20
책임저자: 조영업, 인천시 중구 신흥동 3가 7-206, 400-711, 인하대학교병원 외과 Tel: 032-890-2738, Fax: 032-890-3097, E-mail: [email protected]
접수일:2010년 1월 3일, 게재승인일:2010년 3월 8일
본 논문의 요지는 2008년 제60차 대한외과학회 추계학술대회에서 구연 발표되었음.
이 논문은 인하대학교의 연구비 지원에 의하여 연구되었음.
감시림프절 전이 양성인 유방암 환자에서 비감시림프절 전이 예측인자 및 예측체계의 비교 분석
인하대학교 의학전문대학원 외과학교실, 1병리학교실
박재영ㆍ박근명ㆍ박정미ㆍ이강연ㆍ문연희ㆍ김세중ㆍ김준미
1ㆍ조영업ㆍ김장용 최윤미ㆍ최선근ㆍ허윤석ㆍ이건영ㆍ안승익ㆍ홍기천ㆍ신석환ㆍ김경래
Predicting Factors of Nonsentinel Lymph Node Metastasis in Breast Cancer Patients with Sentinel Lymph Node Metastasis
Jae Young Park, M.D., Keun Myoung Park, M.D., Jeong Mi Park, M.D., Kang Yeun Lee, M.D., Youn Hee Moon, M.D., Sei Joong Kim, M.D., Joon Mee Kim, M.D.1, Young Up Cho, M.D.,
Jang Yong Kim, M.D., Yun-Mee Choe, M.D., Sun Keun Choi, M.D., Yoon-Seok Heo, M.D., Keon-Young Lee, M.D., Seung-Ik Ahn, M.D., Kee Chun Hong, M.D.,
Seok-Hwan Shin, M.D., Kyung Rae Kim, M.D.
Departments of Surgery and 1Pathology, Inha University School of Medicine, Incheon, Korea
Purpose: The purpose of this study was to investigate the predictors of nonsentinel lymph node (NSLN) metastasis in breast cancer and to evaluate the usefulness of the scoring systems and nomograms.
Methods: In this analysis, we reviewed the clinicopathologic features of 70 patients who had undergone sentinel lymph node (SLN) biopsy and axillary lymph node dissection. The clinical features of patients, histologic parameters and hormonal receptor status of primary tumor and histopathologic features of SLN metastasis were noted retrospectively. Furthermore, the receiver operating characteristic (ROC) curve was drawn and the area under the ROC curve (AUC) was calculated to assess the discriminative power of the scoring systems and nomograms.
Results: The metastatic tumor size in SLN (P<0.001), extracapsular invasion (P=0.002), percentage of positive SLNs among the removed SLNs (P=0.011), primary tumor size (P=0.038) were associated significantly with NSLN metastasis, statistically, in univariate analysis. Based on multivariate logistic regression, the metastatic tumor size was the only prognostic factor of NSLN metastasis (P=0.012). The AUC of Memorial Sloan-Kettering Cancer Center scoring system was greater than other systems, significantly (P=0.004).
Conclusion: We have shown in this study that it would be possible to predict NSLN status based on the metastatic tumor size in SLN. Although the significance was not achieved in multivariate analysis, the size of primary tumor, extracapsular invasion of metastasis in SLN, percentage of positive SLNs among the removed SLNs had the potential to be a predictive factor of NSLN metastasis. MSKCC scoring system appears to be more effective and accurate than other scoring systems for selecting patients for whom axillary lymph node dissection can be avoided.
(J Korean Surg Soc 2010;79:20-26)
Key Words: Breast cancer, Sentinel lymph node, Metastasis, Predictor, Scoring system 중심 단어: 유방암, 감시림프절, 전이, 예측인자, 점수체계
서 론
유방암의 치료에 있어서 Fisher 등(1)과 Veronesi 등(2)이 보존적 유방절제술과 변형근치적 유방절제술 간에 전체 생 존율과 무병 생존율에 유의한 차이가 없음을 보고한 이후 로 근래에는 보존적 유방절제술이 활발히 시행되고 있다.
