INTRODUCTION
Mitochondrial disease (MD) is a hereditary or sporadic multi-systemic disorder resulting from the impairment of mitochon-drial energy metabolism in the respiratory chain complex of the mitochondrial inner membrane.1,2 The heart is one of the most commonly affected organs, because the myocardium requires a high level of oxygen metabolism to supply blood and energy substrates.1-3 In addition, mitochondria have a
signifi-cant role in the energy production of cardiac cellular biogenic arrangements. Energy supplied in the form of adenosine tri-phosphate (ATP) is essential in sustaining cardiac contractility and relaxation functions.
MD can result in structural heart lesions, which may affect the myocardium, coronary arteries, pericardium, or aortic root. Cardiovascular functional abnormalities can also occur, includ-ing impulse generation, conduction abnormalities, systolic dysfunction, heart failure, pulmonary hypertension, and auto-nomic dysfunction.1 The most frequent cardiovascular mani-festation is cardiomyopathy (CMP), which presents as hypertro-phic CMP (HCMP), dilated CMP, restrictive CMP, or unclassified CMP resembling left ventricular hypertrabeculation or non-compaction. Myocardial fibrosis and late enhancement are also present in other cardiomyopathies.1-3
Children and infants with MD have different clinical pre-sentations to people with adult-onset MD. In children and in-fants, MD is often correlated with genetic defects. The pheno-types of patients with pediatric MD are much more severe, often involving the brain and multi-systemic disorders, but seldom Received: July 5, 2017 Revised: August 19, 2017
Accepted: August 31, 2017
Corresponding author: Dr. Young-Mock Lee, Department of Pediatrics, Gangnam Severance Hospital, Yonsei University College of Medicine, 211 Eonju-ro, Gang-nam-gu, Seoul 06273, Korea.
Tel: 82-2-2019-3350, Fax: 82-2-3461-9473, E-mail: [email protected] •The authors have no financial conflicts of interest.
© Copyright: Yonsei University College of Medicine 2018
This is an Open Access article distributed under the terms of the Creative Com-mons Attribution Non-Commercial License (http://creativecomCom-mons.org/licenses/ by-nc/4.0) which permits unrestricted non-commercial use, distribution, and repro-duction in any medium, provided the original work is properly cited.
Myocardial Layer-Specific Strain Analysis in Children
with Mitochondrial Disease
Lucy Youngmin Eun
1and Young-Mock Lee
2Divisions of 1PediatricCardiology and 2PediatricNeurology, Department of Pediatrics, Gangnam Severance Hospital,
Yonsei University College of Medicine, Seoul, Korea.
Purpose: Children with mitochondrial disease (MD) have clinical phenotypes that are more severe than those found in adults. In this study, we assessed cardiac function in children with MD using conventional and advanced echocardiographic measurements, explored any unique patterns present, and investigated the development of early cardiomyopathy (CMP).
Materials and Methods: We retrospectively reviewed the medical records of 33 children with MD. All patients underwent trans-thoracic echocardiography with conventional and advanced myocardial analysis. We compared all data between patients and an age-matched healthy control group.
Results: Conventional echocardiographic diastolic measurements of mitral E, E/A, and tissue Doppler E’ were significantly lower and E/E’ was significantly higher in children with MD, compared with the measurements from the control group. There was no significant difference in longitudinal and radial strain between the groups. Circumferential strain in the endocardium (p=0.161), middle myocardium (p=0.008), and epicardium (p=0.042) were lower in patients, compared to the values in controls. Circumfer-ential strain was correlated with E’ (p<0.01, r>0.60).
Conclusion: In children with MD, myocardial circumferential strain may develop early in all three layers, even with normally pre-served longitudinal and radial strain. This may be an early diagnostic indicator with which to predict CMP in this patient population. Key Words: Mitochondrial disease, echocardiography, cardiomyopathy, children, myocardial strain
pISSN: 0513-5796 · eISSN: 1976-2437 Yonsei Med J 2018 Jan;59(1):128-134
isolated myopathy. The frequency of cardiovascular involve-ment may differ between children and adults.
With the above in mind, the purpose of this study was to in-vestigate cardiovascular function in children with MD, to as-sess conventional and advanced echocardiographic data, to distinguish unique myocardial characteristics, and to identify early myocardial deterioration.
