한의표준임상진료지침 개발을 위한 유방암 보완치료 실태조사
1 경희대학교 대학원 임상한의학과, 2 경희대학교 한의과대학 부인과교실
3 경희대학교 한의과대학 예방의학교실
김남훈 1 , 강나훈 1 , 유은실 1 , 박남춘 1 , 이진욱 1 , 박경선 2 , 이진무 2 , 이창훈 2 , 장준복 2 , 장보형 3 , 황덕상 2
ABSTRACT
A Survey on Treatment of Breast Cancer Patients with Korean Medicine:
Preliminary Research for Clinical Practice Guidelines
Nam-Hoon Kim 1 , Na-Hoon Kang 1 , Eun-Sil Yoo 1 , Nam-Chun Park 1 , Jin-Wook Lee 1 , Kyoung-Sun Park 2 , Jin-Moo Lee 2 , Chang-Hoon Lee 2 ,
Jun-Bock Jang 2 , Bo-Hyoung Jang 3 , Deok-Sang Hwang 2
1 Dept. of Clinical Korean Medicine, Graduate School, Kyung Hee University
2 Dept. of Gynecology, College of Korean Medicine, Kyung Hee University
3 Dept. of Preventive Medicine, College of Korean Medicine, Kyung Hee University Objectives: To determine the current status of the treatment of breast cancer patients by Korean Medicine doctors (KMDs) and to examine the need for clinical practice guidelines (CPGs) for the supportive care of these patients.
Methods: This cross-sectional study used a self-administered questionnaire. Participants were asked about their experience in treating breast cancer patients; the number of breast cancer patients they currently treat; the main complaints expressed by, diagnoses of, and treatments used for such patients; and their opinions about Korean Medicine (KM) as the basis for providing supportive care for breast cancer.
Results: The data for this study were collected from 322 respondents. 84 of whom reported having ever treated patients with breast cancer. Most breast cancer patients who visited the KM clinic were classified as stage I or Ⅱ, and their major complaints were fatigue, general weakness and musculoskeletal pain. The major diagnostic strategies were syndrome differentiation and pulse diagnosis. The major treatments administered were herbal medicine, acupuncture, and moxibustion. KMDs cited a need for medical information, such as CPGs, as their most important concern with regard to the treatment of breast cancer patients.
Conclusions: This survey determined the prevalence of the use of KM for Korean breast cancer patients. Our results underscore the need for clinical practice guidelines for using of KM as the basis of supportive care for breast cancer and for informing clinicians and patients about this approach.
Key Words: Breast Cancer, Supportive Care, Cross-sectional Study, Clinical Practice Guidelines, Korean Medicine
1 0)
“본 연구는 한국보건산업진흥원을 통해 보건복지부 한의약선도기술개발사업의 재정 지원을 받아 수행된 연구임(HB16C0072).”
“This study was supported by the Traditional Korean Medicine R&D Program funded by the Ministry of Health & Welfare through the Korea Health Industry
Development Institue (KHIDI) (HB16C0072).”
Corresponding author(Deok-Sang Hwang) : Kyung Hee University Korean Medicine Hospital, 23, Kyungheedae-ro, Dongdaemun-gu, Seoul, Republic of Korea
Tel : 02-958-9160 E-mail : [email protected]
Ⅰ. Background
Breast cancer is the most common cancer worldwide. In 2015, almost 232,000 women in the United States were diagnosed with invasive breast cancer 1) . Moreover, the incidence of breast cancer is rapidly increasing in Korea due to recent changes in diet and lifestyle 2) . According to the annual report of the Korean Central Cancer registry, the incidence of breast cancer is 17.6%, rendering it second only to thyroid cancer, which has an incidence of 23.6% 3) . Additionally, the 5-year relative survival rate for invasive breast cancer is also increasing due to the revitalization of screening and the development of new technology. As a result, the survival rate of breast cancer patients in Korea is expected to increase gradually to 91.5% 4) . However, despite this high survival rate, the quality of life of breast cancer patients is lower than that of patients with other types of cancer 5) .