유방암에 대한 수술 범위가 축소됨에 따라 액와부 수술에 도 Giuliano 등(3)이 유방암에 대한 감시림프절 생검의 적용 을 처음 보고한 이래 액와림프절 절제술을 대체할 수 있는 방법으로 제시하였고, 현재 많은 기관에서 감시림프절이 전이 양성인 경우에만 추가의 액와림프절 절제술을 시행하 고 있고 이것이 표준 치료가 되고 있다. 하지만 여러 연구 결과들을 보면, 감시림프절 전이 양성인 환자의 40∼70%는 비감시림프절(감시림프절을 제외한 동측의 액와림프절)에 전이가 없는 것으로 보고된다.(4-6) 따라서 불필요한 액와 림프절 절제술을 시행 받은 연구 결과들이 보고되고 있 어,(5-8) 추가적인 액와림프절 절제술의 필요성이 의문시 되고 있는 실정이다. 하지만 불행히도, 전이 양성인 감시림 프절을 가진 환자에서, 액와림프절 절제술을 시행하지 않 을 수 있는 신뢰할 만한 예측인자는 정립된 것이 없다. 이에 Louisville Breast Sentinel Lymph Node Study의 Chagpar 등 (9), M. D. Anderson Cancer Center의 Hwang 등(10), Tenon Hospital의 Barranger 등(11)과 Memorial Sloan-Kettering Can- cer Center (MSKCC)의 Van Zee 등(12)은, 감시림프절 전이 양성인 환자의 임상 병리학적 여러 인자를 비교 분석하여 비감시림프절 전이가 있을 확률을 예측하는 점수체계 (scoring system)를 발표하였고, 국내외 여러 center에서 이 점수체계를 임상에 적용시키거나 응용하여 각 center별 점 수체계를 독자적으로 발표하기도 하였다. 본 연구에서는 액와부의 감시림프절이 양성인 환자의 여러 임상 조직학적 인 요인을 분석하여 비감시림프절 전이에 대한 예측인자를 찾아 보고, 이미 보고되어 있는 비감시림프절 전이 예측에 사용되고 있는 점수체계의 예측력을 비교해 보고자 한다.
방 법
1) 연구 대상
2005년 5월부터 2008년 3월까지 감시림프절 생검술을 시 행한 유방암 환자 254명 중, 2005 American Society of Clinical Oncology recommendations(13)에 따른 감시림프절
생검의 적응 대상이 되지 않는 70명을 제외한 184명의 환자 중 감시림프절 전이 양성이 나와 액와림프절 절제술을 시 행한 환자 70예를 대상으로 연구하였다. 액와림프절 절제 술은 level II를 표준으로 하였다.
2) 감시림프절 생검의 수기
수술 당일에 500 micro-Ci의 99mTc-phytate를 환측 유방의 원발종양 방향의 유륜 경계에 피하 주입 후 전후방, 측방 림프관조영술을 시행하여 감시림프절을 우선 확인하였다.
수술 직전 indigocarmine 용액 2 ml를 유륜의 상, 하 및 외측 에 나누어 피내 주입하여 림프액 배액 과정을 육안으로 확 인하여 감시림프절을 찾아내는 데 도움이 되도록 하였다.
암종이 상외측에 존재할 시에는 암종의 주변 실질에도 주 입하였다. 수술 중 감마 탐침자를 이용하여 감시림프절을 찾아낸 뒤 동결절편을 시행하여 감시림프절이 양성인 환자 에서 액와림프절 곽청술을 시행하였다. 수술 중 찾아낸 감 시림프절은 동결절편 검사시, hematoxylin & eosin 염색으로 전이 여부를 확인하였고 필요시 cytokeratin 염색을 시행하 였다.
3) 결과 분석
대상 환자들을 비감시림프절이 양성인 군과 음성인 군으 로 나누어 연령, 폐경 여부, 원발종양의 조직학적 분류, 크 기, 등급, 호르몬 수용체 발현 여부, 림프혈관계 침습 여부, 다중심성 여부, 양성인 감시림프절의 수, 음성인 감시림프 절의 수, 총 감시림프절 개수 중 양성인 림프절의 비율(%), 감시림프절에 전이된 종양의 크기, 감시림프절 주변으로의 피막외 침습 유무에 대하여 두 군 간에 어떠한 임상병리학 적인 차이가 있는지 알아보았다. 또한 타 연구자들에 의해 만들어진 비감시림프절 예측체계 중 Louisville Breast Sentinel Lymph Node Study, M. D. Anderson Cancer Center, Tenon Hospital과 MSKCC의 예측체계에 본 연구 대상 환자 들의 데이터를 입력하여 나온 결과 점수를 분석하여, re- ceiver operating characteristic (ROC) curve와 area under ROC curve (AUC)를 구하여 예측력을 비교하였다. 통계는 SPSS 프로그램(SPSS Inc., Chicago, IL, USA)을 이용하여 chi- square test, student t-test와 로지스틱 회귀분석을 시행하였고 유의수준을 P<0.05로 하였다.