MATERIALS AND METHODS
PatientsWe retrospectively reviewed the medical records of 33 children with MD who were treated at Gangnam Severance Hospital between March 2013 and June 2014. An equal number of heal-thy, age-matched children were enrolled to serve as a control group.
All patients with MD satisfying the modified MD criteria proposed by Bernier, et al.4 were enrolled; mitochondrial respi-ratory chain complex defects were confirmed via muscle tissue biochemical enzyme assay. The mitochondrial enzyme func-tion of isolated mitochondria was assessed using a standard spectrophotometric assay as described by Rustin, et al.5 Nico-tinamide adenine dinucleotide, coenzyme Q (CoQ) reductase (complex I), CoQ reductase (complex II), succinate-cytochrome c reductase (complex II–III), succinate-cytochrome c reduc-tase (complex III), cytochrome c oxidase (complex IV), oligo-mycin-sensitive ATPase (complex V), and citrate synthase activity were also evaluated. Patients were diagnosed with mi-tochondrial respiratory chain complex defects when the resid-ual enzyme activity was <20% of that in the age-matched con-trol group.
The demographic characteristics of patients were collected from their medical records. The control group of children com-prised those from echocardiographic referral for precordial cardiac murmur, an enlarged cardiothymic silhouette in a chest radiogram, or an incomplete right bundle branch block pat-tern on an electrocardiogram. Children with any acute illness by history and physical examination, congenital or acquired heart disease, syndromes, or chromosomal abnormalities were ex-cluded.
All study participants underwent transthoracic echocardiog-raphy. All procedures were approved by the Institutional Re-view Board of Gangnam Severance Hospital in Seoul, Korea (3-2017-0168). Informed consent was obtained and all meth-ods were performed in accordance with the relevant guidelines and ethics board regulations.
Echocardiography and strain analysis
Conventional echocardiographic measurements and advanced myocardial imaging studies were performed by an expert pe-diatric cardiologist in both groups using a Siemens ACUSON SC2000 system (Siemens Medical Solutions USA, Inc.,
Moun-tain View, CA, USA). Echocardiography was performed in the left lateral decubitus or supine position to obtain two-dimen-sional, M-mode, and Doppler measurements of the paraster-nal long-axis view, short-axis view, and four-chamber view, respectively. Maximal left ventricular wall thickness was de-fined as the largest thickness in any single segment, mainly in the parasternal short-axis view. The mean value of more than three measurements obtained using echocardiography was entered into analysis.
Advanced tissue speckle images were recorded at a rate of >50 frames/s to investigate myocardial strain and the rate thereof. Two-dimensional images of the apical four-chamber view were recorded to assess longitudinal strain, while those of the parasternal short-axis view were acquired to assess ra-dial and circumferential strain. An offline speckle tracking pro-cess was conducted with acoustic markers using Syngo Veloc-ity Vector Imaging software (Siemens Medical Solution USA, Inc.). The borders of the endocardium and epicardium were traced manually and the border of the myocardium was defined as the midline between the border of the endocardium and epicardium. These three contours were tracked frame-by-frame throughout the cardiovascular cycle. Patients were diagnosed with myocardial deformation after this tracking process, while simultaneously checking for layer-specific myocardial strain and the respective strain rate of the layers of the endocardium, myocardium, and epicardium.
Statistical analysis
All data and measurements were reported as means±standard deviations. We compared all demographic and echocardiogra-phic data between the two groups using an independent Stu-dent’s t-test. A p-value ≤0.05 was considered statistically sig-nificant with a correlation r-value of ≥0.60 with SPSS 19.0 (IBM Corp., Armonk, NY, USA).
RESULTS
In total, 22 boys and 11 girls with a mean age of 10.3±4.0 years were included in the analysis. The control group included the same number of children (14 boys and 19 girls) with a mean age of 8.4±3.9 years (Table 1). The results of the spectrophotomet-ric biochemical enzyme assays for mitochondrial respiratory chain complexes of the muscle were available in all patients: 66.7% (n=22) of the patients had complex I defects and 33.3% (n=11) had complex IV defects. Among the children with MD, 10 were capable of independent walking, eight were wheel-chair-bound, and 15 were bed ridden.
