서 론
골다공증은 골량의 감소와 뼈의 미세구조 변화로 골강도가 감소 되어 골절의 위험성이 증가하는 질환이다.1) 50세 이상 한국인의 골 다공증 유병률은 여성에서 38%, 남성에서 7.3% 정도로 관찰되며,2) 노
인 인구가 늘어나면서 골다공증 유병률도 점차 증가할 것으로 예상 된다. 또한 골다공증으로 인한 골절은 높은 사망률과 많은 경제적 비용을 초래하므로 사회적으로 중요한 문제이다.
비만은 전통적으로 골다공증의 보호인자로 생각되어 왔으며, 체 중이나 체질량지수가 증가할수록 골밀도가 증가하는 것으로 알려
Received July 6, 2017 Revised August 22, 2017 Accepted August 30, 2017
Corresponding author Eun-Ju Sung Tel: +82-2-2001-2277, Fax: +82-2-2001-1404 E-mail: eunjusung68@gmail.com
ORCID: http://orcid.org/0000-0002-6045-3154
Copyright © 2018 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Original Article
https://doi.org/10.21215/kjfp.2018.8.4.593 eISSN 2233-9116
Korean J Fam Pract. 2018;8(4):593-600
Korean Journal of Family Practice
KJFP
한국인 60세 이상 성인에서 비만과 대사적 건강 상태에 따른 요추 골밀도와의 관계
김민지
1, 성은주
1,*, 김철환
1, 신호철
1, 이선영
21성균관대학교 의과대학 강북삼성병원 가정의학교실, 2인제대학교 의과대학 상계백병원 가정의학교실
Association of Lumbar Spine Bone Mineral Density According to Obesity and Metabolic Health Status in Korean 60 Years of Age or Older
Min-Ji Kim1, Eun-Ju Sung1,*, Cheol-Hwan Kim1, Ho-Cheol Shin1, Seon-Yeong Lee2
1Department of Family Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine; 2Department of Family Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
Background: Obesity has been considered a protective factor for osteoporosis. Being obese not only means being overweight, but also having metabolic derangements. Several studies have shown that metabolic abnormalities may have negative effects on bone mineral density (BMD), but the evidence is inconclusive. We compared BMD according to a metabolically healthy obesity phenotype to analyze the influence of metabolic abnormalities and obesity on BMD.
Methods: We conducted a cross-sectional study of Korean adults who underwent a health screening program between 2010 and 2013. A total of 1,298 subjects (550 women and 748 men) were included. Lumbar spine (LS) BMD was assessed using dual-energy X-ray absorptiometry. Obesity was defined as body mass index (BMI) of 25 kg/m2 or higher. Participants were classified as being metabolically healthy if fewer than two of the following were present: hypertension, hyperglycemia, hypertriglyceridemia, and low high-density lipoproteinemia. Analyses were conducted in four groups that were divided according to obesity and metabolic health: metabolically healthy non-obese (MHNO), metabolically unhealthy non-obese (MUHNO), metabolically healthy obese (MHO), and metabolically unhealthy obese (MUHO).
Results: The mean values of LS BMD were higher in obese groups (MHO and MUHO) than in non-obese groups (MHNO and MUHNO). However, there were no significant differences between MHNO and MUHNO and between MHO and MUHO, which were different in metabolic health status. After adjusting for BMI and other covariates, there were no differences in LS BMD between the four groups.
Conclusion: Overweight may be an important factor in BMD, whereas metabolic health did not appear to be associated with BMD.
Keywords: Obesity; Metabolically Benign; Metabolic Syndrome; Bone Density
Min-Ji Kim, et al. Bone Mineral Density According to Obesity and Metabolic Health Status
Korean Journal of Family Practice
KJFP
져 있다.3,4) 그러나 비만은 인슐린 저항성, 만성 염증, 산화스트레스 등의 대사 이상을 초래하며, 이러한 대사 이상은 전염증성 사이토카 인을 증가시키고, 지방세포에서 에스트로겐, 렙틴, 아디포넥틴과 같 은 호르몬 분비를 통해 골대사에 영향을 미치는 것으로 알려져 있 다.5) 죽상동맥경화증과 낮은 골밀도와의 연관성들이 보고되면서,6) 죽상동맥경화증의 전구상태인 대사증후군과 골밀도와 연관성을 밝히기 위한 많은 연구들이 이루어졌으나, 아직 일관된 결론을 내리 지 못하고 있다.7,8) 한국인 40세 이상 남성 1,780명과 폐경 후 여성 1,108명을 대상으로 대사증후군과 대퇴 경부 골밀도의 연관성을 분 석한 연구에서 체중을 포함한 교란변수 보정 후 남녀 모두 대사증 후군이 있는 군에서 골밀도가 더 낮았고,9) 성인 여성 2,265명을 대상 으로 한 연구에서도 폐경 전 여성에서는 요추 골밀도가, 폐경 후 여 성에서는 요추부와 대퇴 경부 골밀도가 대사증후군과 역의 상관관 계를 보였다.10) 성인 여성 2,475명을 대상으로 한 또 다른 연구에서도 대사증후군이 있는 군에서 요추 골밀도가 더 낮게 나타났다.11) 한편 한국인 20세 이상 성인 남녀를 대상으로 한 일부 연구들에서는 남성 의 경우에는 마찬가지로 대사증후군이 낮은 골밀도와 연관성이 있 었으나, 여성에서는 연관성이 없었다.12-14) 또한 미국의 란쵸 베르나르 도 연구(Rancho Bernardo Study)에서도 체질량지수를 포함한 교란변 수 보정 후 남성에서는 대사증후군과 대퇴 경부 골밀도가 역의 상관 관계를 보였으나, 여성에서는 연관성이 없었다.15) 이러한 결과들은 대사이상이 골밀도에 부정적인 영향을 미칠 가능성을 제시하나 아 직 결론에 논란이 있다.
