大 4i~I/;{~‘J*h~~~~ 짜쩍 μ 짜 23 卷 었 6 iJIÆ pp. 1031- 1037, 1987 Journal of Korean Radiological Society, 23(6) 1031-1037, 1987
Effects of Extracorporeal Shock Wave Lithotripsy on the Kidney and Perinephric tissues: CT Evaluation *
Kounn Sik Song, M.D., Kun Sang Kim, M.D., Sae Chul Kim, M.D. * *
Department of Radiology, College of Medicine, Chung-Ang University
〈국문초록〉
n (
체외충격파쇄석술이 신장 및 신주위조직에 미치는 영향*
- 전산화단층찰영소견 -
중앙대학교 의과대 학 방사선파학교실
송 군 식
•김 건 상
•김 세 칠
**
처1외충격파쇄석술은 신장결석 및 요판결석을 수술에 의하지 않고 비침습석으로 제거하는 새로운 치효땅법이다. 충격파가 결석에 도달하려연 연부조직, 신주위조직 및 신실질을 통파하여야 하으로 위의 조직에 기능적 및 형태학적인 변화를 일으킬 가능성이 있으나 현재까지는 보고가 미미한 싶정 이며 결파 또한 일정하지 않마 Domier쇄석기와 같은 electrostatic spark discharge방식에 의 한 충격파의 영향에 판해서는 보고되어 있지만 piezoeJectric crystaJ 에 의한 충격파의 영뺑 대 해서는 보고된 바가 없막 저자들은 piezoelectric crystal에 의한 충격파가 신실질, 신주위 조직 및 연부조직에 미치는 영향을 전산화단충촬영을 이용하여 분석한 결파 다음과 같은 결론을 얻었다.
총 130 명의 환자중 87명(67%)에서 전반적인 신종대의 소견을 보였고 79 영(61 %)의 환자에 서 신주위조직의 증가된 선상음영이냐 Gerota’s fascia가 비후되는 소견을 보였으나 임상석으로 벨마른 치료릎 요하는 증상은 없었다. 또한 5 명(4 %)의 환자에서 신피악하혈종이 관찰되었고 4 영
(3 %)의 환자에서 신실질내혈종이 발견되었으냐 밸마은 치료을 요히순 증상은 없었다. 따라서 저 자들은 체외충격파쇄석숭은 바칩습적으로 비교적 안전하게 신장결석 및 요판결석을 제 거하는 치료 방법이라는 결론을 얻었다.
* 본 논문은 1987 년도 한국방사선의학재단 연쿠바 보조로 이루어진 것임.
** 중앙대학교 의과대학 비뇨기과학교실
* * Department of Urology, College of Medicine, Chung-Arg University
이 논문은 1987 년 10 월 5 일에 접수하여 1987 년 11월 19 일에 채택되었음.
Received October 5, Aecepted November 19, 1987
J、센1;!,:~'Jt있셋작,~{u'ì lt~.: : IT}23정 찌, 6 싸 1987-
Since the first successful treatment of the pa- tient with renal stone by extracorporeal shock wave lithotripsy at the Institute for Surgical Research, West Germany, on February 7,1980, extracorporeal shock wave lithotripsy (ESWL) has been a non-invasive technique for the treat- ment of the renal and ureteral calculi'-4), ln spite of the fact that the acoustic energy of the focused shock waves must pass through the soft tissues of back, perinephric tissues and renal parenchyme before reaching calculi, little is known about the effects of ESWL on the renal parenchyme and perinephric soft tissues, So we analyzed a pre and post-ESWL computed tomography scans of the kidenys in 130 patients treated at our hospital during a three month period to evaluate the effects of ESWL on the kidney and perinephric soft tissues.
Materials and Methods
One hundred thirty patients (106 males and 24 females) treated by ESWL for renal and pro- ximal ureteral stones were evaluated with CT.