The conventional echocardiographic measurements of left ventricular ejection fraction were similar between the two groups [MD, 65.8±9.8%; control, 65.9±4.2%; p=not significant (ns)]. The results of fractional shortening were also similar be-tween groups (MD, 35.6±6.3%; control, 36.3±3.2%; p=ns).
Pa-tients with MD had greater interventricular septal and left ven-tricular posterior wall thickness during diastole and systole than patients in the control group. However, this difference was not statistically significant (p=ns) (Table 2).
The conventional mitral inflow E, E/A, tissue Doppler dia-stolic E' were significantly lower, and E/E' was higher in the MD group than those in the control group (p<0.05) (Table 2). These diastolic parameters did not correlate with wall thick-ness in this study.
We noted no difference in longitudinal strain in the apical four-chamber view between the two groups in all layers of the
endocardium, myocardium, and epicardium. Strain rate was not significantly different between the two groups in the apical four-chamber view (Table 3).
Radial strain measured in the parasternal short-axis view was not statistically different between the groups (MD, 37.17±11.1%; control, 37.73±25.9%; p=0.924). Similarly, the radial strain rate was not significantly different between the groups (MD, 2.26± 0.91; control, 2.44±0.84; p=0.562).
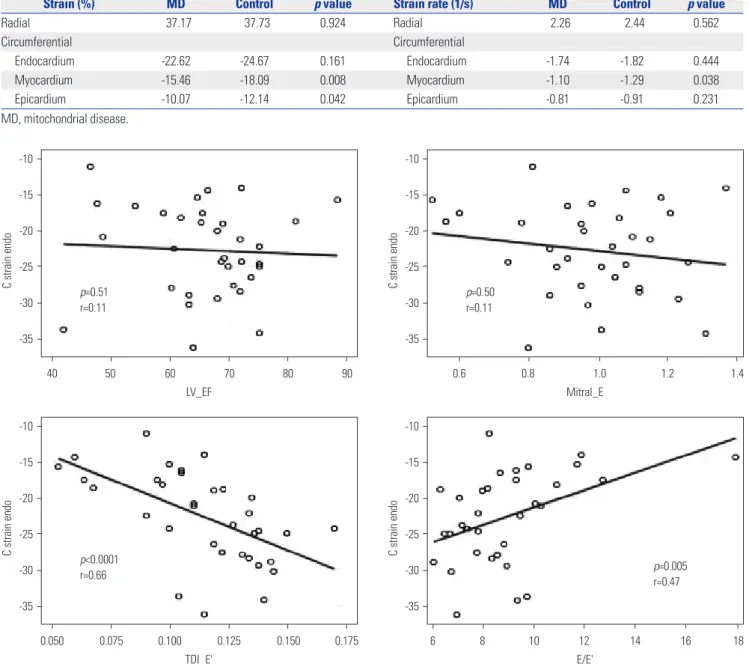
Circumferential strain in the endocardium (-22.62±4.7% vs. -24.67±5.3%; p=0.161), myocardium (-15.46±3.8% vs. -18.09± 4.0%; p=0.008), and epicardium (-10.07±4.0% vs. -12.14±5.0%; p=0.042) was lower in patients with MD than in healthy pa-tients. Circumferential strain rate of the myocardium was also lower in the MD group (-1.10±0.27) than that in the control group (-1.29±0.22) (p=0.038). The strain rate was lower in the endocardium (-1.74±0.38 vs. -1.82±0.27; p=0.444) and epicar-dium (-0.81±0.38 vs. -0.91±0.27, p=0.231) of patients in the MD group than in patients in the control group, although the dif-ference was not statistically significant (Table 4). Interestingly, the decreased circumferential strain of the endocardium, myo-cardium, and epicardium in patients with MD correlated well with the tissue Doppler peak velocities of E’ (Figs. 1, 2, and 3).