한편, 단순히 체질량지수만으로 정의한 비만은 대사 질환에 대한 위험도를 예측하는데 한계가 있다는 점에서 대사 이상이 동반되지 않은 비만의 형태가 제시되고 있다. 아직 일관된 정의가 정립되지는 않았으나, 체질량지수는 비만이지만 대사적으로 건강한 사람을 metabolically healthy obese (MHO), 체질량지수는 정상이지만 대사 적 위험요인을 가지고 있는 사람을 metabolically unhealthy non-obese (MUHNO)로 지칭한다.16) 이러한 개념은 체질량지수를 기준으로는 같은 비만 범주이더라도, 대사적 건강상태에 따라 접근이나 중재가 달라질 수 있다는 점에서 주목할 만하다.
본 연구는 한국 60세 이상 성인을 대상으로 비만 형태에 따른 골 밀도 차이를 확인하고, 대사이상과 골밀도와의 관련성과 비만이 이 에 미치는 영향을 분석하고자 한다.
방 법
1. 연구 대상 및 기간
2010년 1월부터 2013년 12월까지 강북삼성병원 종합검진센터 방
문자 중 강북삼성코호트연구(Kangbuk Samsung Cohort Study, KSCS) 에 등록된 수진자를 대상으로 단면 연구를 실시하였다. 검진 항목 으로 요추 골밀도 검사가 포함된 60세 이상 수진자 총 3,308명 중 대 사적 지표 및 설문 항목 누락자(n=1,681), 악성종양(n=94)이나 갑상샘 질환 과거력(n=172)이 있거나, 현재 혹은 최근 1개월 이내 1주일 이상 여성 호르몬제(n=22), 골다공증 치료약물(n=39), 경구 스테로이드 (n=2) 복용 이력이 있는 사람을 제외한 1,298명을 최종 연구 대상으 로 하였다(Figure 1). 본 연구는 강북삼성병원 연구윤리심의위원회 (Institutional Review Board, IRB)의 사전 승인을 받아 진행하였다 (IRB no. 2015-07-003).
2. 신체 계측 및 생화학적 검사
신장(cm)은 BSM330 (Biospace, Vacaville, CA, USA)을 이용하여 측 정하였다. InBody 720 (Biospace)을 이용하여 체성분 분석을 시행하 였고, 체중(kg), 체질량지수(kg/m2), 근육량(kg), 체지방량(kg)을 측정 하였다. 복부둘레(cm)는 SECA201 tape (Seca, Hamburg, Germany)을 이용하여 기립상태에서 마지막 늑골 하단과 장골능선의 상단부위 두 점의 중간지점에서 측정하였다. 혈압은 5분간 휴식 후 표준화된 혈압계를 이용하여 측정하였다. 생화학적 검사를 위해 채혈 전 12시 간 이상 금식 후 총 콜레스테롤과 중성지방, 고밀도 지단백 콜레스테 롤, 저밀도 지단백 콜레스테롤은 Hitachi 7600 (Hitachi, Tokyo, Japan) 을 이용하여 enzymatic calorimetric test와 liquid-selective detergent methods로 측정하였고, 공복혈당은 hexokinase/glucose-6-phosphate
2,010 were excluded
Missed data for any metabolic parameters or questionnaire (n=1,681) History of malignancy (n=94)
History of thyroid disease (n=172) Current medication (n=63)
HRT (n=22) Osteoporosis (n=39) Steroids (n=2) n=3,308
Women n=550
Men n=748 n=1,298
Figure 1. Flow chart of the study subjects.
HRT, hormonal replacement therapy.
김민지 외. 비만과 대사적 건강 상태에 따른 요추 골밀도와의 관계 Korean Journal of Family Practice
KJFP
dehydrogenase (Hitachi 7600 Modular Dp-110 autoanalyzer; Hitachi) 방 법으로, 공복 인슐린은 radioimmunoassay (Packard Cobra II 5010;
Packard Instrument, Baltimore, MD, USA)로 측정하였다. 인슐린 저항 성 평가를 위한 HOMA-IR (homeostatic model assessment-insulin re- sistance)은 다음 식에 따라 구하였고: (fasting insulin [IU/mL]*fasting glucose [mmoL/L])22.5,17) hs-CRP (high sensitivity C-reactive protein)는 particle-enhanced immunoturbidimetric assay (Modular P800; Roche Diagnostics, Tokyo, Japan)를 이용하여 측정하였다.
당뇨병 약과 고혈압 약 복용 여부, 흡연, 음주, 신체활동 여부는 문 진표를 이용한 자가 기입 방식으로 평가하였다. 흡연자는 생애 동안 5갑 이상의 흡연을 한 적이 있는 사람으로 정의하였으며, 음주자는 하루 평균 3잔 이상의 음주력을 가진 경우로 정의하였다. 신체 활동 에 대한 평가로 지난 7일간 무거운 물건 나르기, 달리기 등 격렬한 신 체활동 시행 일수가 4일 이상인 경우로 정의하였다.
