Prediction for risk of ischemic heart disease (IHD) in aged 30 or older Korean using national health insurance
service-national sample cohort (NHIS-NSC)
Hyemin Wang 1 · Sungsuk Chung 2
1 Department of Statistics, Chonbuk National University
2 Department of Statistics (Institute of Applied Statistics), Chonbuk National University
Received 1 July 2019, revised 21 August 2019, accepted 1 September 2019
Abstract
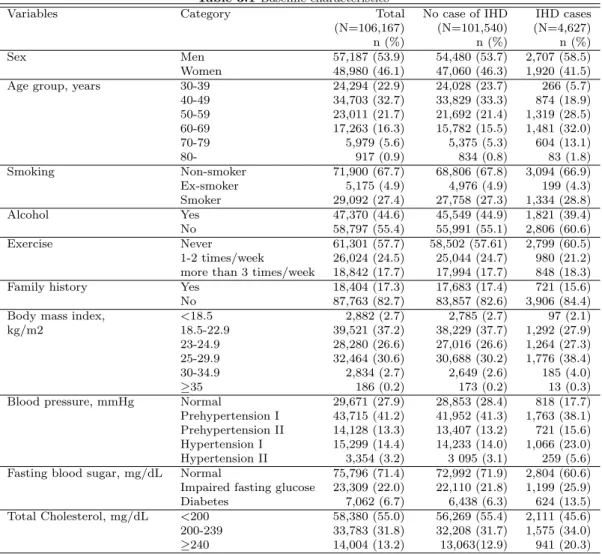
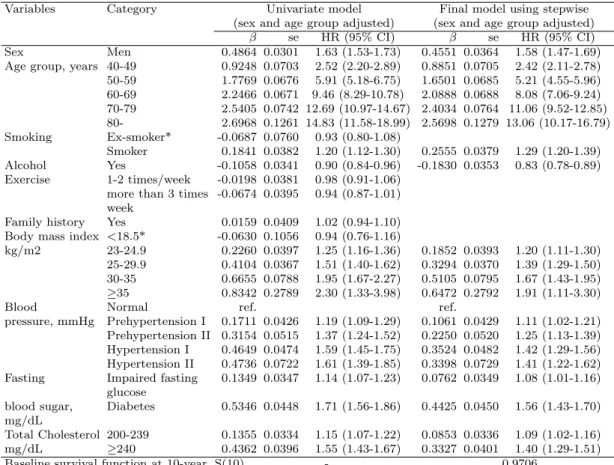
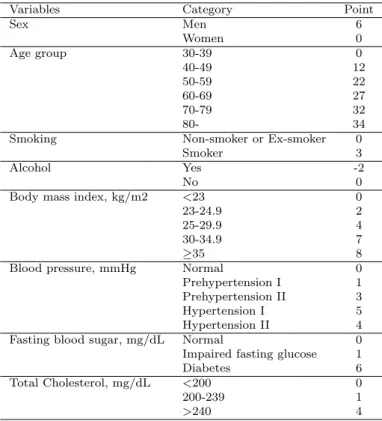
The mortality rate of ischemic heart disease (IHD) was the highest rate of any heart diseases in South Korea. In this study, we predict the absolute risk factors of IHD according to individual characteristics or health status. Cox proportional hazards regression models were fitted to estimate hazard ratio of risk. Stepwise method was used to select a final model. After predictors were selected, the results were used to estimate the absolute 10-year IHD risk using Framingham risk score function and to calculated a simple point system. The total observation period for 106,167 subjects was 1,071,584 person-years. During the observation period, 4,627 subjects (4.4%) developed IHD with incidence rate of 431.79 per 100,000 person-year. Sex, age, smoking, drink, blood pressure, fasting blood sugar and total cholesterol were included in the final model. A Harrell?s c-index was 0.7321 as a measure of discrimination and the overall O/E ratio was 0.972 (95% CI 0.944-1.000). We have predicted a model for 10-year risk of IHD related to risk factors using NHIS-NSC. Using these results, if you have your health information, you will be able to predict your risk of IHD.
Keywords: Absolute risk factor, Cox proportional hazards regression, Framingham risk score, ischemic heart disease.
1. Introduction
In 2015, the total number of deaths in South Korea was 275,895, and the three leading causes were malignant neoplasms (cancer), heart disease, and cerebrovascular disease. The heart disease was the third leading cause of death 10 years ago, and now it is second only to cancer. The mortality rate of ischemic heart disease (IHD) was 28.9 per 100,000 population, which was the highest rate of any heart diseases (Statistics Korea, 2016). IHD is a commonly caused by atherosclerosis affecting the coronary arteries, which limits the flow of oxygen-rich
1
Ph. D. candidate, Department of Statistics, Chonbuk National University, Jeonju, Jeonbuk 54896, Korea.
2