As breast cancer has a higher incidence of recurrence, even after 5 years, compared to other solid tumors, breast cancer survivors suffer more distress over time because of concerns about recurrence 6) . Additionally, breast cancer chemotherapy may cause fatigue, apathy, nausea, malaise, insomnia, and anorexia, and may also affect sexual performance by acting directly on the ovarian or endocrine system 7) . Tamoxifen, which decreases breast cancer recurrence, commonly causes a range of
side effects, such as hot flashes, night sweats, gynecologic symptoms (vaginal dryness, vaginal discharge), depression, forgetfulness, sleep alterations, weight gain, and diminished sexual functioning 8) .
To manage symptoms, prevent toxicity, and improve quality of life, the majority of breast cancer patients use complementary therapies during and after cancer treatment 9) . An estimated 33-47% of individuals throughout the world who have been diagnosed with cancer use complementary, alternative, or integrative therapies during cancer treatment 10) . In Korea, more than two-thirds of cancer patients used various kinds of complementary and alternative medicine, and 31% of cancer patients use Korean medicine (KM) treatment 11,12) .
Many of these cancer patients use KM treatment to alleviate a variety of symptoms, but there are currently no clinical practice guidelines (CPGs) for the use of this treatment to provide supportive care for breast cancer patients in Korea. Recent randomized controlled clinical trials have shown that KM treatment is effective and safe for cancer patients 13-5) , but this has not been communicated to patients or doctors.
Thus, standardized KM CPGs are needed to guide evidence-based, complementary therapies.
Currently, the Ministry of Health and
Welfare in Korea uses one of the standard
CPGs for breast cancer supplementation
therapy, as the basis for the development
of standard Korean CPGs. We are working
to develop a KM approach to treatment that improves the quality of life and health of breast cancer patients. To this end, we administered a questionnaire survey to Korean Medicine doctors (KMDs) to examine their awareness of Korean standard CPGs and to ascertain the current status of treating breast cancer patients with KM.
Ⅱ. Methods
1. Subjects
Subjects were KMDs who were affiliated with the Association of Korean Medicine.
2. Criteria
With the assistance of the Association of Korean Medicine, we sent the questionnaire to all affiliated KMDs by e-mail between March 30 and April 10, 2017. KMDs who had incorrect or missing e-mail addresses, and those who did not agree to participate in the survey, were excluded.
3. Content
The total number of questionnaires is 16. Participants were asked to provide information about their demographic characteristics; experience treating breast cancer patients; average number of breast cancer patients; patients' major complaints, diagnoses, and treatments; and opinions about the use of KM to provide supportive care for breast cancer. This study received
approval from the Institutional Review Board (IRB) of Kyung Hee University (KHSIRB-17-013(RA)).
Ⅲ. Results
E-mails providing an explanation regarding the study, a consent form, and online questionnaire were sent to 18,289 KMDs who were members of the Association of Korean Medicine. We analyzed data from 322 respondents.
1. Demographic characteristics Of the respondents, 232 (72.0%) were male, and 90 (28.0%) were female. In terms of the age distribution of the sample, 39.1% were aged 30-39 years and 31.7% were aged 40-49 years. In terms of professional experience, 102 (31.7%) respondents had been practicing for 11-20 years and another 102 (31.7%) had been practicing for 0-5 years.
Additionally, 84 (26.1%) of the KMDs
had ever treated patients diagnosed
with breast cancer (Table 1).
Variable N %
Gender Male 232 72.0
Female 90 28.0
Age (years)
20-29 44 13.7 30-39 126 39.1 40-49 102 31.7 50-59 43 13.4 Above 60 7 2.2
Years in practice
0-5 102 31.7
6-10 67 20.8
11-20 102 31.7 21-30 40 12.4
> 31 11 3.4 Provide KM*
treatment?