3. 골밀도 측정
골밀도는 이중 에너지 X-선 흡수계측법(PRODIGY advance; Madi- son, WI, USA)을 이용하여 측정하였으며, 변동계수는 1.0%이었다. 요 추골 1번에서 4번까지의 평균값을 보고하였고, 퇴행성변화, 압박 골 절, 인공 삽입물이 존재하는 척추를 배제하기 위해 T-score가 인접한 척추와 1 표준편차(standard deviation) 이상 차이 나거나, 위에 있는 요추가 아래에 있는 요추보다 골밀도가 높은 경우 제외하고 골다공 증 여부를 판단하였다.
4. 대사적으로 건강한 비만의 정의
비만은 세계보건기구에서 제시하는 아시아-태평양 가이드라인18) 의 체질량지수(body mass index, BMI) 범주에 따라 정의하였다. 대사 적으로 건강한 상태는 미국심장학회/국립심폐혈연구소(American Heart Association/National Heart, Lung, and Blood Institute)의 대사증 후군 진단기준에서,19) BMI와 밀접한 관련성을 가지는 허리둘레는 제외하고 다음 위험 요인들 중 2가지 미만을 만족하는 경우로 정의 하였다:
1) 수축기 혈압 ≥130 mmHg 또는 이완기 혈압 ≥85 mmHg, 또는 고 혈압 약 복용 중
2) 공복혈당 ≥100 mg/dL 또는 당뇨병 약 복용 중 3) 중성지방 ≥150 mg/dL
4) 고밀도 콜레스테롤 <40 mg/dL (남성) 또는 <50 mg/dL (여성) 아래 기준에 따라, 대상자들을 4군으로 분류하였다 :
1) 대사적으로 건강하고 비만이 아닌 군(metabolically healthy non- obese, MHNO): BMI 25 미만이면서 대사적 위험요인 중 2가지
미만을 만족하는 경우
2) 비만은 아니지만 대사적으로 건강하지 않은 군(metabolically unhealthy non-obese, MUHNO): BMI 25 미만이면서 대사적 위 험요인 중 2가지 이상을 만족하는 경우
3) 비만이지만 대사적으로 건강한 군(metabolically healthy obese, MHO): BMI 25 이상이면서 대사적 위험요인 중 2가지 미만을 만 족하는 경우
4) 대사적으로 건강하지 않고 비만인 군(metabolically unhealthy obese, MUHO): BMI 25 이상이면서 대사적 위험요인 중 2가지 이상을 만족하는 경우
5. 통계 분석
성별에 따른 층화 분석을 시행하였으며, 연속형 변수는 평균값과 표준편차로, 명목형 변수는 빈도와 백분율로 표시하였다. 요추 골밀 도와 변수들간에 상관분석을 시행하였고, 나이를 보정하기 위해 부 분상관분석을 시행하였다. 체질량지수와 대사상태에 따른 네 군 간 의 비교에는 일원배치분산분석(one-way analysis of variance, ANO- VA)을 이용하였고, ANCOVA를 이용하여 교란변수들을 보정하였으 며, 사후 검정으로 Bonferroni 검정법을 이용하였다. 통계 분석은 IBM SPSS ver. 20.0 (IBM Co., Armonk, NY, USA) 프로그램을 이용하 였고 통계적 유의 수준은 P-value 0.05 미만으로 하였다.
결 과
1. 연구 대상자들의 일반적 특성
연구 대상자들의 특성을 Table 1에 나타내었다. 총 연구 대상자는 1,298명이며, 여성 550명, 남성 748명이었다. 전체 대상자들의 평균 나 이는 65.5세(60–84세)였고, BMI의 평균값은 여성에서 23.86 (16.4–
35.4) kg/m2, 남성에서 23.81 (15.7–34.3) kg/m2이었다. 여성의 2.7%, 남성 의 74.9%가 현재 또는 과거 흡연자였으며, 하루 평균 3잔 이상의 알코 올을 섭취하는 대상자 비율이 여성에서 0.9%, 남성에서 16.4%였다. 또 한 여성의 11.1%, 남성의 18.4%가 주 4회 이상 격렬한 운동을 시행한 다고 답변하였다.
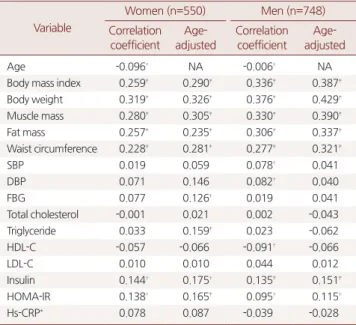
2. 요추 골밀도와 변수들간의 상관관계
평균 요추 골밀도는 나이가 증가함에 따라 감소하였으며, 여성에 서 더 두드러졌다. 나이 보정 후 체중이 가장 높은 상관성을 보였고, 체성분 구성요소 중에서는 근육량, 체지방량, 복부둘레 순으로 연관 성을 보였다. 또한 나이 보정 후 대부분의 대사적 변수들은 연관성이 없거나 낮았다. 단, 남녀 모두에서 인슐린과 HOMA-IR이, 여성에서
Min-Ji Kim, et al. Bone Mineral Density According to Obesity and Metabolic Health Status
Korean Journal of Family Practice
KJFP
공복 혈당, 중성지방이 골밀도와 양의 상관관계를 보였다(Table 2).