When these results were considered together, we found that the conventional echocardiographic diastolic values of mitral E, E/A, and tissue Doppler E’ were significantly lower in chil-dren with MD than those in healthy chilchil-dren. In contrast, E/E’ was significantly higher in children with MD than that in he-althy children. The advanced myocardial analysis revealed no significant differences in longitudinal and radial strain be-tween the two study groups; however, the circumferential strain in patients with MD was significantly lower in the myocardium and epicardium. In addition, the circumferential strain in all three layers correlated with tissue Doppler E’.
DISCUSSION
Hundreds of different pathogenic mitochondrial DNA muta-tions have been reported in humans, many of which are asso-ciated with various cardiovascular diseases. This wide range of disease expression and the lack of a specific cardiovascular phenotype distinctive to patients with MD presents a challenge for cardiologists, especially in pediatric patients.6 According to previously published studies, cardiac involvement was re-Table 1. Baseline Patient Characteristics
MD (n=33) Control (n=33) p value
Sex (M:F) 22:11 14:19
Age (year) 10.3±4.0 8.4±3.9 0.069 Weight (kg) 30.0±12.7 30.0±16.6 0.531 MD, mitochondrial disease.
Table 2. Comparison of Echocardiographic Measurements between the Groups MD (n=33) Control (n=33) p value LV EF (%) 65.94±8.05 65.79±4.02 0.899 LV FS (%) 36.31±7.35 35.62±3.06 0.620 IVSTd (mm) 7.75±3.25 6.91±1.56 0.192 IVSTs (mm) 9.97±3.42 8.98±1.81 0.153 LVIDd (mm) 36.06±6.92 37.83±5.86 0.277 LVIDs (mm) 23.15±5.80 24.34±3.92 0.353 LV PWTd (mm) 6.06±2.09 5.63±1.57 0.364 LV PWTs (mm) 9.20±2.88 8.68±1.51 0.048 Mitral E (m/s) 0.98±0.20 1.08±0.16 0.029 Mitral A (m/s) 0.61±0.20 0.54±0.11 0.074 Mitral E/A 1.77±0.69 2.09±0.45 0.041 TDI E' (m/s) 0.11±0.03 0.14±0.02 <0.001 TDI A' (m/s) 0.08±0.11 0.05±0.02 0.230 TDI S' (m/s) 0.06±0.01 0.09±0.10 0.086 E/E' 8.88±2.26 7.62±1.64 0.0007 MD, mitochondrial disease; LV, left ventricle; EF, ejection fraction; FS, frac-tional shortening; IVSTd, interventricular septal thickness, diastole; IVSTs, in-terventricular septal thickness, systole; LVIDd, left ventricle internal diameter, diastole; LVIDs, left ventricle internal diameter, systole; PWTd, posterior wall thickness, diastole; PWTs, posterior wall thickness, systole; E, peak early mi-tral inflow velocity; A, peak late mimi-tral inflow velocity; TDI, tissue Doppler imaging; E’, peak early diastolic septal annulus velocity; A’, peak late diastol-ic septal annulus velocity; S’, peak systoldiastol-ic septal annulus velocity.
Table 3. Strain and Strain Rate in the Apical Four-Chamber View
Strain (%) MD Control p value Strain rate (1/s) MD Control p value
Radial 23.53 23.15 0.941 Radial 2.22 2.18 0.855 Longitudinal Longitudinal Endocardium -18.83 -17.64 0.377 Endocardium -1.40 -1.25 0.313 Myocardium -15.50 -12.93 0.165 Myocardium -1.09 -1.00 0.220 Epicardium -12.23 -12.71 0.613 Epicardium -0.86 -0.85 0.768 MD, mitochondrial disease.
