43
C A S E REPO RT
pISSN: 2384-3799 eISSN: 2466-1899 Int J Thyroidol 2016 May 9(1): 43-46 http://dx.doi.org/10.11106/ijt.2016.9.1.43
Received October 21, 2015 / Revised January 25, 2016 / Accepted February 22, 2016
Correspondence: Jee Soo Kim, MD, PhD, Division of Breast and Endocrine Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea Tel: 82-2-3410-0253, Fax: 82-2-3410-6982, E-mail: jskim0126@skku.edu
Copyright ⓒ 2016, the Korean Thyroid Association. All rights reserved.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creative- commons.org/licenses/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Thyroid Hemiagenesis Associated with Papillary Thyroid Carcinoma
Inhye Park, Jun Ho Choi, Jung-Han Kim and Jee Soo Kim
Division of Breast and Endocrine Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Thyroid hemiagenesis is a rare congenital anomaly that is caused by a developmental defect of a thyroid.
Previous reports indicate that thyroid cancer associated with hemiagenesis is extremely rare. A 47-year-old woman presented with single nodule in the right thyroid gland that was incidentally detected during a routine medical checkup. Ultrasonography showed a 1.5×1.2 cm sized ill-defined irregular hypoehoic nodule in the right thyroid and the isthmus was present. However, the left thyroid was not seen and thyroid was disconnected at left paraisthmic area. Fine-needle aspiration cytology confirmed that the right thyroid nodule was papillary thyroid carcinoma. Total thyroidectomy with bilateral central compartment node dissection was performed.
Permanent pathologic finding was 1.3×1 cm sized classical type papillary thyroid carcinoma with nodular hyperplasia. There was extensive lymphatic invasion and 3 metastatic lymph nodes out of 4 in central compartment. In conclusion, although thyroid hemiagenesis associated with thyroid carcinoma is extremely rare, treatment strategy is not different with patients with normal anatomy. And the possibility of developing a thyroid carcinoma should be considered in patients with hemiagenesis. Furthermore, it requires awareness of anatomical difference around the thyroid gland during operation.
Key Words: Thyroid hemiagenesis, Thyroid cancer, Papillary thyroid carcinoma
Introduction
Thyroid hemiagenesis is an uncommon congenital anomaly that is caused by a developmental defect of a thyroid or failure of its precursor to migrate to the normal location.1,2) The prevalence of thyroid hemia- genesis is reported as 0.05-0.2%.3-5) Its occurrence is mostly concomitant other pathologic conditions such as Graves’ disease, multinodular goiter, and thyroiditis.