The patients ranged in age from 17 to 68 years and mean age were 50 years. Patients with ureteral stones except proximal ureteral stones were excluded from the study for shock waves did not traverse the kidney in patients with mid and distal ureteral stones. ESWL was perform- ed with a second generation lithotripter LT-01 (EDAP, France). EDAP LT-01 extracorporeal lithotripter generates shock waves by multiple piezoelectric crystals and localization of the stones is made by realtime ultrasound sector scanner in which 5MHz probe was pre-set in the middle of the wave generator. Storage of shock waves ranged from 30 to 170 (mean 83), rate from 1.25 to 20/sec (mean 15), duration from 15 to 88 minutes (mean 36 minutes) and power from 33% to 100% (mean 86%) per treat- ment. No patient required general or epidural anesthesia.
CT scans were obtained both before and after treatment in all patients. Pre-ESWL scans were obtained the day of treatment 'and post
ESWL scans the day after treatment. The CT scans were performed with a TCT-80A scan- ner (Toshiba corporation) with contiguous 10mm sections through the kidneys without ad- ministration of contrast media to prevent any unnecessary adverse reactions.
Kidney size was measured along the short axis and long axis at the same level on both pre and post-ESWL scans at the level of center of the stone and renal vein. Presence of hematomas, hydronephrosis and changes of the perinephric tissues, Gerota’s fascia, soft tissues of back were evaluated also (Fig. 1).
X
Fig-. J \r easurement of the size of kidney at the level of [he stone and renal vein along the short axis (AB) and long axis (CD)
Results Kidney
Eighty seven (67%) of the 130 treated kidneys were enlarged by more than 4mm either along the short axis or long axis on the post-ESWL scans. The mean pre-ESWL measurement of the 130 kidneys was 49.2mm (SD 6.4) in short axis and 60.4mm (SD 6.6) in long axis at the level of the stone. At the level of the renal vein mean pre-ESWL measurement was 52.0mm (SD 5.9) in short axis and 63.1mm (SD 7.0) in long axis respectively. The mean post-ESWL measurement of the treated kidneys was 55.4mm (SD 7.5) in short axis and 63.1mm (SD7.0) in long axis at the level of the stone. At the level of the renal vein mean post- - 1032
• Kounn Sik Song, et al.: Effects of Extracorporeal Shock 씨r ave Lithotripsy on the Kidney and Perinephric tissues ESWL measurement was 57.9mm (SD 6.9) in
short axis and 64.4mm (SD 6.2) in long axis respectively. The average increase in renal size was 6.2mm (12.6%) in short axis and 2.7mm (4.5%) in long axis at the level of the stone. At the level of the renal vein average increase in renal size was 5.9mm (11.3%) in short axis and 3.2mm (5.2%) in long axis respectively.
Statistically significant increase of renal size in short axis (P<0.005) and long axis (P<0.05) after ESWL at the level of both stone and renal vein was found. The average increase in kidney size of nine patients with post-ESWL hydronephrosis and five patients with subcap sular hematoma was 17.6% in short axis, 8.9%
in long axis at the level of stone and 16.3% in short axis, 11.0% in long axis at the level of renal vein respectively (Fig. 2).
Discrete high density parenchymal hema tomas were seen in four (3%) patients. 1n one patient it was the only abnormality after ESWL.
1n the other patients it was associated with Gerota’s fascia thickening, Gerota’s fascia thickening with perirenal strands, and subcap sular hematoma, respectively (Fig. 3).
Crescentic shaped high density subcapsular hematomas were seen in five (4%) patients.
Two of the subcapsular hematomas were ex- tensive and three subcapsular hematomas were smal1 in amount. Hemorrhage into a simple cor tical cyst was seen in one patient (0.7%). Focal bulge of renal parenchyme rather than usual diffuse swelling of the kidney were seen in four patients (30/0) (Fig. 4).
Perinephric space
Seventy nine (61%) patients showed high density linear strands within the perinephric soft tissues with associated blurring of the renal margin and Gerota’s fascia thickening. 1n four patients thickening of the Gerota’s fascia was the only post-ESWL abnormalities and in twen- ty one patients perinephric soft tissue strands were the only post-ESWL abnormalities (Fig.