ported in 33% of pediatric patients with MD, while CMP was present in approximately 5.6% of children with MD.1,7,8
Among the different types of CMP, HCMP is the most fre-quently observed in patients with MD.1,9,10 Cardiac hypertro-phy is an adaptive response to the increased work load induced by physiological or pathological stimuli to counteract the in-creased wall tension and to maintain cardiac output.11 When the heart is extremely stressed with persistent overload, the result-ing hypertrophy may become maladaptive, and cardiac func-tion may progressively deteriorate, resulting in heart failure.12
Primary mitochondrial cardiomyopathies lead to mitochon-drial proliferation in cardiomyocytes.13 In addition, pathologi-cal cardiac hypertrophy that develops due to increasing num-bers of mitochondria results in the enhancement of
mitochon-drial biogenesis and protein synthesis.14 To our knowledge, however, the implications of mitochondrial biogenesis in CMP have not been clarified. Furthermore, the hypertrophic phase induced in CMP that naturally accompanies increased mito-chondrial biogenesis seems to delay the cardiac decompensa-tion caused by pressure overload.15
Other experimental studies have reported the cardiovascu-lar effects of prediabetes in patients with MD, indicating that mild diastolic dysfunction and cardiovascular hypertrophy are multifactorial phenomena associated with early changes in mi-tophagy, cardiac lipid accumulation, and elevated oxidative stress.16 Prediabetes-induced oxidative stress was also shown to originate from the subsarcolemmal mitochondria.16
Severe and rapidly progressive dilated CMP has been shown Table 4. Strain and Strain Rate in the Parasternal Short-Axis View
Strain (%) MD Control p value Strain rate (1/s) MD Control p value
Radial 37.17 37.73 0.924 Radial 2.26 2.44 0.562 Circumferential Circumferential Endocardium -22.62 -24.67 0.161 Endocardium -1.74 -1.82 0.444 Myocardium -15.46 -18.09 0.008 Myocardium -1.10 -1.29 0.038 Epicardium -10.07 -12.14 0.042 Epicardium -0.81 -0.91 0.231 MD, mitochondrial disease.
Fig. 1. Correlation of circumferential strain of the endocardial layer with conventional and tissue Doppler parameters.
-10 -15 -20 -25 -30 -35 -10 -15 -20 -25 -30 -35 -10 -15 -20 -25 -30 -35 -10 -15 -20 -25 -30 -35 40 0.050 0.075 0.100 0.125 0.150 0.175 0.6 6 60 1.0 10 12 80 1.2 16 50 0.8 8 70 14 90 1.4 18 LV_EF TDI_E' Mitral_E E/E' C strain endo C strain endo C strain endo C strain endo p=0.51 r=0.11 p<0.0001 r=0.66 p=0.50 r=0.11 p=0.005 r=0.47
to occur if the hypertrophic phase is bypassed.17 Since cardio-vascular systolic and diastolic function is dependent on mito-chondrial ATP, it is possible that a decline in mitomito-chondrial bio-genesis contributes to the progression of CMP and heart failure, leading to sudden cardiovascular death.
Many questions still remain to be answered, however. The reason why CMP is the most common form of cardiac involve-ment in MD may be due to the close relationship between myocardial function and mitochondrial energy supply. Addi-tionally, the similarities between skeletal muscle and the myo-cardium may play a role, with the former being the most fre-quently affected organ due to its need for constant energy supply and the latter being the tissue with potentially the great-est energy requirement.1 HCMP is most prevalent in children with MD and develops even without the presence of systolic dysfunction or heart failure.8
In the present study, we identified an increase in the left ven-tricular posterior wall and intervenven-tricular septal thickness, which may indicate the beginning of myocardial hypertrophy preceding HCMP. Furthermore, the diastolic measurement of mitral inflow, E, E/A, tissue Doppler E’, and E/E’ were all sig-nificantly different, suggesting that statistically significant dia-stolic dysfunction had already developed. This diadia-stolic
dete-rioration certainly seems to have preceded the hypertrophic change of the myocardium. The decline of diastolic function could represent the beginning of real myocardial deterioration. Pathological hypertrophy may then progress in the interven-tricular septum and veninterven-tricular posterior free wall along with mitochondrial biogenesis to overcome the persistent lack of sufficient energy to meet the workload demanded.
To diagnose patients with early cardiac deterioration, diverse echocardiographic techniques should be used in patients with MD, along with conventional and advanced myocardial imag-ing studies. Myocardial layer-specific strain analysis is a feasi-ble and reproducifeasi-ble method to assess subtle myocardial de-terioration.18 However, to our knowledge, it has rarely been used in children. In this study, children with MD demonstrated decreased diastolic parameters, compared to those in healthy controls. We also tried to perform layer-specific myocardial analysis of the endocardium, myocardium, and epicardium in this patient population for the first time. Interestingly, we ob-served circumferential strain deterioration in the myocardium and epicardium despite preserved longitudinal and radial strain with normal left ventricular ejection fraction.