3. 체질량지수와 대사적 건강상태에 따른 네 군에서의 요추 골밀도 평가
대상자들을 비만과 대사적건강 상태에 따라 네 개의 군으로 나누 었다(Table 3). 여성에서는 MHNO군이 170명(30.9%), MUHNO군이 200명(36.4%), MHO군이 56명(10.2%), MUHO군이 124명(22.5%)이었 고, 남성에서는 MHNO군이 339명(45.3%), MUHNO군이 172명 (23.0%), MHO군이 93명(12.4%), MUHO군이 144명(19.3%)이었다.
네 군의 특성을 비교했을 때, 여성에서는 대사적으로 건강하지 않 은 군들에서 나이가 더 많았으나, 남성에서는 차이가 없었다. 대사적 상태에 따른 체중 차이는 없었고, 대사 변수들은 대사적으로 건강 하지 않은 군들에서 좋지 않았다. 또한 여성에서는 군간 흡연, 음주, 운동량에 차이가 없었고, 남성에서도 흡연율은 차이가 없었으나, 대 사적으로 건강한 군들에서 하루 3잔 이상 음주자의 비율이 낮고, 고 강도의 운동을 규칙적으로 하는 대상자의 비율이 더 높았다.
요추 골밀도의 평균값은 비만하지 않은 MHNO, MUHNO군에 비 해 비만한 MHO, MUHO군에서 더 높았다(Table 4). 그러나 사후분
석에서 MHNO와 MUHNO, MHO와 MUHO 사이에는 통계적으로 유의한 차이가 없었다. 체질량지수를 보정한 후에는 모든 군간의 골 밀도 차이가 사라졌으며, 나이와 흡연, 음주, 신체활동 등 교란변수 들을 보정한 후에도 같은 결과를 보였다.
고 찰
본 연구 결과, 비만한 군들에서 비만하지 않은 군들에 비해 요추 골밀도가 더 높았지만, 체질량지수가 유사한 경우 대사적 상태에 따 른 골밀도의 차이는 유의하지 않았다. 또한 체질량지수를 보정한 후 모든 군간에 대사 상태에 따른 골밀도 차이가 없었다. 이는 체질량지 수는 요추 골밀도와 높은 연관성을 가지나, 대사적 상태는 연관성이 낮음을 시사한다.
체중 및 체질량지수가 높을수록 골밀도 감소의 보호효과가 있다 는 것은 지속적으로 증명되어 왔다.3,4,20) 이는 체중의 기계적 부하에 의한 골형성 촉진, 피하 지방 세포에서 골소실을 억제하는 에스트로 겐 합성, 골형성을 자극하는 렙틴, 아디포넥틴 등의 호르몬 분비 등 으로 설명된다. 체성분 구성요소 중에서는 근육량이 체지방량보다 골밀도와 더 높은 연관성을 보였는데, 이는 Ho-Pham 등21)이 44개의 Table 1. Characteristics of the participants (n=1,298)
Variable Women (n=550) Men (n=748)
Age (y) 65.66±4.61 65.36±4.31
Body weight (kg) 56.80±8.07 66.98±9.32
Body mass index (kg/m2) 23.86±3.04 23.81±2.84 Waist circumference (cm) 82.87±8.47 85.62±8.39
SBP (mmHg) 117.24±14.74 117.88±13.91
DBP (mmHg) 70.81±9.31 74.62±9.07
FBG (mg/dL) 100.03±16.24 102.97±23.41
Total cholesterol (mg/dL) 209.01±38.70 193.88±34.28 Triglyceride (mg/dL) 109.80±60.19 116.05±67.31
HDL-C (mg/dL) 59.01±14.21 53.67±14.24
LDL-C (mg/dL) 134.43±36.01 123.67±31.89
Fasting insulin (uIU/mL) 5.381±2.900 5.047±3.041
HOMA-IR 1.395±1.133 1.341±1.053
Total lumbar BMD (g/cm2) 0.947±0.165 1.151±0.194 Hs-CRP* (mg/L) 0.050 (0.030–0.090) 0.060 (0.030–0.128) Proportion of subjects who
has ever smoked
15 (2.7) 560 (74.9)
Proportion of subjects who drink alcohol 3 or more units/day
5 (0.9) 123 (16.4)
Proportion of subjects who do regular vigorous exercise 4 or more times/week
61 (11.1) 138 (18.4)
Values are presented as mean±standard deviation or number (%).
SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, Fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipopro- tein cholesterol; HOMA-IR, homeostasis model assessment-insulin resistance;
BMD, bone mineral density; Hs-CRP, high sensitivity C-reactive protein.
*Hs-CRP is presented as median (Interquartile range).
Table 2. Correlation analysis of lumbar spine BMD and variables Variable
Women (n=550) Men (n=748) Correlation
coefficient
Age- adjusted
Correlation coefficient
Age- adjusted
Age -0.096† NA -0.006† NA
Body mass index 0.259‡ 0.290‡ 0.336‡ 0.387‡
Body weight 0.319‡ 0.326‡ 0.376‡ 0.429‡
Muscle mass 0.280‡ 0.305‡ 0.330‡ 0.390‡
Fat mass 0.257‡ 0.235‡ 0.306‡ 0.337‡
Waist circumference 0.228‡ 0.281‡ 0.277‡ 0.321‡
SBP 0.019 0.059 0.078† 0.041
DBP 0.071 0.146 0.082† 0.040
FBG 0.077 0.126† 0.019 0.041
Total cholesterol -0.001 0.021 0.002 -0.043
Triglyceride 0.033 0.159‡ 0.023 -0.062
HDL-C -0.057 -0.066 -0.091† -0.066
LDL-C 0.010 0.010 0.044 0.012
Insulin 0.144† 0.175† 0.135‡ 0.151‡
HOMA-IR 0.138† 0.165‡ 0.095† 0.115†
Hs-CRP* 0.078 0.087 -0.039 -0.028
BMD, bone mineral density; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, Fasting blood glucose; HDL-C, high-density lipoprotein cholester- ol; LDL-C, low-density lipoprotein cholesterol; HOMA-IR, homeostasis model as- sessment-insulin resistance; Hs-CRP, high-sensitivity C-reactive protein; NA, not available.