5). Perinephric hematomas were not found.
Adjacent pancreas, liver, spleen, aorta and 1VC, soft tissues of back showed no abnor malities after ESWL.
Table 1 is a summary of the abnormalities found in CT scan after ESWL.
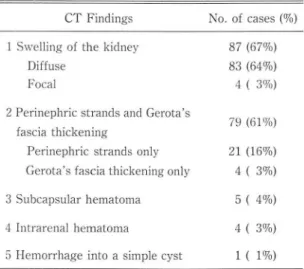
Table 1. CT Findings after ESWL in Treated 130 Kidneys CT Findings
1 Swelling of the kidney Diffuse
Focal
2 Perinephric strands and Gerota’s fascia thickening
Perinephric strands only Gerota’s fascia thickening only 3 Subcaps비ar hematoma
4 Intrarenal hematoma
5 Hemorrhage into a simple cyst
Discussion
No. of cases (%)
87 (67%) 83 (64%) 4 ( 3(70)
79 (61%) 21 (16%)
4 ( 3%) 5 ( 4%)
4 ( 3%) 1 ( 1%)
Extracorporeal shock wave lithotripsy (ESWL) is a relatively new technique for the treatment of the renal and ureteral calculi.
Because of excellent results and non-inva- siveness, ESWL actual1y supplanted classic surgical treatment for nephrolithiasis and is now the primary modality for treatment of nephrolithiasis. Properties of shock waves generated by ESWL causing disintegration of renal and ureteral calculi are, 1) Shock waves exert sufficient mechanical stresses that exceed the tensile strength of brittle stones 2) Shock waves are propagated through the body without energy loss 3) Shock waves can be focused and reproduced reliably. At present many different types of lithotripters are commercially delivered, 1) Generation of shock waves by underwater spark discharge, focusing with semiellipsoidal reflector and localization of stone by fluoroscopy such as Dornier
-大짧放射線챔쩡 *tt 第 23卷 第6 Y!Ii 1987-
A B
C D
E
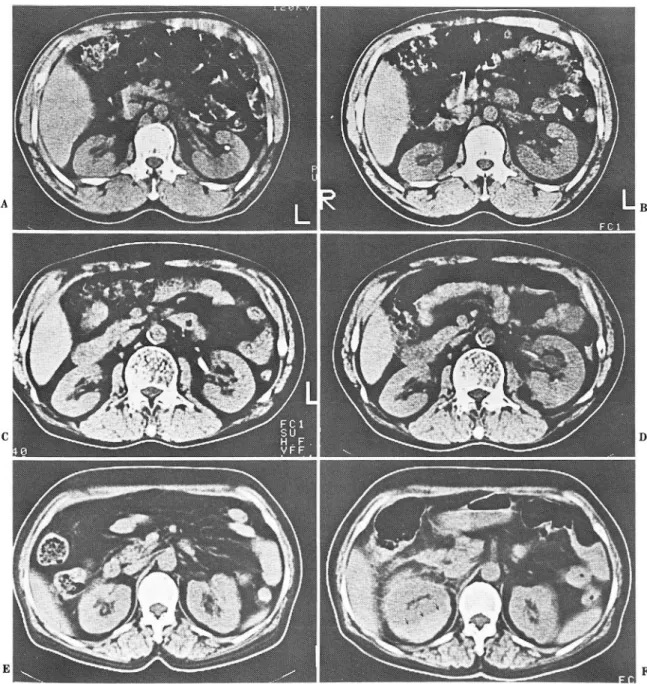
Fig. 2. Renal enlargement after ESWL is due to parenchymal swelling, hydronephrosis and subcapsular hematoma‘
A,B. Renal stone is seen in pre-ESWL scan (A). Diffuse swelling of the left kidney, especially along the short axis, is seen in post-ESWL scan (B). Notice the fragmented stone.
C,D. UPJ stone is seen in pre-ESWL scan(C). More obvious enlargement of the left kidney due to diffuse swell- ing and hydronephrosis is seen in post-ESWL scan (D).