Earlier deterioration of circumferential strain may be due to the configuration of left ventricular myofibril derangement in Fig. 2. Correlation of circumferential strain of the middle myocardial layer with conventional and tissue Doppler parameters.
-10 -15 -20 -10 -15 -20 -10 -15 -20 -10 -15 -20 40 0.050 0.075 0.100 0.125 0.150 0.175 0.6 6 60 1.0 10 12 80 1.2 16 50 0.8 8 70 14 90 1.4 18 LV_EF TDI_E' Mitral_E E/E' C strain myo C strain myo C strain myo C strain myo p=0.25 r=0.20 p<0.0001 r=0.70 p=0.39 r=0.15 p=0.003 r=0.49
patients with MD. As myocardial fiber arrangement is impor-tant for electrical propagation and myocardial contraction, once subtle myofibril dysfunction develops, the conduction problem would be unavoidable. Moreover, myofibril dysfunc-tion is the obvious cause for further contractile dysfuncdysfunc-tion. In other words, decreased circumferential strain could serve as an early sign of myocardial dysfunction before it is severe en-ough to produce clinical detectable changes and while other conventional systolic parameters are still within reasonable ranges. Therefore, circumferential strain can be a sensitive in-dicator of myocardial deterioration before the development of myocardial fibrosis and the subsequent loss of myocytes.
Among the three layers of the myocardium, we recognized that, in terms of order and severity, circumferential strain al-teration started from the mid-myocardial layer and progressed to the epicardial layer. The endocardial layer may be less dete-riorated or relatively preserved in terms of functional decline, compared with the middle myocardium and epicardium. This could indeed be a promising valuable discovery in relation to myocardial assessment in pediatric patients with MD. Further-more, circumferential strain in all three layers correlated well
with early diastolic tissue Doppler velocity of E’, which may im-ply systolic and diastolic coupling in these children.
The goal of cardiovascular treatment is to decelerate the de-terioration of myocardial function with appropriate drugs to al-low a better quality of life, regardless of systemic multi-organ involvement. Even in patients showing values in the normal ranges for various parameters of conventional echocardiogra-phy, advanced detailed functional indicators, such as strain measurements, may help to recognize early signs of dysfunc-tion, as demonstrated in this study.
Myocardial strain analysis of the respective cardiac layers is certainly a promising tool with which to detect subtle myocar-dial deterioration before any noticeable decline of cardiac func-tion occurs, aiding in determining when to proceed with suit-able cardiac treatment. It could undoubtedly play a role in the enhancement of cardiac function and thus improve prognosis with respect to growth and development in children with MD. The limitation of this study is a small sample size of the rare disease children with MD. Further studies are needed to pro-vide a better and more comprehensive investigation.
In conclusion, children with MD may have earlier myocar-Fig. 3. Correlation of circumferential strain of the epicardial layer with conventional and tissue Doppler parameters.
-5.0 -7.5 -10.0 -12.5 -15.0 40 50 60 70 80 90 LV_EF C strain epi p=0.16 r=0.24 -5.0 -7.5 -10.0 -12.5 -15.0 0.050 0.075 0.100 0.125 0.150 0.175 TDI_E' C strain epi p<0.0001 r=0.63 -5.0 -7.5 -10.0 -12.5 -15.0 0.6 0.8 1.0 1.2 1.4 Mitral_E C strain epi p=0.32 r=0.17 -5.0 -7.5 -10.0 -12.5 -15.0 6 8 10 12 14 16 18 E/E' C strain epi p=0.006 r=0.46
dial deterioration in circumferential strain, especially of the middle myocardial and epicardial layers, even with well-pre-served longitudinal function. This knowledge could be used as an early diagnostic indicator of myocardial involvement, aid-ing in diagnosis and allowaid-ing for timely treatment of CMP.