Table 1. Comparison of preoperative clinicopathologic character- istics of patients and primary tumor between 2 groups;
NSLN*(+) and NSLN(−) patients NSLN(−) (%) (n=39)
NSLN(+)
(%) (n=31) P-value
Age (years) 0.786
Mean±SD† 49.2±11.1 49.9±10.1
Menopause 0.335
Yes 25 (64.1) 16 (51.6)
No 14 (35.9) 15 (48.4)
Pathologic type 0.368
Ductal 34 (87.2) 30 (96.8)
Lobular 0 1 (3.2)
Tubular 1 (2.6) 0
Cribriform 1 (2.6) 0
Apocrine 2 (5.1) 0
Metaplastic 1 (2.6) 0 Tumor size (cm)
Mean±SD 2.07±1.18 1.91±0.67 0.158
≤10 mm (T1a, T1b) 8 (20.5) 1 (3.2) 0.038 >10 mm (T1c, T2) 31 (79.5) 30 (96.8)
Histologic grade 0.601
1 10 (25.6) 7 (22.6)
2 19 (48.7) 14 (45.2)
3 10 (25.6) 10 (32.3)
Nuclear grade 0.178
1 8 (20.5) 4 (12.9)
2 24 (61.5) 16 (51.6)
3 7 (17.9) 11 (35.5)
Tumor location 0.235
Upper outer 22 (56.4) 18 (58.1) Lower outer 4 (10.3) 5 (16.1) Upper inner 8 (20.5) 1 (3.2) Lower inner 1 (2.6) 2 (6.5)
Central 4 (10.3) 5 (16.1)
LV invasion‡ 0.071
Present 23 (58.9) 25 (80.6)
Absent 16 (41.1) 6 (19.4)
Multicentricity 0.171
Present 3 (7.7) 6 (19.4)
Absent 36 (92.3) 25 (80.6)
Hormone receptor status 0.561
ER§(+), PR∥(−) 5 (12.8) 5 (16.1) ER(−), PR(+) 3 (7.7) 4 (12.9) ER(+), PR(+) 21 (53.8) 18 (58.1) ER(−), PR(−) 10 (25.6) 4 (12.9)
HER2¶/neu expression 0.391
C-erb B-2(+) 7 (17.9) 9 (29.0) C-erb B-2(−) 32 (82.1) 22 (70.9)
*NSLN = nonsentinel lymph node; †SD = standard deviation; ‡LV invasion = lymphovascular invasion; §ER = estrogen receptor; ∥PR
= progesteron receptor; ¶HER2 = human epidermal growth factor receptor 2.
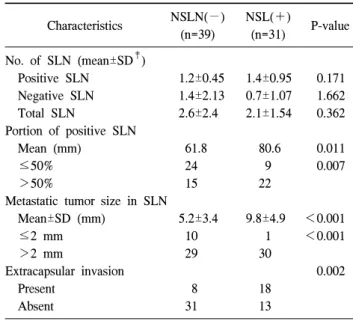
Table 2. Comparison of SLN* status between 2 groups; NSLN† (+) and NSLN(−) patients
Characteristics NSLN(−) (n=39)
NSL(+)
(n=31) P-value No. of SLN (mean±SD‡)
Positive SLN 1.2±0.45 1.4±0.95 0.171
Negative SLN 1.4±2.13 0.7±1.07 1.662
Total SLN 2.6±2.4 2.1±1.54 0.362
Portion of positive SLN
Mean (mm) 61.8 80.6 0.011
≤50% 24 9 0.007
>50% 15 22
Metastatic tumor size in SLN
Mean±SD (mm) 5.2±3.4 9.8±4.9 <0.001
≤2 mm 10 1 <0.001
>2 mm 29 30
Extracapsular invasion 0.002
Present 8 18
Absent 31 13
*SLN = sentinel lymph node; †NSLN = nonsentinel lymph node;
‡SD = standard deviation.