E,F. Enlargement of the right kidney is mainly due to subcapsular hematoma (arrow) in post-ESWL scan Perinephric soft tissue stranding and Gerota’s fascia thickening.
- 1034-
F
- Kounn Sik Song. et al.: Effects of Extracorporeal Shock Wave Lithotripsy on the Kidney and Perinephric tissues
A B
Fig. 3. Intrarenal hematoma
A. Pre.ESWL scan shows small renal stone of the left kidney.
B. Post-ESWL scan shows globular swelling of the left kidney with small and punctate discrete high density hematoma within the renal parenchyme (arrow).
A
C
Fig. 4. Subcapsular hematoma and hemoπhage into a pre-existing simple cyst
A.B. Large stone is seen in the pelvis of right kidney in pre-ESWL scan(A). Stone is fragmented and crescentic shaped high density subcapsular hematoma (arrow) is seen is post-ESWL scan (B)
C.D. Pre-ESWL scan (C) shows renal stones ancl simple renal cyst in lower pole of left kidney. Small amount of high density blood with layering (arrow) is seen in post-ESWL scan(D)
- 1035 -
B
D
A
B
大혐}jj(Íj‘t*~~씬J}~1깐과‘ • 명 23양 까 6 싸 1987
Fig. 5. Perinephric soft tissue stranding and thickening of the Gerota’s fascia‘
A. Multiple renal stones with focal caliectasis is seen in the lower pole of the left kidney in pre ESWL scan
B. Curvilinear stranding of the perinephric soft tissues and thickening of the Gerota’s fascia are evident in post-ESWL scan
lithotripter or localization with ultrasound 2) Generation of the shock waves by synchroniz- ecl multiple piezoelectric crystals mountecl on a spherical clish without reflector for focusing ancl localization of stone by ultrasouncl such as EDAP lithotripter. 1-5)
Although the complications after ESWL are mainly of urological problems such as pain, hematuria, ureteral obstruction and sepsis, possibilities of clamaging the kiclney ancl perinephric tissues cannot be neglectecl for focusecl shock waves must traverse the soft
before reaching calculi. Gross hematuria occurs in virtual1y al1 patients after ESWL, which is self-limited ancl clears within one day, and it has been speculated that virtually al1 patients SUS-
tains some forms of renal trauma during ESWL.6)
Of the 130 treated kiclneys stucliecl with CT scan, 87 kidneys showed significant swel1ing.
Measurement of the treated kidneys showed mean increase of 12.6% in short axis and 4.5%
in long axis at the level of the stone, 11.3% and 5.2% at the level of the renal hilum respective- ly. Swel1ing of the kidney after ESWL has already been reported by Kaude et al. on ex- cretory urography in seven (18%) of 41 kidneys with an average increase of 1.8cm in length7).
Grantham et al. found in 26 kidneys (26%) of 100 treated kidneys with an average increase of 2.4cm in length8). Rubin et al. founcl in 34 (64%) of 53 treated kidneys with an average in- crease of 9% in AP dimension on CT scan6). CT findings of renal contusion is wel1 known and although intravenous contrast media is not ad- ministered in our study, swel1ing of the kidney after ESWL seemed to be largely due to renal contusion and in the minority of cases ureteral obstruction played some role6.9).
Acute subcapsular hematoma was found in five (4%) patients in our study, two were ex- tensive and three were smal1 in amount, and none of the patient required surgery or in- terventional procedures. Chaussy et al reported 0.6% incidence of post-ESWL subcapsular hematomas in their ultrasound evaluation of nearly 1,000 patients and Rubin et al. reported 15% incidence of subcapsular hematoma in their CT study6) Kaude et al reported 24% in- cidence of subcapsular hematoma and Baum- gartner reported 26% incidence of subcapsular hematoma in the MR evaluation of post-ESWL kidne ys7.l0). Rubin explained apparent discrepancy of inciclence of subcapsular hematoma with Chaussy’s series for different number of shock waves are given to the patient, tissues of back, perinephric space and kidney two times more shock waves in Rubins series
- 1036-
Kounn Sik Song, et a1.: Effects 01 Extracorporeal Shock Wave Lithotripsy on the Kidney and Perinephric tissues- than Chaussy’s. Baumgartner explained this
discrepancy for relatively low sensitivity of ultrasonography to detect small amount of sub- capsular hematoma. Low incidence of subcap- sular hematoma in our series cannot be compared with Rubin’s series for absolute acoustic energy given to the patients are differ in parameter, but some difference of quality of the shock waves generated by spark gap discharge and piezoelectric crystals was at least partly responsible if not all.