Data were analyzed using Pearson’s correlation and partial correlation as appro- priate.
*Hs-CRP was log-transformed. †P<0.05. ‡P<0.01.
김민지 외. 비만과 대사적 건강 상태에 따른 요추 골밀도와의 관계 Korean Journal of Family Practice
KJFP
Table 3. Comparison of variables among the groups divided according to metabolic health and obesity status Variable
Women (n=550)Men (n=748) MHNO (n=170)MUHNO (n=200)MHO (n=56)MUHO (n=124)P-value*MHNO (n=339)MUHNO (n=172)MHO (n=93)MUHO (n=144)P-value* Age (y)64.78±3.94†66.08±4.61‡,§64.48±4.26†,‡66.71±5.30§0.00065.30±4.0565.76±4.8265.12±4.5865.15±4.120.540 Body weight (kg)52.31±5.70†53.67±5.80†64.37±6.77‡64.58±6.34‡0.00062.18±6.56†63.81±6.92†75.96±7.15‡76.32±7.36‡0.000 body mass index (kg/m2)21.91±1.9022.50±1.7727.19±2.15†27.24±2.08†0.00022.14±1.9322.77±1.7726.79±1.86†27.06±1.76†0.000 Muscle mass (kg)34.12±3.08†34.44±3.30†37.33±3.32‡36.84±3.63‡0.00046.39±4.13†46.43±5.00†52.25±4.87‡51.67±4.97‡0.000 Fat mass (kg)16.13±3.75†17.16±3.82†24.83±4.66‡25.52±4.63‡0.00013.17±3.8714.74±3.4820.74±4.76†21.70±4.71†0.000 Waist circumference (cm) 77.79±6.4779.98±6.1389.81±5.69†91.38±6.58†0.00081.00±6.5483.70±5.8892.70±6.37†94.19±6.10†0.000 SBP (mmHg)109.79±11.14121.08±15.13†,‡115.64±12.41†122.01±15.35‡0.000113.16±12.49122.66±14.81†,‡118.42±12.42†,§122.93±13.23‡,§0.000 DBP (mmHg)68.20±8.29†72.10±9.67‡,§71.11±8.57†,‡,∥72.16±9.72§,∥0.00072.56±8.2776.37±10.06†,‡75.55±8.78†,§76.80±8.86‡,§0.000 FBG (mg/dL) 91.18±7.56†103.65±17.5195.89±12.15†108.22±18.220.00094.73±16.03†112.92±29.48‡96.35±14.23†114.74±25.26‡0.000 Total cholesterol (mg/dL)211.36±35.37207.21±39.22207.96±38.57209.19±42.410.776195.08±32.64†,‡197.98±38.19†,§194.02±33.13‡,§,∥186.08±32.95∥0.016 Triglyceride (mg/dL)90.46±37.15†114.25±66.76‡,§104.11±40.77†,‡131.73±72.61§0.00088.44±39.50†152.20±86.11‡94.83±30.56†151.56±74.63‡0.000 HDL-C (mg/dL)60.17±14.54†,‡60.28±14.58†,§52.71±14.09∥58.23±12.44‡,§,∥0.00357.63±13.54†50.57±15.01‡,§55.12±13.57†,‡47.10±11.99§0.000 LDL-C (mg/dL)137.91±32.14131.13±36.06140.04±36.51132.45±40.190.171124.64±30.57126.02±34.07125.72±31.52117.24±31.980.057 Fasting insulin (uIU/mL)4.289±1.6495.397±3.029†5.818±2.731†,‡6.656±3.501‡0.0004.183±1.8105.241±2.930†5.939±5.242†,‡6.273±2.962‡0.000 HOMA-IR1.035±0.429†1.452±1.437‡1.419±0.691†,‡,§1.786±1.259§0.0001.050±0.4801.433±0.891†1.560±2.072†,‡1.774±01.05‡0.000 Hs-CRP (mg/L)0.103±0.0830.121±0.2020.142±0.1940.157±0.3270.1610.195±0.6830.238±0.7880.137±0.1450.131±0.0980.359 Total lumbar BMD (g/cm2)0.919±0.150†0.925±0.155†1.000±0.130‡0.997±0.196‡0.0001.106±0.175†1.134±0.199†1.236±0.196‡1.222±0.190‡0.000 Smoking (%)6 (3.5)6 (3.0)NA 3 (2.4)0.555246 (72.6)137 (79.7)73 (78.5)104 (72.2)0.238 Alcohol (%)1 (0.6)2 (1.0)NA2 (1.6)0.70439 (11.5)42 (24.4)13 (14.0)29 (20.1)0.001 Vigorous exercise (%)18 (10.6)24 (12.0)7 (12.5)12 (9.7)0.90275 (22.1)28 (16.3)19 (20.4)16 (11.1)0.030 Values are presented as mean±standard deviation or number (%). MHNO, metabolically healthy non-obese; MUHNO, metabolically unhealthy non-obese; MHO, metabolically healthy obese; MUHO, metabolically unhealthy obese; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, Fasting blood glucose; HDL-C, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol; HOMA-IR, homeostasis model assessment-insulin resistance; Hs-CRP, high-sensitivity C-reac- tive protein; BMD, bone mineral density; NA, not available. *P-value for one-way analysis of variance among the four groups. †,‡,§,∥No differences between the groups with same footnotes in post-hoc analyses.