결 과
대상 환자들의 평균 연령은 49.5세(±1.2)였으며, 폐경인 환자는 전체 70명 중 41명(58.6%)이었다. 원발종양을 조직 학적으로 분류해 보면 64예(91%)가 침윤성 관암으로 가장 많았고, 종양의 크기는 평균 2.0 cm (0.3∼4.5)로 T 병기는 T1이 41예(58.6%), T2가 29예(41.4%)였다. 총 70예의 환자 중 감시림프절에만 전이가 있고, 나머지 액와림프절에는 종양의 전이가 없었던 환자는 39명(55.7%)이었고, 환자당 절제된 감시림프절은 평균 2.38개(1∼15)였다.
대상 환자의 임상적인 요인과 원발종양의 병리학적 요소 들을 분석한 결과, 환자의 나이, 폐경 여부, 위치, 병리학적 분류, 등급, 림프혈관계 침습 여부, 호르몬 수용체 발현 여 부에 대해서는 비감시림프절 전이 양성군과 음성군 간에 통계적으로 유의한 차이를 보이지 않았다(Table 1). 비감시 림프절 전이 여부에 관련될 것으로 생각되는 감시림프절에 대한 요인들을 분석한 결과, 원발종양의 크기(P=0.038), 감 시림프절에 전이된 종양의 크기(P<0.001), 감시림프절 주 변으로의 피막외 침습 여부(P=0.002), 총 감시림프절 개수 중 양성인 림프절의 비율(P=0.011)이 단변량 분석에서 통계 학적으로 의미가 있었다(Table 2). 이 중 다변량 분석에서 의미 있는 변수는 감시림프절에 전이된 종양의 크기였다 (P=0.012) (Table 3). 특히 감시림프절에 미세전이가 있는 환
Table 3. Multivariate analysis (logistic regression test) of variables predicting sentinel lymph node-only disease
Variables β-coefficient Odds ratio 95% confidence interval P-value
Tumor size >10 mm 1.558 4.750 0.454∼49.706 0.193
Portion of positive SLN* >50% 0.823 2.278 0.708∼7.332 0.167
Extracapsular invasion 0.224 1.251 0.312∼5.012 0.751
Metastasis size in SLN >2 mm 2.411 11.143 1.688∼73.572 0.012
*SLN = sentinel lymph node.
Table 4. Variables of scoring systems that considered predictable factors for metastasis to nonsentinel lymph node
Scoring system Variables
Louisville Number of positive SLN*, proportion of involved SLNs among all removed SLNs, tumor size M. D. Anderson Tumor size, size of the largest SLN metastasis, LVI† status
Tenon Tumor size, macro or micrometastasis in SLN, proportion of involved SLNs among all removed SLNs MSKCC‡ Tumor size, grade, number of (+) SLNs, number of (−) SLNs, method of detection of SLNs, ER§ status,
LVI status, multifocality of the tumor
*SLN = sentinel lymph node; †LVI = lymphovascular invasion; ‡MSKCC = Memorial Sloan-Kettering Cancer Center; §ER = estrogen receptor.
Fig. 1. The receiver operating characteristic curves (ROC) and area under ROC curve (AUC) of scoring systems and nomogram.
Table 5. The area under ROC curve* for training and validation datasets compared with other published scoring systems and nomogram applied to the validation dataset
Scoring system AUC† 95% confidence
interval P-value
Louisville 0.642 0.511∼0.773 0.043
M. D. Anderson 0.606 0.474∼0.738 0.130
Tenon 0.673 0.547∼0.799 0.013
MSKCC‡ 0.700 0.577∼0.823 0.004
*ROC curve = reciever operating characteristic curve; †AUC = area under ROC curve; ‡MSKCC = Memorial Sloan-Kettering Cancer Center.
자 11예 중 비감시림프절에 전이가 발견된 환자는 1명 (9.1%)이었고, 거대전이가 있는 59예 중 비감시림프절에 전 이가 있는 환자는 30명(50.9%)으로 두 군 간에 현격한 차이 를 보였다. 총 70명의 환자 중에 감시림프절 내 전이가 미세 전이이고, 감시림프절 주변으로의 피막외 침습이 없으며, 전이 양성인 감시림프절 비율이 50% 이하인 경우는 총 10 예였고, 10예 모두 비감시림프절 전이 음성을 나타냈다. 림 프혈관계 침습의 경우, 통계적 유의성은 확보하지 못했지 만(P=0.071), 림프혈관계 침습이 있는 경우 48예 중 25예 (52.1%)가 비감시림프절 전이 양성을 나타냈고, 침습이 없
는 경우 22예 중 6예(27.3%)가 비감시림프절 전이 양성을 보여, 림프혈관계 침습이 있는 경우가 없는 경우보다 1.9배 높은 비감시림프절 전이 양성률을 보였다.