Yes 84 26.1
No 238 73.9
*KM : Korean medicine
Table 1. Demographic Characteristics of the Respondents
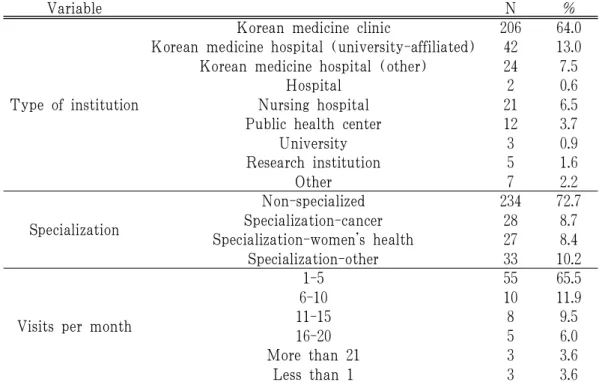
2. Medical Institution Characteristics Of the respondents, 206 practiced in KM clinics, 42 practiced in a university- affiliated KM Hospital, and 21 practiced in nursing hospitals. The majority of the respondents (234) practiced in non- specialized medical institutions.
According to our results, 55 (65.5%) breast cancer patients visited a medical institution with which respondents were affiliated one to five times per month, and 78 (92.9%) did so 20 or fewer times per month (Table 2).
Variable N %
Type of institution
Korean medicine clinic 206 64.0 Korean medicine hospital (university-affiliated) 42 13.0 Korean medicine hospital (other) 24 7.5
Hospital 2 0.6
Nursing hospital 21 6.5
Public health center 12 3.7
University 3 0.9
Research institution 5 1.6
Other 7 2.2
Specialization
Non-specialized 234 72.7
Specialization-cancer 28 8.7
Specialization-women’s health 27 8.4
Specialization-other 33 10.2
Visits per month
1-5 55 65.5
6-10 10 11.9
11-15 8 9.5
16-20 5 6.0
More than 21 3 3.6
Less than 1 3 3.6
Table 2. Medical Institutions and Specializations of the Respondents
3. Clinical practice patterns of respondents Most breast cancer patients were of stage I or Ⅱ according to the TNM
staging criteria.
The major complaints of breast cancer
patients were fatigue and general weakness,
followed by musculoskeletal pain and anorexia.
Syndrome differentiation was the most common diagnostic method used for breast cancer patients, followed by pulse diagnosis and questionnaires.
The most common treatment for breast cancer patients was herbal medicine, followed
by acupuncture and moxibustion.
Most respondents believed that herbal medicines should be used aggressively for patients with breast cancer, but 24 (28.6%) endorsed minimal and short-term prescriptions, and 10 (11.9%) were reluctant to prescribe these medicines at all (Table 3).
Variable N %
TNM stage
Stage 0 38 45.2
Stage I 78 92.9
Stage Ⅱ 78 92.9
Stage Ⅲ 57 67.6
Stage Ⅳ 37 44.0
Uncertain 50 59.5
Complaints
Fatigue and general weakness 77 91.7
Musculoskeletal pain 54 64.3
Anorexia 47 56.0
Neurosis 37 44.0
Edema 31 36.9
Hot flashes 24 28.6
Vomiting 23 27.4
Blood component reduction
(decrease in red blood cells, platelets, lymphocytes) 22 26.2
Alopecia 10 11.9
Other 13 15.5
Diagnostic method
Syndrome differentiation 79 94.0
Pulse diagnosis 62 73.8
Questionnaire 59 70.2
Korean medicine instrument 46 54.8
Abdominal diagnosis 43 51.2
Sasang constitution 35 41.7
Other 12 14.3
Treatment
Acupuncture 81 96.4
Moxibustion 58 69.0
Herbal medicine 49 58.3
Cupping 41 48.8
Pharmaco-acupuncture 32 38.1
Electro-acupuncture 21 25.0
Opinion about the use of herbal
medicine
Prescribe aggressively 41 48.8
Prescribe minimally and in the short-term 24 28.6
Reluctant 10 11.9
Never use 2 2.4
Other 7 8.3
Table 3. Clinical Practices of the Respondents
4. Opinion about KM clinical practice guidelines for supportive care for breast cancer
As described above, 238 (73.9%) KMDs had never treated breast cancer patients.