Min-Ji Kim, et al. Bone Mineral Density According to Obesity and Metabolic Health Status
Korean Journal of Family Practice
KJFP
연구를 대상으로 시행한 메타분석의 결과와 일치했다. 근육은 기계 적 부하 이외에도 뼈에 순간적인 스트레인을 주어 “mechanostat the- ory”에 따라 골형성을 자극하고,22) 근육량이 부분적으로 근력 증가 를 매개로 골밀도에 영향을 줌으로써,23) 근육량이 골량을 유지하고 개선하는데 중요한 역할을 하는 것으로 생각된다.
대사증후군과 골밀도와의 연관성에 대해서는 아직 결론이 불명 확하다. 이러한 연구 결과들의 차이는 연구 대상자, 대사증후군의 진단기준, 공변수 보정 등과 같은 연구 방법의 차이에 의해 영향을 받았을 것으로 생각된다. 본 연구에서는 각각의 대사적 위험요인들 과 요추 골밀도 사이에 대부분 연관성이 없거나 낮았다. 공복 인슐 린 및 인슐린 저항성의 경우 남녀 모두에서 요추 골밀도와 양의 상 관관계를 보였는데, 이는 고인슐린혈증이 IGF-1수용체에 직접적으 로 작용하여 골형성을 자극하거나, 성호르몬 결합 글로불린을 억제 함으로써 골소실의 예방적 역할을 하는 유리 성호르몬을 증가시키 기 때문일 것으로 생각되며,24,25) 이는 2형 당뇨병에서의 높은 골밀도 를 일부 뒷받침하는 근거가 되어오기도 했다.26) 여성에서 공복혈당 이 골밀도와 양의 연관성을 보인 것도 고인슐린혈증이 부분적으로 기여했을 것으로 생각된다.27) 그러나 일부 연구에서는 체질량지수 를 보정한 후 고인슐린혈증이나 인슐린 저항성과 골밀도와의 양의 연관성이 약해지거나 사라졌고,25) 결국 이 또한 인슐린 저항성을 가 진 사람들에서의 체지방 증가가 체중 부하를 통해 골밀도에 영향을 준 결과일 수 있다. 다른 대사 지표로는 중성지방이 여성에서 양의 상관관계를 보였다. 이는 Dennison 등28)이 영국에서 시행한 코호트 연구 결과와 일치하며, 중성지방이 높을수록 요추 골밀도가 높았으 나 체지방율을 보정한 후에는 상관성이 낮아진 것으로 보아 지질과 골밀도의 연관성에 있어 지방세포가 교란역할을 하는 것으로 추정 하였다. 본 연구에서 일부 대사적 지표들이 부분적으로 골밀도와 연 관성이 있었으나, 전체 대사적 이상들이 복합적으로 골밀도에 미치 는 영향은 미미했다. 대사 증후군과 골밀도와의 역의 상관관계를 주 장한 연구들은 복부 비만을 주요인자로 제시하고 있다.9,11,12,14) 내장지
방에서 전염증성 사이토카인들을 분비하고, 이로 인한 만성적인 낮 은 염증 상태가 골흡수에 중요한 역할을 한다는 것이다.29) 그러나 본 연구에서는 염증상태를 반영하는 지표인 hs-CRP와 요추 골밀도 사 이에 연관성이 없었으며, 기존의 연구들에서 체질량지수 보정 후 복 부둘레와 골밀도가 역의 상관관계를 보인 것과 달리 체질량지수 보 정 후 복부 둘레와 골밀도 사이에 연관성이 없었다(데이터 제시하지 않음). 그러나 확인 가능한 염증지표가 제한적이고, 복부둘레가 내 장지방을 정확히 반영할 수 없다는 한계가 있다. 결론적으로 대사상 태와 골밀도는 연관성이 낮으며, 연관성이 존재한다 하더라도 비만 의 골밀도 보호 효과가 훨씬 더 큰 것으로 생각된다.
본 연구의 강점은 대사적으로 건강한 비만이라는 개념을 이용하 여, 대사적 건강과 골밀도와의 연관성을 밝힘으로써 골밀도 개선을 위해 대사 상태 개선에 초점을 맞춘 중재의 필요성 여부를 확인하고 자 한 점이다. 또한 한국인의 대사 상태와 골밀도의 연관성에 관한 기존연구들이 주로 여성을 대상으로 하여 남성을 대상으로 한 연구 가 상대적으로 미흡하였고,7,8) 특히 대사이상과 골다공증에 취약한 60세 이상의 고령자를 대상으로 한 연구는 거의 이루어지지 않았다 는 점에서 의미가 있다.