타 연구자들에 의해 만들어진 예측체계에서 비감시림프 절 전이를 예측하는데 사용된 변수는 그 수와 종류가 다양 하다(Table 4). 본 연구 대상 환자들의 데이터를 각각의 예 측체계에 입력하여 나온 점수를 분석하여 ROC curve를 그 려본 결과(Fig. 1), MSKCC의 nomogram이 네 가지 중 통계 적으로 가장 AUC 면적이 넓어(P=0.004) 기타 체계에 비해 좋은 예측력을 나타냈다(Table 5).
고 찰
유방암의 치료에 있어 감시림프절 생검술은 액와림프절 전이 상태를 나타내는 표준 술식으로 받아들여지고 있다.
감시림프절 생검술의 가장 큰 효용성은, 액와림프절 절제 술에 의한 합병증을 감소시키면서 액와림프절 절제술을 시 행한 환자와 동등한 치료 효과를 나타내는데 있다.(14) 유 방암의 조기 진단율이 높아짐에 따라 림프절 전이 양성인 환자의 비율은 감소하고 있지만, 현재까지 감시림프절에 전이가 있는 환자에서는 액와림프절 절제술이 표준 치료로 시행되고 있다. 본 연구에서도 감시림프절 전이 양성으로 액와림프절 절제술을 시행 받은 환자 중에 44.3% (70명 중 31명)만이 비감시림프절 전이가 있었다. 이것은 감시림프 절 전이 양성인 환자의 과반수가 불필요한 액와림프절 절 제술을 시행 받았다는 것을 입증하는 것으로 보고된 연구 들과 비슷한 결과를 나타낸 것이다.(5-8)
본 연구에서 비감시림프절 전이에 관여하는 가장 유의한 인자는 감시림프절 내 전이된 종양의 크기였다. 단변량 분 석(P<0.001)과 다변량 분석(P=0.012)에서 모두 통계적으로 유의하게 미세전이 환자군과 거대전이 환자군 간의 비감시 림프절 전이율(9.1% vs. 50.9%)에서 차이를 보였다. 감시림 프절 전이의 크기가 2 mm 이하인 미세전이인 경우 추가로 액와림프절 절제술을 시행해야 하는지는 아직도 논란이 있 다. Langer 등(15)과 Liang 등(16)은 감시림프절 생검술을 받 은 환자들의 전향적 연구에서, 미세전이가 있더라도 액와 부 재발이나 원격전이가 보이지 않았다고 보고하며, 감시 림프절에 미세전이가 있는 환자에서 액와림프절 절제술이 불필요하다고 하였다. 하지만 Barranger 등(17)은 감시림프 절 내 미세전이가 있는 환자의 14%에서 비감시림프절 전이 를 보고하였고, 그 외의 다른 여러 연구 결과(10,18)에서도 10% 내외의 비감시림프절 전이율을 나타내고 있다. 또 Gipponi 등(19)에 의하면 감시림프절에 미세전이만 있는 환 자에서도 일차 종양의 크기가 크고 림프혈관계 침습이 있 는 경우 비감시림프절 전이가 있을 수 있음을 보고하였다.
본 연구에서는 미세전이가 있는 환자 11예 중 1예에서 비감 시림프절 전이가 있는 것으로 나타났고, 이것 또한 감시림 프절에 미세전이가 있는 환자에서 액와림프절 절제술을 필 수적으로 시행해야 한다는 근거라 할 수 있다.
기존의 연구에서 감시림프절 내 전이 크기 이외에 비감 시림프절 전이의 예측인자로 보고된 것으로는, 원발종양의
크기, 감시림프절 피막외 침습 유무, 원발종양 주위의 림프 혈관계 침윤 등이 있다. Chu 등(20)은 종양의 T 병기가 T1에 서 T2로 올라갈수록 비감시림프절 전이율이 13%에서 38%
까지 증가한다고 보고하였고, Viale 등(21)도 2 cm 이상의 종양에서는 비감시림프절 전이가 유의하게 증가한다고 보 고하였다. 하지만 본 연구에서는 1 cm로 종양의 크기를 나 누어 비교한 결과, 비감시림프절 전이와 통계적으로 유의 한 상관관계를 나타내었다.