Previous reports indicate that thyroid cancer asso- ciated with hemiagenesis is extremely rare.3) In this study, we presented a case of hemiagenesis of thyroid associated with papillary carcinoma.
Case Report
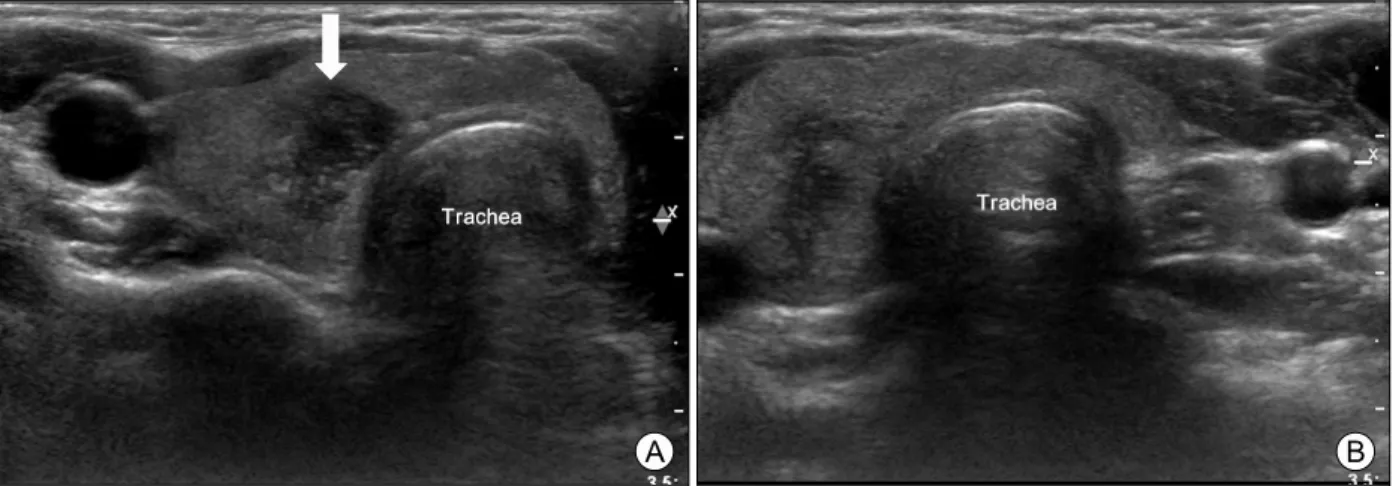
A 47-year-old woman presented with single nod- ule in the right thyroid gland that was incidentally de- tected during a routine medical checkup. There was no history of previous radiation to the neck or any other history of thyroid disease. Her older sister was diagnosed papillary thyroid carcinoma without con- genital anomaly of thyroid. Clinical examination re- vealed no cervical lymphadenopathy. Ultrasonography showed a 1.5×1.2 cm sized ill-defined irregular hy- poechoic nodule in the right thyroid and the isthmus was present. However, the left thyroid was not seen and thyroid was disconnected at left paraisthmic area
Inhye Park, et al
Vol. 9, No. 1, 2016 44 Fig. 1. Ultrasonography of the thyroid gland showing one hypoechoic nodule (arrow) in the right thyroid (A) and no thyroid tissue in the left thyroid (B).
Fig. 2. Operative finding of specimen showing absence of left lobe.
(Fig. 1). Fine-needle aspiration cytology confirmed that the right thyroid nodule was papillary thyroid carcino- ma; in addition, BRAFV600E mutation was not detected.
Neck CT, MRI or thyroid scan were not performed.
The patient was biochemically euthyroid (thyroid stim- ulating hormone [TSH]: 1.57 μIU/mL [normal range, 0.3-6.0 μIU/mL], free T4: 1.25 ng/dL [normal range, 0.79-1.86 ng/dL], T3: 104.3 ng/dL [normal range, 76-190 ng/dL, Calcitonin: 7.8 pg/mL [normal range, 1.9-9.6 ng/dL]).
Total thyroidectomy with bilateral central compart- ment node dissection was performed (Fig. 2). Thyroid nodule was hard in the right lobe and gross perithyr- oidal invasion was not detected. The left superior and inferior parathyroid glands were located on the tra- cheoesophageal groove and preserved in situ.
Because thyroid hemiagenesis is rare, extent of lymph node dissection of thyroid carcinoma in patient with hemiagenesis is still unclear. But in this patient, meta- static papillary carcinoma of right central lymph node was found in frozen biopsy. We considered risk of contralateral central lymph node metastasis and per- formed contralateral central lymph node dissection.
Permanent pathologic finding was 1.3×1 cm sized classical type papillary thyroid carcinoma with nodular hyperplasia. There was extensive lymphatic invasion and 3 metastatic lymph nodes out of 4 in central com- partment (right central lymph node 2/3, left central lymph node 1/1). Postoperative TSH was 1.26 μIU/ml (normal range, 0.3-6.0 μIU/ml) and free T4 was 1.85
ng/dL with levothyroxine 150 ug per day (normal range, 0.79-1.86 ng/dL). Parathyroid hormone level was 41.1 pg/dL (normal, 11.0-62.0).