The reasons cited for not treating patients with breast cancer were that few appointments were made by such patients and that there was a lack of medical information about breast cancer. The lack of evidence related to the treatment of breast cancer has been the focus of considerable discussion.
Most respondents said they would be
willing to adhere to CPGs for breast cancer supplementation therapy if they were available.
According to our data, the most pressing need related to the medical treatment of breast cancer was the development of systematized medical information, such as CPGs. The second most urgent need was to expand health insurance coverage for medical treatment.
In total, 96.3% of respondents agreed that there was a need for KM CPGs for breast cancer patients.
Variables N %
Reasons for not treating breast cancer patients
Few patient visits 187 78.6 Lack of information 31 13.0
Lack of evidence 11 4.6
Low fees 2 0.8
Minimal effectiveness 1 0.4
Other 6 2.5
Requirements for treating breast cancer patients with KM*
Development of clinical practice guidelines 115 48.3 Expansion of health insurance 61 25.6 Expansion of casualty insurance 29 12.2 Active participation 14 5.9
Other 19 8.0
Necessity Yes 310 96.3
No 12 3.7
*KM : Korean medicine
Table 4. Opinions about KM* CPGs for Supportive Care for Breast Cancer
Ⅳ. Discussion
In Korea, 31% of cancer patients use KM treatment 11) . Nevertheless, as there is no consensus approach to the use of KM, it is difficult to recommend KM treatment for breast cancer patients. We performed this study to fill the gap caused
by the absence of CPGs for the use of KM for the supportive care of breast cancer patients in Korea.
This cross-sectional study used a
self-administered questionnaire that was
emailed to 18,289 KMDs who were members
of the Association of Korean Medicine,
and which included an explanation of
the study, a consent form, and online questionnaire between March 30 and April 10, 2017. The data analyzed in this study were from 322 respondents (1.76%).
In total, 84 (26.1%) respondents had ever treated patients with breast cancer.
Most patients were in stage I or Ⅱ, and the main symptoms were fatigue and general weakness. The primary diagnostic method used was syndrome differential diagnosis, and herbal medicine, acupuncture, and moxibustion were the main treatments administered.
Acupuncture has been reported to be an effective treatment for fatigue and general weakness, which are the most common complaints of breast cancer patients 14) . Moxibustion, the second most commonly used treatment, is known to be effective in relieving postoperative pain in breast cancer patients 16) . According to Hajime, herbal medicine has been reported to be effective against breast cancer, as well as pain 13) .
In total, 238 (73.9%) of the respondents had never treated breast cancer patients at medical institutions . The reasons for not treating such patients were their infrequent visits and the lack of information and evidence about this disease. Most respondents agreed that there was a need for CPGs and reported that they would adhere to them when they were available.
CPGs for the supportive care of breast cancer patients are being implemented worldwide. In the United States, the
National Comprehensive Cancer Network (NCCN) has published guidelines for breast cancer 17) . In Korea, the third set of guidelines for breast cancer were presented at the 2008 Korean Breast Cancer Society 18) .
Practitioners of alternative medicine are also developing CPGs for breast cancer.
According to the CPGs on the Use of Integrative Therapies as Supportive Care in Patients Treated for Breast Cancer, electro-acupuncture is a grade B approach (should be considered) for nausea and vomiting and a grade C approach (may be considered) for anxiety/stress, depression, fatigue, pain, and burning sensations due to chemotherapy 9) . In 2014, CPGs for breast cancer were presented to the Chinese Association of Integrative Medicine. To improve the treatment rate, the CPGs combined traditional Western medical treatment with Oriental medicine approaches 19) . In addition to alleviating symptoms, several herbal medicines have been found to inhibit the proliferation of breast cancer cells 20,21) . Previous studies have shown a 2.2-fold increase in the incidence of endometrial cancer in patients taking tamoxifen for 5 years, and that patients with tamoxifen and herbal remedies have a lower incidence of endometrial cancer 22) .