감시림프절 피막외 침습 유무에 따른 비감시림프절 전이 에서는 다변량 분석에서 통계적으로 유의하지는 않지만(P=
0.751) 단변량 분석에서 통계적 유의성을 가지며(P=0.002) 피막외 침습이 있는 경우에 비감시림프절 전이가 더 잘 되 는 것으로 나왔다(26예 중 18예, 69.2%). 이는 데이터 분석 결과, 피막외 침습이 있는 경우 26예가 모두 감시림프절 내 거대전이를 가지고 있는 것으로 나와 피막외 침습 여부가 독립적인 요소로 작용하지 못한 것으로 생각된다. Stitzen- berg 등(22)은 감시림프절 주위 피막외 침습이 있는 종양은 좀더 공격적인 성향을 나타내고 액와림프절로의 침습경향 을 높인다고 보고하였고, 본 연구 대상 환자들 역시 비슷한 결과를 나타내어 감시림프절 피막외 침습이 비감시림프절 전이 예측인자로서 가능성을 제시하였다.
Schrenk 등(23)과 Callejo 등(24)의 연구에서는 원발종양의 림프혈관계 침윤이 비감시림프절 전이에 의미 있는 예측인 자로 소개되고 있으나 본 연구에서는 통계적으로 유의한 차이를 보이지는 못했다(P=0.071). 하지만 림프혈관계 침윤 이 있는 경우 52.1% (48예 중 25예)가 비감시림프절 전이를 보여, 림프혈관계 침윤이 없는 경우(27.3%, 22예 중 6예)보 다 높은 전이율을 나타내는 상관관계를 보여주었다.
비교 분석한 4개의 예측체계(Louisville Breast Sentinel Lymph Node Study, the M.D. Anderson Cancer Center, Tenon Hospital, MSKCC) 중에서는 MSKCC의 예측체계가 비감시 림프절의 전이에 대한 가장 큰 예측력을 나타내었다.
결 론
본 연구에서 다변량 분석 결과 감시림프절내 전이 크기 가 비감시림프절의 예측인자로 나타났고, 원발종양의 림프 혈관 침윤, 감시림프절 피막외 침습, 총 감시림프절 개수 중 전이 양성 림프절의 비율은 통계적인 유의성은 확보하지 못하였으나 단변량 검사에서의 유의성 확보와 데이터 간의 상당한 상관관계로서 예측인자로서의 가능성을 나타내었
다. 이로써 감시림프절 생검술 후 감시림프절의 병리학적 소견을 통해 비감시림프절의 전이 유무를 예측하여 액와림 프절의 절제를 피할 수 있을 가능성을 보여주었다. 비교 분 석한 4개의 예측체계 중에서는 MSKCC의 예측체계가 비감 시림프절의 전이에 대한 가장 큰 예측력을 나타내었다. 한 가지 아쉬운 점은, 본 연구를 통해 독자적인 예측체계를 구 축해 보고 이 예측체계를 타 연구 기관의 것과 비교해 보려 하였으나, 다변량 분석에서 유의하게 나온 감시림프절 내 의 전이된 종양의 크기의 변수 하나만으로는 예측체계의 공식 성립이 어렵고, 표본수가 상대적으로 적어 큰 의미가 없었다는 점이다. 추후 표본수의 증대를 통해 이 한계점이 해결되리라 본다.
REFERENCES
1) Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002;347:1233-41.
2) Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 2002;347:1227-32.
3) Giuliano AE, Kirgan DM, Guenther JM, Morton DL.
Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 1994;220:391-8.
4) Yu JC, Hsu GC, Hsieh CB, Sheu LF, Chao TY. Prediction of metastasis to non-sentinel nodes by sentinel node status and primary tumor characteristics in primary breast cancer in Taiwan. World J Surg 2005;29:813-8.
5) Guenther JM, Hansen NM, DiFronzo LA, Giuliano AE, Collins JC, Grube BL, et al. Axillary dissection is not required for all patients with breast cancer and positive sentinel nodes.
Arch Surg 2003;138:52-6.
6) Sachdev U, Murphy K, Derzie A, Jaffer S, Bleiweiss IJ, Brower S. Predictors of nonsentinel lymph node metastasis in breast cancer patients. Am J Surg 2002;183:213-7.