Discussion
Thyroid hemiagenesis is a rare congenital anomaly that is caused by a developmental defect of a thyroid or failure of its precursor to migrate to the normal location.1,2) It was first described by Handfield-Jones in 1866. The prevalence of thyroid hemiagenesis is re- ported as 0.05-0.2%, and is more frequently found in women. Absence of the left lobe is more common and absence of the isthmus occurs in 50% of cases.5,6) But,
Thyroid Hemiagenesis with PTC
45 Int J Thyroidol
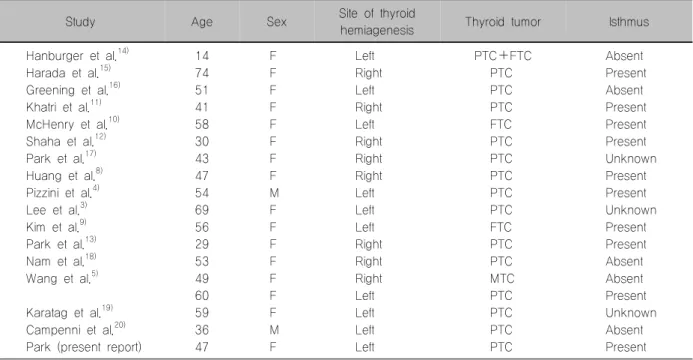
Table 1. Thyroid hemiagenesis associated with thyroid cancer
Study Age Sex Site of thyroid
hemiagenesis Thyroid tumor Isthmus
Hanburger et al.14) 14 F Left PTC+FTC Absent
Harada et al.15) 74 F Right PTC Present
Greening et al.16) 51 F Left PTC Absent
Khatri et al.11) 41 F Right PTC Present
McHenry et al.10) 58 F Left FTC Present
Shaha et al.12) 30 F Right PTC Present
Park et al.17) 43 F Right PTC Unknown
Huang et al.8) 47 F Right PTC Present
Pizzini et al.4) 54 M Left PTC Present
Lee et al.3) 69 F Left PTC Unknown
Kim et al.9) 56 F Left FTC Present
Park et al.13) 29 F Right PTC Present
Nam et al.18) 53 F Right PTC Absent
Wang et al.5) 49 F Right MTC Absent
60 F Left PTC Present
Karatag et al.19) 59 F Left PTC Unknown
Campenni et al.20) 36 M Left PTC Absent
Park (present report) 47 F Left PTC Present
FTC: follicular thyroid carcinoma, MTC: medullary thyroid carcinoma, PTC: papillary thyroid carcinoma
the true prevalence of this congenital abnormality is dif- ficult to verify, because the absence of one thyroid lobe alone usually does not lead to clinical manifestations.
The diagnosis is frequently incidental in the setting of concomitant thyroid disorders.7)
In the remnant thyroid lobe, pathologic conditions including follicular adenoma, multinodular goiter, chronic thyroiditis and Graves’ disease are common.2-4,8) However, thyroid hemiagenesis associated with papil- lary thyroid carcinoma is extremely rare with only 18 patients reported including 14 papillary carcinoma, 2 follicular carcinoma, 1 medullary carcinoma, 1 mixed papillary and follicular carcinoma. Sixteen patients were women and hemiagenesis occurred on the left in 11 cases and the right in 7 cases.5) Mean age was 48.3 years old (range, 14-74), without significant dif- ference from patients with thyroid cancer, except de- velopment defect. The isthmus could be found in 10 patients (Table 1).4,5,8-13)
Hemiagenesis is usually asymptomatic, if not con- comitant with another condition causing hyper- or hypothyroidism. It is diagnosed by imaging methods including ultrasonography, CT, MRI and/or thyroid scanning.3,5) Treatment strategy for thyroid carcinoma patients with hemiagenesis was not different in patients
with anatomically normal thyroid gland.3,5) However, the location of parathyroid gland and the course of re- current laryngeal nerve could differ from the normal thyroid gland, hence, greater intra-operative care is required from the surgeon.
In conclusion, although thyroid hemiagenesis asso- ciated with thyroid carcinoma is extremely rare, the possibility of developing a thyroid carcinoma should be considered in patients with hemiagenesis. Further- more, it requires awareness of anatomical difference around the thyroid gland during operation.
References
1) Lipin R, Kandil E. Thyroid hemiagenesis. J La State Med Soc 2012;164(4):205-6.
