uniform and short because of the retrospective nature of this study. This is a major limitation of our study; how- ever, the range was not wide (1-4 weeks), and most of the patients (43 of 45 patients) were followed-up within 2-3 weeks. To overcome this limitation, we treated the data statistically treated it by multiple regression analy- sis which can control the various follow-up periods.
Second, multiple-level lesions were not considered;
therefore the possibility of injection at the wrong level could not be excluded. Third, the amount of contrast material used in obtaining epidurographs was small, and lateral and oblique views were not routinely ob- tained; however, 2 cc of contrast or less is usually enough to confirm needle placement and drug delivery.
We did not use a large amount of contrast during the procedure. Fourth, large population studies would be needed, because of small number of subjects in this study.
In conclusion, cervical TFESI can be useful in patients
with cervical radicular pain. Among them, patients with MR revealed HIVD in the lateral recess gained the most significant benefit at the short-term follow-up after in- jection in the present study. Contrast spread in both the epidural and epineural spaces appears to be a favorable injection pattern while performing the procedure. In ad- dition, it is recommended that the needle tip be located outside the foramen rather than in the foramen.
References
1. Slipman CW, Lipetz JS, Jackson HB, Rogers DP, Vresilovic EJ.
Therapeutic selective nerve root block in the nonsurgical treat- ment of atraumatic cervical spondylotic radicular pain: a retro- spective analysis with independent clinical review. Arch Phys Med Rehabil 2000;81:741-746
2. Bush K, Hiller S. Outcome of cervical radiculopathy treated with periradicular/epidural corticosteroid injections: a prospective study with independent clinical review. Eur Spine J 1996;5:319-325 3. Rathmell JP, Aprill C, Bogduk N. Cervical transforaminal injection
of steroids. Anesthesiology 2004;100:1595-1600
4. Furman MB, Giovanniello MT, O’Brien EM. Incidence of intravas- cular penetration in transforaminal cervical epidural steroid injec- tions. Spine 2003;28:21-25
5. Brouwers PJ, Kottnik EJ, Simon MA, Prevo RL. A cervical anterior spinal artery syndrome after diagnostic blockade of the right C6- nerve root. Pain 2001;91:397-399
6. Baker R, Dreyfuss P, MercerS, Bogduk N. Cervical transforaminal injection of corticosteoids into a radicular artery: a possible mecha- nism for spinal cord injury. Pain 2003;103:211-215
7. Scanlon GC, Moeller-Bertram T, Romanowsky SM, Wallace MS.
Cervical transforaminal epidural steroid injections: more danger- ous than we think? Spine 2007;32:1249-1256
8. Boutin RD, Steinbach LS, Finnesey K. MR imaging of degenerative diseases in the cervical spine. Magn Reson Imaging Clinic N Am 2000;8:471-490
9. Brown MN, Schwartz RH, Frank E, Blank NK. Preoperative evalu- ation of cervical radiculopathy and myelopathy by surface-coil MR imaging. AJR Am J Roentgenol 1988;151:1205-1212
10. Strobel K, Pfirrmann CW, Schmid M, Hoder J, Boos N, Zanetti M.
Cervical nerve root blocks: indications and role of MR imaging.
Radiology 2004;233:87-92
11. Choi SJ, Song JS, Kim C, Ryu DS, Ahn JH, Jung SM, et al. The use of magnetic resonance imaging to predict the clinical outcome of non-surgical treatment for lumbar intervertebral disc herniation.
Korean J Radiol 2007;8:156-163
12. Jeong HS, Lee JW, Kim SH, Myung JS, Kim JH, Kim JH, et al.
Effectiveness of transforaminal epidural steroid injection by using a preganglionic approach: a prospective randomized controlled study. Radiology 2007;245:584-590
13. Johnson BA, Schellhas KP, Pollei SR. Epidurography and thera- peutic epidural injections: technical considerations and experience with 5334 cases. AJNR Am J Neuroradiol 1999;20:697-705 14. Manchikanti L, Cash KA, Pampati V, McManus CD, Damron KS.
Evaluation of fluoroscopically guided caudal epidural injections.
Pain Physician 2004;7:81-92
15. Botwin KP, Natalicchio J, Hanna A. Fluoroscopic guided lumbar interlaminar epidural injections: a prospective evaluation of epidurography contrast patterns and anatomincal review of the
epidural space. Pain Physician 2004;7:77-80
16. Boswell MV, Shah RV, Everett CR, Sehgal N, McKenzie Brown AM, Abdi S, et al. Interventional techniques in the management of chronic spinal pain: evidence-based practice guidelines. Pain Physician 2005;8:1-47
17. Kubo Y, Waga S, Kojima T, Matsubara T, Kuga Y, Nakagawa Y.
Microsurgical anatomy of the lower cervical spine and cord.
Neurosurgery 1994;34:895-902
18. Ma DJ, Gilula LA, Riew KD. Complications of fluoroscopically guided extraforaminal cervical nerve blocks. An analysis of 1036 injections. J Bone Joint Surg Am 2005;87:1025-1030
대한영상의학회지 2011;64:25-32
경추의 경추간공 경막외 스테로이드 주사요법:
자기공명영상과 경막외조영영상의 역할1
1울산대학교 의과대학 강릉아산병원 영상의학과
2울산대학교 의과대학 강릉아산병원 정형외과
3관동대학교 의과대학 예방의학과
최수정∙안재홍∙김정환2∙송재석3∙정승문∙류대식∙박만수∙이종혁
목적: 경추부의 경추간공 경막 외 스테로이드 주사요법을 받은 환자에서 시술 전의 자기공명영상과 경막외조영영상 소견을 시술 후 임상경과와 비교하고자 한다.
대상과 방법: 경추부 병변으로 투시장비 유도 하 경추간공 경막외 스테로이드 주사요법을 받은 45명 환자의 자기공 명영상과 경막외조영영상 소견을 후향적으로 분석하여 환자의 동통 감소 정도와 비교, 통계처리하였다. 환자의 동통 감소 정도는 visual analog pain scale을 시술 전과 후 문진하여 백분율로 표시하였다.
결과: 자기공명영상 소견 중 추간판탈출증의 위치는 특히 외측함요에 위치할 때 동통감소가 많았다(central:
54.4%, lateral recess: 69.4%, foraminal: 59%; p = 0.048). 경막외조영영상 소견에서는 조영제의 확산 범위 가 신경근 주변에만 있는 경우보다 경막 외 공간까지 확산된 경우 더 동통감소가 많았고(epidural and epineural space, 65.3%; epineural space only, 64.2%; p = 0.03), 바늘의 위치는 신경공안에 있을 때보다 바깥쪽에 있 을 때 더 동통감소가 많았다(in the foramen, 59.4%; outside the foramen, 68.4%; p = 0.002).
결론: 경추부의 경추간공 경막 외 스테로이드 주사요법은 특히 추간판탈출증의 위치가 외측함요에 있는 경우 좋은 적응증이 될 수 있으며, 시술 시 바늘의 위치는 신경공 밖에서 조영제가 경막외 공간까지 확산되도록 하는 것이 바람 직하다.