ORCID
Lucy Youngmin Eun https://orcid.org/0000-0002-4577-3168
Young-Mock Lee https://orcid.org/0000-0002-5838-249X
REFERENCES
1. Finsterer J, Kothari S. Cardiac manifestations of primary mito-chondrial disorders. Int J Cardiol 2014;177:754-63.
2. DiMauro S, Schon EA, Carelli V, Hirano M. The clinical maze of mitochondrial neurology. Nat Rev Neurol 2013;9:429-44. 3. Meyers DE, Basha H, Koenig MK. Mitochondrial
cardiomyopa-thy: pathophysiology, diagnosis, and management. Tex Heart Inst J 2013;40:385-94.
4. Bernier FP, Boneh A, Dennett X, Chow CW, Cleary MA, Thorburn DR. Diagnostic criteria for respiratory chain disorders in adults and children. Neurology 2002;59:1406-11.
5. Rustin P, Chretien D, Bourgeron T, Gérard B, Rötig A, Saudubray JM, et al. Biochemical and molecular investigations in respiratory chain deficiencies. Clin Chim Acta 1994;228:35-51.
6. Bates MG, Bourke JP, Giordano C, d’Amati G, Turnbull DM, Taylor RW. Cardiac involvement in mitochondrial DNA disease: clinical spectrum, diagnosis, and management. Eur Heart J 2012;33:3023-33. 7. Yaplito-Lee J, Weintraub R, Jamsen K, Chow CW, Thorburn DR, Boneh A. Cardiac manifestations in oxidative phosphorylation disorders of childhood. J Pediatr 2007;150:407-11.
8. Yilmaz A, Gdynia HJ, Ponfick M, Rösch S, Lindner A, Ludolph AC, et al. Cardiovascular magnetic resonance imaging (CMR) reveals characteristic pattern of myocardial damage in patients with
mi-tochondrial myopathy. Clin Res Cardiol 2012;101:255-61. 9. Bates MG, Nesbitt V, Kirk R, He L, Blakely EL, Alston CL, et al.
Mi-tochondrial respiratory chain disease in children undergoing car-diac transplantation: a prospective study. Int J Cardiol 2012;155: 305-6.
10. Lev D, Nissenkorn A, Leshinsky-Silver E, Sadeh M, Zeharia A, Garty BZ, et al. Clinical presentations of mitochondrial cardiomy-opathies. Pediatr Cardiol 2004;25:443-50.
11. Zhou LY, Liu JP, Wang K, Gao J, Ding SL, Jiao JQ, et al. Mitochon-drial function in cardiac hypertrophy. Int J Cardiol 2013;167:1118-25. 12. Osterholt M, Nguyen TD, Schwarzer M, Doenst T. Alterations in
mitochondrial function in cardiac hypertrophy and heart failure. Heart Fail Rev 2013;18:645-56.
13. Sebastiani M, Giordano C, Nediani C, Travaglini C, Borchi E, Zani M, et al. Induction of mitochondrial biogenesis is a maladaptive mechanism in mitochondrial cardiomyopathies. J Am Coll Cardi-ol 2007;50:1362-9.
14. Asayama K, Dobashi K, Hayashibe H, Megata Y, Kato K. Lipid peroxidation and free radical scavengers in thyroid dysfunction in the rat: a possible mechanism of injury to heart and skeletal muscle in hyperthyroidism. Endocrinology 1987;121:2112-8.
15. Rosca MG, Tandler B, Hoppel CL. Mitochondria in cardiac hyper-trophy and heart failure. J Mol Cell Cardiol 2013;55:31-41. 16. Koncsos G, Varga ZV, Baranyai T, Boengler K, Rohrbach S, Li L, et
al. Diastolic dysfunction in prediabetic male rats: role of mito-chondrial oxidative stress. Am J Physiol Heart Circ Physiol 2016; 311:H927-43.
17. Shende P, Plaisance I, Morandi C, Pellieux C, Berthonneche C, Zorzato F, et al. Cardiac raptor ablation impairs adaptive hypertro-phy, alters metabolic gene expression, and causes heart failure in mice. Circulation 2011;123:1073-82.
18. Williams LK, Urbano-Moral JA, Rowin EJ, Jamorski M, Bruchal-Garbicz B, Carasso S, et al. Velocity vector imaging in the measure-ment of left ventricular myocardial mechanics on cardiac magnetic resonance imaging: correlations with echocardiographically de-rived strain values. J Am Soc Echocardiogr 2013;26:1153-62.