7) Grube BJ, Giuliano AE. Observation of the breast cancer pa- tient with a tumor-positive sentinel node: implications of the ACOSOG Z0011 trial. Semin Surg Oncol 2001;20:230-7.
8) Ross MI. Sentinel node dissection in early-stage breast cancer:
ongoing prospective randomized trials in the USA. Ann Surg Oncol 2001;8:77S-81S.
9) Chagpar AB, Scoggins CR, Martin RC 2nd, Carlson DJ, Laidley AL, El-Eid SE, et al. Prediction of sentinel lymph node-only disease in women with invasive breast cancer. Am J Surg 2006;192:882-7.
10) Hwang RF, Krishnamurthy S, Hunt KK, Mirza N, Ames FC, Feig B, et al. Clinicopathologic factors predicting involvement of nonsentinel axillary nodes in women with breast cancer.
Ann Surg Oncol 2003;10:248-54.
11) Barranger E, Coutant C, Flahault A, Delpech Y, Darai E, Uzan S. An axilla scoring system to predict non-sentinel lymph node status in breast cancer patients with sentinel lymph node involvement. Breast Cancer Res Treat 2005;91:113-9.
12) Van Zee KJ, Manasseh DM, Bevilacqua JL, Boolbol SK, Fey JV, Tan LK, et al. A nomogram for predicting the likelihood of additional nodal metastases in breast cancer patients with a positive sentinel node biopsy. Ann Surg Oncol 2003;10:
1140-51.
13) Lyman GH, Giuliano AE, Somerfield MR, Benson AB 3rd, Bodurka DC, Burstein HJ, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol 2005;23:
7703-20.
14) Soni NK, Spillane AJ. Experience of sentinel node biopsy alone in early breast cancer without further axillary dissection in patients with negative sentinel node. ANZ J Surg 2005;75:
292-9.
15) Langer I, Marti WR, Guller U, Moch H, Harder F, Oertli D, et al. Axillary recurrence rate in breast cancer patients with negative sentinel lymph node (SLN) or SLN micrometastases:
prospective analysis of 150 patients after SLN biopsy. Ann Surg 2005;241:152-8.
16) Liang WC, Sickle-Santanello BJ, Nims TA. Is a completion axillary dissection indicated for micrometastases in the sentinel lymph node? Am J Surg 2001;182:365-8.
17) Barranger E, Morel O, Coutant C. Axilla scoring systems pre- dicting risk of non-sentinel-node metastasis in breast cancer patients with a positive sentinel node. Ann Surg Oncol 2008;
15:1261-2.
18) van Iterson V, Leidenius M, Krogerus L, von Smitten K.
Predictive factors for the status of non-sentinel nodes in breast cancer patients with tumor positive sentinel nodes. Breast Cancer Res Treat 2003;82:39-45.
19) Gipponi M, Canavese G, Lionetto R, Catturich A, Vecchio C, Sapino A, et al. The role of axillary lymph node dissection in breast cancer patients with sentinel lymph node micro- metastases. Eur J Surg Oncol 2006;32:143-7.
20) Chu KU, Turner RR, Hansen NM, Brennan MB, Bilchik A, Giuliano AE. Do all patients with sentinel node metastasis from breast carcinoma need complete axillary node dissection?
Ann Surg 1999;229:536-41.
21) Viale G, Maiorano E, Pruneri G, Mastropasqua MG, Valentini S, Galimberti V, et al. Predicting the risk for additional axil- lary metastases in patients with breast carcinoma and positive sentinel lymph node biopsy. Ann Surg 2005;241:319-25.
22) Stitzenberg KB, Meyer AA, Stern SL, Cance WG, Calvo BF, Klauber-DeMore N, et al. Extracapsular extension of the senti-
nel lymph node metastasis: a predictor of nonsentinel node tu- mor burden. Ann Surg 2003;237:607-12.
23) Schrenk P, Konstantiniuk P, Wolfl S, Bogner S, Haid A, Nemes C, et al. Prediction of non-sentinel lymph node status in breast cancer with a micrometastatic sentinel node. Br J
Surg 2005;92:707-13.
24) Callejo IP, Brito JA, Bivar JW, Fernandes FJ, Faria JL, Andre MS, et al. Predictors of positive axillary lymph nodes in breast cancer patients with metastatic sentinel lymph node. Clin Transl Oncol 2005;7:18-22.