Small parenchymal hematoma were found in four of our patients. Incidence of parenchymal hematoma was similar with Rubin’s series6).
These parenchymal hematoma maybe resulted from the severe renal contusion due to shock waves. Hemorrhage into a preexisting simple cortical cyst was found in one patient.
Seventy nine patients (61 %) in our series showed curvilinear thickening and stranding of perinephric tissues and associated Gerota’s fascia thickening. Rubin et al. has already reported in his CT evaluation of post-ESWL kidneys and perinephric tissues above findings similar in incidence with our series6). Three groups of bridging septa divide the perinephric space into several compartment are well known and these are fibrous connective tissue septa which connect the renal capsule to the Gerota’s fascia and septa which connect the anterior and posterior renal fascia 11) • As was pointed out by Rubin et al. increased perinephric soft tissue stranding and thickening of the Gerota’s fascia on post-ESWL CT scan maybe related to edematous thickening of these bridging connec- tJve tJssue septa.
Conclusion
lithiasis. Morphologic changes of the kidney and perinephric tissues after ESWL in our 130 patients are clinically insignificant and self- limited in most cases, so ESWL can be regard- ed as a safe modality for treatment of the renal and ureteral calculi.
REFERENCES
1. Gravenstein, j.5., Peter, K.: Extracorporeal shock-wave lithotripsy for renal stone disease- Technical and clinical aspects. 1st Ed: 5-1, Butterworths, Boston, 1986 2. Chaussy, c., Schmiedt, E., jocham, D. et al.: First clinica!
experiences with extracorporeally induced destruction of kidney stones by shock waves.}. UroI127:411-420, 1982 3. Chaussy, c., Schmiedt, E.: Shock wave treatment for stones
in the upper urinary tract. Urol Clin North Am. 10:143-150, 1983
4. Chaussy, c., Schmiedt, E., jocham, E. et al.: Extracorporeal shock wave lithotripsy (ESWL) for treatment of urolithiasis Urology 23:59-66, 1984
5. LeRoy, A.j., Arger, P.H., Pollack, H.M. et al.: Extracorporeal shock wave Iithotripsy. Radiol clin North Am 24.623-631,
1986
6. Rubin, j.l., Arger, P.H., Pollack, H.M. et al.: Kidney changes after extracorporeal shock wave lithotripsy: CT evaluation Radiology 162:21-24, 1981
7. Kaude, j.V., Williams, C.M., Millner, M.R. et al.: Renal mor- phology and function immediately after extracorporeal shock wave Iithotripsy. AjR 145:305-313, 1985 8. Grantham, J.R., Millner, M.R., Kaude, j.v. et al.: Renalstone
disease treated with extracorporeal shock wave Iithotripsy short term observations in 100 patients. Radiology 158:203-206, 1986
9. Lang, E.K., Sullivan, L Frentz, C: Renal trauma: Radiological studies. Radiology 154:1-6, 1985
10. Baumgartner, B.R., Dickey, K.W., Ambrose, S.s. et al
Kidney changes after extracorporeal shock wave Iithotrip sy: Appearance on MR imaging. Radiology 163:531-544,
Extracorporeal shock wave lithotripsy had 1981
a major impact on the treatment of renal and 11. Kunin, M.: Bridging sep떠 of the perinephric space
ureteral calculi and established as a primary anatomiι pathologic and diagnostic considerations
noninvasive modality for treatment of nephro- Radiology 158:361-365, 1986