본 연구의 제한점은, 검진센터 수진자들을 대상으로 하여, 일반인 구에 비해 사회 경제 수준이 높고, 건강한 사람들의 비율이 높았을 수 있다. 두 번째로, 요추 부위의 골밀도만을 평가하여 다른 부위의 골밀도와의 연관성은 확인할 수 없었다. 그러나 요추골이 해면골의 비율이 높아 대사적으로 더 활동적이고 체내 환경 및 폐경기 변화 를 민감하게 잘 반영하여, 대사 상태에 따른 골밀도의 변화를 평가 하기에 보다 적절한 부위였다고 생각된다. 세 번째로, 여성의 경우 폐 경기간에 관한 정보가 수집되지 않았으나, 한국 여성의 평균 폐경 나이가 49.7세이고 60세 이상 성인을 연구 대상으로 하였으므로 폐 경 상태인 대상자의 비율이 높았을 것으로 생각된다. 마지막으로, 단 면연구로 인과관계를 밝히기에는 어려움이 있었으며, 임상적으로 골절 위험을 예측하는데 있어, 골밀도에 더해 골질이나 강도 등을 함 Table 4. Mean lumbar spine BMD among the four metabolic health and obesity status
Women (n=550) Men (n=748)
MHNO (n=170)
MUHNO (n=200)
MHO (n=56)
MUHO
(n=124) P-value* MHNO (n=339)
MUHNO (n=172)
MHO (n=93)
MUHO
(n=144) P-value* Unadjusted 0.919±0.150† 0.925±0.155† 1.000±0.130‡ 0.997±0.196‡ 0.000 1.106±0.175† 1.134±0.199† 1.236±0.196‡ 1.222±0.190‡ 0.000 Model 1 0.943±0.014 0.943±0.012 0.958±0.024 0.954±0.019 0.953 1.141±0.012 1.156±0.014 1.176±0.022 1.154±0.019 0.607 Model 2 0.939±0.014 0.944±0.012 0.954±0.024 0.960±0.019 0.892 1.142±0.012 1.155±0.015 1.176±0.022 1.153±0.019 0.590 Values are presented as mean±standard deviation.
BMD, bone mineral density; MHNO, metabolically healthy non-obese; MUHNO, metabolically unhealthy non-obese; MHO, metabolically healthy obese; MUHO, meta- bolically unhealthy obese.
Model 1 adjusted for body mass index. Model 2 adjusted for Model 1 plus age, smoking, alcohol consumption, physical activity.
*P-value by analysis of variance or analysis of covariance as appropriate. †,‡Same letters indicate no statistical significance based on Bonferroni’s multiple comparison.
김민지 외. 비만과 대사적 건강 상태에 따른 요추 골밀도와의 관계 Korean Journal of Family Practice
KJFP
께 고려한 연구들이 필요할 것이다.
결론적으로, 본 연구 결과 비만의 과체중은 골다공증 예방에 중 요하나 대사적 상태는 임상적으로 의미 있는 영향을 미치지 않는 것 으로 추정된다.
요 약
연구배경:
비만은 골다공증의 보호인자로 생각되어 왔다. 그러나 비만은 대사 이상을 초래하며, 이러한 대사 이상이 골밀도를 악화시 킬 수 있다는 보고가 있으나 아직 결론에 논란이 있다. 본 연구는 대 사적으로 건강한 비만 형태에 따른 골밀도를 비교하고, 대사 이상과 비만이 골밀도에 미치는 영향을 분석하고자 한다.방법:
2010년 1월부터 2013년 12월까지 강북삼성병원 종합검진센터 방문자 중 요추 골밀도 검사를 시행한 60세 이상 성인 1,298명(여성 550명, 남성 748명)을 대상으로 단면 연구를 시행하였다. 요추 골밀도 는 이중 에너지 방사선 흡수 계측법을 이용하여 측정하였다. 비만은 체질량지수가 25 이상인 경우로 정의하였고, 대사적으로 건강한 상 태는 다음 위험요인들 중 2가지 미만을 만족하는 경우로 정의하였 다: 고혈압, 고혈당, 고중성지방혈증, 저고밀도지단백콜레스테롤혈 증. 비만과 대사적 건강 상태에 따라 네 군으로 나누어 분석하였다:metabolically healthy non-obese (MHNO), metabolically unhealthy non-obese (MUHNO), metabolically healthy obese (MHO), metaboli- cally unhealthy obese (MUHO).
결과:
평균 요추 골밀도를 비교하였을 때, 비만하지 않은 MHNO, MUHNO군들에 비해 비만한 MHO, MUHO군들에서 더 높았으나, 대사 상태가 다른 MHNO와 MUHNO (0.919±0.150 vs. 0.925±0.155, P=1.000 in women; 1.106±0.175 vs. 1.134±0.199, P=1.000 in men), MHO 와 MUHO (1.000±0.130 vs. 0.997±0.196, P=1.000 in women; 1.236±0.196 vs. 1.222±0.190, P=0.662 in men) 사이에는 통계적으로 유의한 차이가 없었다. 체질량지수를 포함한 교란변수를 보정한 후에는 모든 군 사 이의 연관성이 사라졌다.결론:
비만의 과체중은 골다공증 예방에 중요하나 대사적 상태는 임상적으로 의미 있는 영향을 미치지 않는 것으로 추정된다.중심단어:
비만; 대사적으로 건강한 비만; 대사증후군; 골밀도REFERENCES
1. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harri- son’s principles of internal medicine. Lindsay R, Cosman F, Osteoporosis.
19th ed. New York: McGraw-Hill Companies; 2016. p. 2488.
2. Park EJ, Joo IW, Jang MJ, Kim YT, Oh K, Oh HJ. Prevalence of osteoporosis in the Korean population based on Korea National Health and Nutrition Examination Survey (KNHANES), 2008-2011. Yonsei Med J 2014; 55:
1049-57.