2) Sari O, Ciftci I, Toru M, Erbas B. Thyroid hemiagenesis.
Clin Nucl Med 2000;25(10):766-8.
3) Lee YS, Yun JS, Jeong JJ, Nam KH, Chung WY, Park CS.
Thyroid hemiagenesis associated with thyroid adenomatous hyperplasia and papillary thyroid carcinoma. Thyroid 2008;
18(3):381-2.
4) Pizzini AM, Papi G, Corrado S, Carani C, Roti E. Thyroid hemiagenesis and incidentally discovered papillary thyroid cancer: case report and review of the literature. J Endocrinol Invest 2005;28(1):66-71.
5) Wang J, Gao L, Song C. Thyroid hemiagenesis associated with medullary or papillary carcinoma: report of cases. Head
Inhye Park, et al
Vol. 9, No. 1, 2016 46 Neck 2014;36(11):E106-11.
6) Maiorana R, Carta A, Floriddia G, Leonardi D, Buscema M, Sava L, et al. Thyroid hemiagenesis: prevalence in normal children and effect on thyroid function. J Clin Endocrinol Metab 2003;88(4):1534-6.
7) Shabana W, Delange F, Freson M, Osteaux M, De Schepper J. Prevalence of thyroid hemiagenesis: ultrasound screening in normal children. Eur J Pediatr 2000;159(6):456-8.
8) Huang SM, Chen HD, Wen TY, Kun MS. Right thyroid hemiagenesis associated with papillary thyroid cancer and an ectopic prelaryngeal thyroid: a case report. J Formos Med Assoc 2002;101(5):368-71.
9) Kim B, Kim IA. Means of monitoring the course of postoperative inflammatory processes in the abdominal cavity. Vestn Akad Med Nauk SSSR 1981(6):46-8.
10) McHenry CR, Walfish PG, Rosen IB, Lawrence AM, Paloyan E. Congenital thyroid hemiagenesis. Am Surg 1995;
61(7):634-8; discussion 8-9.
11) Khatri VP, Espinosa MH, Harada WA. Papillary adenocar- cinoma in thyroid hemiagenesis. Head Neck 1992;14(4):312-5.
12) Shaha AR, Gujarati R. Thyroid hemiagenesis. J Surg Oncol 1997;65(2):137-40.
13) Park J-Y, Kim SJ, Cho YU. Thyroid hemiagenesis associated
with micropapillary thyroid carcinoma. J Korean Surg Soc 2010;78(2):116-8.
14) Hamburger JI, Hamburger SW. Thyroidal hemiagenesis. Report of a case and comments on clinical ramifications. Arch Surg 1970;100(3):319-20.
15) Harada T, Nishikawa Y, Ito K. Aplasia of one thyroid lobe.
Am J Surg 1972;124(5):617-9.
16) Greening WP, Sarker SK, Osborne MP. Hemiagenesis of the thyroid gland. Br J Surg 1980;67(6):446-8.
17) Park SG, Ryu JW, Myung NH. Thyroid hemiagenesis and ectopic thymus at thyroid bed, and papillary cancer in opposite thyroid lobe with hyperthyroidism. J Korean Surg Soc 2000;
58(3):433-7.
18) Nam YM, Park JS, Na KH, Ahn D. A case of thyroid hemiagenesis with concurrent papillary thyroid carcinoma.
Korean J Otorhinolaryngol-Head Neck Surg 2011;54(8):557-9.
19) Karatag GY, Albayrak ZK, Onay HK, Karatag O, Peker O.
Coexistence of thyroid hemiagenesis, nodular goitre and papillary carcinoma. Kulak Burun Bogaz Ihtis Derg 2013;23(2):115-8.
20) Campenni A, Giovinazzo S, Curto L, Giordano E, Trovato M, Ruggeri RM, et al. Thyroid hemiagenesis, Graves' disease and differentiated thyroid cancer: a very rare association: case report and review of literature. Hormones (Athens) 2015;14(3):451-8.