Nevertheless, KM is rarely recommended
to patients in Korea 23) . A study of the
perceptions of female cancer patients' found
that non-Western treatment approaches
were not used because patients sought
“to follow the opinion of a Western medical doctor" (71.3%), did “not know the content [of this modality]" (14.9%) 24) . According to a focus group study, supplementary treatment with alternative medicine was not sought due to its unconditional rejection by Western clinicians and their lack of communication 25) .
In a survey of 160 breast cancer patients, 79.6% reported that they had combined complementary alternative therapy with hospital treatment. Nonetheless, 67.3%
of patients reported that they did not consult with their doctor about such alternative treatments. Of this group, 40.7% explained their lack of consultation in terms of their doctor's negative attitudes and indifference 26) .
This situation may be attributable to the absence of current CPGs. If reasonable guidelines were developed, Western medical doctors could change their minds, which would improve breast cancer treatment.
It is important to investigate the current status of KMDs. However, the response rate in this study was low, at 1.76%. The reason for the low response rate was the short survey period (10 days) and the small number of KMDs who were actually treating breast cancer patients. Because more than 70% of the
respondents are aged between 30 and 50, the ratio of physicians with more than 20 years of clinical experience is relatively low and this is considered to be the limitation of this study
Most of the KMDs (74%) who responded to the survey did not treat breast cancer patients at their medical institutions.
This can also be viewed as reflective of the need for CPGs for the supportive care of breast cancer patients. According to our questionnaire results, the development of CPGs was seen as the most important way to improve medical treatment for breast cancer. Moreover, respondents reported that they would actively adhere to such guidelines if they were implemented.
Ⅴ. Conclusion
This survey determined the proportion of KMDs who treat breast cancer patients, and underscored the need for CPGs for using KM to provide supportive care to breast cancer patients and inform both clinicians and patients of the benefits of this approach.
□ Received : Sep 22, 2018
□ Revised : Nov 01, 2018
□ Accepted : Nov 26, 2018
국 문초록
목 적: 한의사의 유방암 보완치료에 대한 실태를 조사하고 임상진료지침의 필 요성을 알아보고자 본 연구를 시행하였습니다.
방 법: 본 연구는 e mail 설문지를 사용하였으며 유방암 환자 치료 여부, 내원 환자들의 병기, 증상, 진단, 치료, 기타 의견 등을 설문하였습니다.
결 과: 322명이 응답하였으며 그 중 84명이 해당 기관에서 유방암 치료를 시행 하고 있었습니다. 내원 환자들의 주된 호소는 피로 및 전신 소력감이었고 변증 및 맥진을 주된 진단법으로 한약 및 침뜸을 중심으로 치료하고 있다고 응답하였습니 다. 유방암의 한의학적 보완치료로서 임상진료지침이 필요하다고 생각하며 개발된 다면 적극적으로 사용하겠다고 응답하였습니다.
결 론: 유방암 보완치료 실태조사를 통해 임상진료지침에 대한 필요성을 알 수 있었으며 추가적인 연구가 필요합니다.
중심단어: 유방암, 보완치료, 단면연구, 임상진료지침, 한의학
References
1. Schwartz R, Erban J. Timing of Metastasis in Breast Cancer. N Engl J Med. 2017;376(25):2486-8.
2. Lee YK, Kim JW, Kang SB. Management of breast cancer survivors in gynecologic area. J Korean Obstet Gynecol. 2007;
50(6):821-30.
3. National Cancer Center Korea Central Cancer Registry. Annual report of cancer statistics in Korea in 2014. Ministry of Health and Welfare. 2016.
4. Oh CM, et al. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2013. Cancer Res Treat. 2016;48(2):436-50.
5. Seo JY, Yi MS. Distress and Quality of Life in Cancer Patients Receiving Chemotherapy. Asian Oncology Nursing.
2015;15(1):18-27.
6. Jo HC, Kim ET, Min JW. Distress and Quality of Life for Breast Cancer Survivors during Follow-Up Periods in Korea. Journal of Breast Disease.