3. Felson DT, Zhang Y, Hannan MT, Anderson JJ. Effects of weight and body mass index on bone mineral density in men and women: the Framingham study. J Bone Miner Res 1993; 8: 567-73.
4. Edelstein SL, Barrett-Connor E. Relation between body size and bone min- eral density in elderly men and women. Am J Epidemiol 1993; 138: 160-9.
5. Cao JJ. Effects of obesity on bone metabolism. J Orthop Surg Res 2011; 6: 30.
6. Ye C, Xu M, Wang S, Jiang S, Chen X, Zhou X, et al. Decreased bone mineral density is an independent predictor for the development of atherosclerosis:
a systematic review and meta-analysis. PLoS One 2016; 11: e0154740.
7. Zhou J, Zhang Q, Yuan X, Wang J, Li C, Sheng H, et al. Association between metabolic syndrome and osteoporosis: a meta-analysis. Bone 2013; 57: 30-5.
8. Xue P, Gao P, Li Y. The association between metabolic syndrome and bone mineral density: a meta-analysis. Endocrine 2012; 42: 546-54.
9. Kim HY, Choe JW, Kim HK, Bae SJ, Kim BJ, Lee SH, et al. Negative associa- tion between metabolic syndrome and bone mineral density in Koreans, es- pecially in men. Calcif Tissue Int 2010; 86: 350-8.
10. Jeon YK, Lee JG, Kim SS, Kim BH, Kim SJ, Kim YK, et al. Association be- tween bone mineral density and metabolic syndrome in pre- and post- menopausal women. Endocr J 2011; 58: 87-93.
11. Hwang DK, Choi HJ. The relationship between low bone mass and meta- bolic syndrome in Korean women. Osteoporos Int 2010; 21: 425-31.
12. Kim T, Park S, Pak YS, Lee S, Lee EH. Association between metabolic syn- drome and bone mineral density in Korea: the Fourth Korea National Health and Nutrition Examination Survey (KNHANES IV), 2008. J Bone Miner Metab 2013; 31: 652-62.
13. Kim H, Oh HJ, Choi H, Choi WH, Lim SK, Kim JG. The association be- tween bone mineral density and metabolic syndrome: a Korean population- based study. J Bone Miner Metab 2013; 31: 571-8.
14. Kim YH, Cho KH, Choi YS, Kim SM, Nam GE, Lee SH, et al. Low bone mineral density is associated with metabolic syndrome in South Korean men but not in women: The 2008-2010 Korean National Health and Nutri- tion Examination Survey. Arch Osteoporos 2013; 8: 142.
15. von Muhlen D, Safii S, Jassal SK, Svartberg J, Barrett-Connor E. Associations between the metabolic syndrome and bone health in older men and wom- en: the Rancho Bernardo Study. Osteoporos Int 2007; 18: 1337-44.
16. Rhee EJ, Seo MH, Kim JD, Jeon WS, Park SE, Park CY, et al. Metabolic health is more closely associated with coronary artery calcification than obesity.
PLoS One 2013; 8: e74564.
17. Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC.
Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetolo- gia 1985; 28: 412-9.
18. James WP, Chunming C, Inoue S. Appropriate Asian body mass indices?
Obes Rev 2002; 3: 139.
19. Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005; 112: 2735-52.
20. Lloyd JT, Alley DE, Hawkes WG, Hochberg MC, Waldstein SR, Orwig DL.
Min-Ji Kim, et al. Bone Mineral Density According to Obesity and Metabolic Health Status
Korean Journal of Family Practice
KJFP
Body mass index is positively associated with bone mineral density in US older adults. Arch Osteoporos 2014; 9: 175.
21. Ho-Pham LT, Nguyen UD, Nguyen TV. Association between lean mass, fat mass, and bone mineral density: a meta-analysis. J Clin Endocrinol Metab 2014; 99: 30-8.
22. Frost HM. Bone “mass” and the “mechanostat”: a proposal. Anat Rec 1987;
219: 1-9.
23. Schoenau E, Neu MC, Manz F. Muscle mass during childhood--relationship to skeletal development. J Musculoskelet Neuronal Interact 2004; 4: 105-8.
24. Wakasugi M, Wakao R, Tawata M, Gan N, Koizumi K, Onaya T. Bone min- eral density measured by dual energy x-ray absorptiometry in patients with non-insulin-dependent diabetes mellitus. Bone 1993; 14: 29-33.
25. Dennison EM, Syddall HE, Aihie Sayer A, Craighead S, Phillips DI, Cooper C. Type 2 diabetes mellitus is associated with increased axial bone density in
men and women from the Hertfordshire Cohort Study: evidence for an in- direct effect of insulin resistance? Diabetologia 2004; 47: 1963-8.
26. Ma L, Oei L, Jiang L, Estrada K, Chen H, Wang Z, et al. Association between bone mineral density and type 2 diabetes mellitus: a meta-analysis of obser- vational studies. Eur J Epidemiol 2012; 27: 319-32.
27. Barrett-Connor E, Kritz-Silverstein D. Does hyperinsulinemia preserve bone? Diabetes Care 1996; 19: 1388-92.
28. Dennison EM, Syddall HE, Aihie Sayer A, Martin HJ, Cooper C. Lipid pro- file, obesity and bone mineral density: the Hertfordshire Cohort Study. QJM 2007; 100: 297-303.
29. Manolagas SC, Jilka RL. Bone marrow, cytokines, and bone remodeling.
Emerging insights into the pathophysiology of osteoporosis. N Engl J Med 1995; 332: 305-11.