2016;4(2):58-63.
7. Yurek D, Farra W, Andersen B. Breast Cancer Surgery: Comparing Surgical Groups and Determining Individual Differences in Postoperative Sexuality and Body Change Stress. J Consult Clin Psychol. 2000;68(4):697-709.
8. Mourits M, et al. Tamoxifen treatment and gynecologic side effects: A review.
Obstetrics and Gynecology. 2001;97(5(2)) :855-66.
9. Greenlee H, et al. Clinical practice
guidelines on the use of integrative
therapies as supportive care in patients
treated for breast cancer. J Natl
Cancer Inst Monogr. 2014;50:346-58.
10. Horneber M, et al. How many cancer patients use complementary and alternative medicine: a systematic review and metaanalysis. Integrative Cancer Therapies. 2012;11(3):187-203.
11. Choi YJ, Lee JS, Cho SH. Use of Korean Medicine among Cancer Patients. Journal of Korean Oriental Medicine. 2012;33(9):46-53.
12. Kim MJ, et al. Use of Complementary and Alternative Medicine among Korean Cancer patients. The Korean Journal of Internal Medicine. 2004;19(4):250-6.
13. Abe H, et al. The Kampo Medicine Goshajinkigan Prevents Neuropathy in Breast Cancer Patients Treated with Docetaxel. Asian Pacific Journal of Cancer Prevention. 2013;14(11):6351-6.
14. Smith C, et al. The effect of acupuncture on post-cancer fatigue and well-being for women recovering from breast cancer: a pilot randomised controlled trial. Acupunct Med. 2013;31(1):9-15.
15. Yao C, et al. Effects of warm acupuncture on breast cancer-related chronic lymphedema: a randomized controlled trial. Curr Oncol. 2016;23(1):e27-34.
16. Tao J, et al. Clinical Research on the Effect of Thunder Fire Moxibustion Combined with Air Wave Pressure in Treating Limb Edema After Breast Cancer Operation. Clinical Medical
& Engineering. 2015;22(9):1141-3.
17. William J, et al. NCCN Guidelines Insights Breast Cancer, Version 1. 2017.
J Natl Compr Canc Netw. 2017;15(4) :433-51.
18. Korea Breast Cancer Society. Korea Breast Cancer Society Practice Recommendations of Breast Cancer 2008(cited Mar 1, 2016). Available from:URL:http://
guideline.or.kr/guideline/guide/conten ts.php?number=27&F_sid=660.
19. Li X, et al. Traditional Chinese medicine in cancer care: a review of controlled clinical studies published in chinese.
PLoS One. 2013;8(4):e60338.
20. Seo KJ, et al. Effects of Taraxaci Herba on Cell Death in Breast Cancer Cells.
The Journal of Korean Obstetrics and Gynecology. 2015;28(2):1-14.
21. Song YR, et al. Effects of Trogopterorum Faeces on the Apoptostic Cell Death in Breast Cancer Cells. The Journal of Korean Obstetrics and Gynecology.
2015;28(1):46-57.
22. Tsai YT, Lai JN, Wu CT. The use of Chinese herbal products and its influence on tamoxifen induced endometrial cancer risk among female breast cancer patients: a population-based study.
J Ethnopharmacol. 2014;155(2):1256-62.
23. Kim JW. Complementary therapies and cancer treatment, Journal of Korean Medical Association. 2008;51(5):427-34.
24. Moon HW. A Study on the Use of the Complementary and Alternative Therapy in Female Cancer Patients.
Yosong Kongang. 2004;5(2):19-44.
25. Han SA, et al. Experiences of Treatment-
Related Side Effects and Supportive
Care with Korean Medicine in Women
with Breast Cancer - A Focus Group
Study. The Journal of Korean Obstetrics
and Gynecology. 2017;30(1):85-94.
26. Chung HJ, et al. Complementary and Alternative Medicine in Patients with
Breast Cancer. Journal of Breast Cancer.
2006;9(4):361-6.
<별첨. #online questionnaire>