Clinical Pediatric Hematology-Oncology Volume 23ㆍNumber 1ㆍApril 2016 CASE REPORT
53
철결핍빈혈로 내원한 고립성직장궤양증후군 청소년 환자 1예
정선희1ㆍ김영배1ㆍ김현진1ㆍ황진원2ㆍ이상헌2ㆍ정수진3ㆍ박지경1
인제대학교 의과대학 1소아과학교실, 2내과학교실, 3병리학교실
A Case of Solitary Rectal Ulcer Syndrome in a 16-year-old Girl Presented with Iron Deficiency Anemia
Sun Hee Jung, M.D.1, Young Bae Kim, M.D.1, Hyun Jin Kim, M.D.1, Jin Won Hwang, M.D.2, Sang Heon Lee, M.D.2, Su Jin Jung, M.D.3 and Ji Kyoung Park, M.D.1
Departments of 1Pediatrics, 2Internal Medicine, and 3Pathology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea
Solitary rectal ulcer syndrome (SRUS) is a rare condition that is most commonly charac- terized by rectal pain and bleeding. It can be accompanied by diarrhea or constipation, tenesmus, and rectal prolapse. Considering its non-specific symptoms, it is often difficult to diagnose, particularly in children. The underlying etiology of SRUS is not fully under- stood; however, it may be secondary to ischemic changes in the rectum associated with paradoxical contraction of the pelvic floor and external anal sphincter muscles and rectal prolapse. The macroscopic appearance of the rectal lesion may vary from hyperemia to ulceration or a polypoid lesion that can mimic carcinoma, although the histological findings are characteristic, with fibromuscular obliteration of the lamina propria and dis- orientation of muscle fibers. We report an adolescent case of SRUS developed in a 16-year-old adolescent girl who presented with iron deficiency anemia.
pISSN 2233-5250 / eISSN 2233-4580 http://dx.doi.org/10.15264/cpho.2016.23.1.53 Clin Pediatr Hematol Oncol 2016;23:53∼56
Received on April 1, 2016 Revised on April 12, 2016 Accepted on April 14, 2016
Corresponding Author: Ji Kyoung Park Department of Pediatrics, Busan Paik Hospital, Inje University College of Medicine, Kaekum-dong, Busanjin-gu, Busan 47392, Korea Tel: +82-51-890-6972
Fax: +82-51-895-7785 E-mail: [email protected]
Key Words: Solitary rectal ulcer syndrome, Anemia, Adolescent
Introduction
Solitary rectal ulcer syndrome (SRUS) is a rare, benign disorder in children, which usually presents with rectal bleeding, constipation, mucous discharge, prolonged strain- ing, tenesmus, lower abdominal pain, and localized pain in the perineal area [1,2].
After the first description by Cruveilhier, Madigan and Morson further detailed the clinical and pathologic features of SRUS in 1969 [2,3].
Its incidence is estimated to be one in 100,000 in adults;
however, only a few pediatric cases have been reported [4].
The clinical symptoms of SRUS are variable and patients may even be asymptomatic. Endoscopic findings vary and include mucosal ulcerations, polypoid and mass lesions, or erythema. Therefore, misdiagnosis is common on the basis of gross findings on colonoscopy [4,5]. Histologically, the presence of fibromuscular obliteration of the lamina propria with disorientation of muscle fibers is characteristic, which could be secondary to chronic mechanical and ischemic trauma and inflammation by hard stools, and intussu-
Sun Hee Jung, et al
54 Vol. 23, No. 1, April 2016
Fig. 1. Colonoscopic images of an SRUS patient, showing the distal rectum on retroflexion. Multiple polypoid lesions surrounded by erythema and inflammatory infil- tration.
sception of the rectal mucosa [3]. Therefore, the diagnosis of SRUS is usually based on the clinical symptoms com- bined with endoscopic and histologic findings [4]. We re- port an adolescent case of SRUS developed in a 16-year-old adolescent girl who presented with iron deficiency anemia.
Case Report
A 16-year-old girl was referred to our pediatric hematol- ogy-oncology clinic for syncope of one day and anemia which was revealed on laboratory examination in the local clinic. She has had episodes of constipation and recurrent rectal bleeding for the past two years. The frequency of rectal bleeding have increased over the last year. She had no history of fever, arthralgia, skin rashor abdominal pain.
She had no remarkable family history and was taking no medications. She had no previous history of hospitalization.
On physical examination, she was alert. Her weight and height were 61 kg (50-75th centile) and 168 cm (90-95th centile), respectively. She had anemic conjunctivae. Body temperature (axillary) was 36.4oC. Her pulse rate was 78 beats per minute and regular. Her blood pressure was 110/60 mmHg. She had normal heart sounds and no murmur. Her peripheral perfusion was normal. She had normal breath sounds bilaterally, and her respiratory rate was 20 breaths per minute. Her neurologic examination was normal. Studies including echocardiography, electro- cardiography, brain magnetic resonance imaging, electro- encephalogram,and gynecologic evaluations were normal.
The laboratory examinations revealed normal serum glu-
cose, electrolyte levels, C-reactive protein, thyroid function test, and cardiac enzymes. A peripheral blood smear re- vealed that erythrocytes were microcytic and hypochromic, indicating iron deficiency anemia (hemoglobin 7.9 g/dL, hematocrit 27.8%, mean corpuscular volume 63.0 fL, mean corpuscular hemoglobin 17.9 pg, mean cell hemoglobin concentration 28.4 g/dL, Fe 144dL, total iron binding ca- pacity 380 g/dL, ferritin 5.90 ng/mL, and transferrin satu- ration 3.7%). Colonoscopy revealed a large fungating semi-circumferential mass (approximately 3.5 cm in diame- ter) with ulcerated covering mucosa at the mid rectum and several medium-sized villous masses with ulcerated cover- ing mucosa at the distal rectum, just above the dentate line (Fig. 1). It was thought to be malignant until pathological findings to the contrary. Histopathologic examination of bi- opsy specimens revealed mucosal ulcerations with gran- ulation tissue proliferation and crypt dilatation, which con- firmed the diagnosis of SRUS (Fig. 2).
An increase in dietary fiber and regular use of laxatives were advised. Biofeedback therapy of retraining was recommended. Treatment for iron deficiency anemia was initiated with oral iron therapy. She is presently being fol- lowed with ongoing therapy for oral iron therapy and constipation.
Discussion
SRUS is a benign condition of the rectum and sigmoid that is often found in young adults [2,4,6]. SRUS is rarely reported in children because it is difficult to recognize both
Solitary Rectal Ulcer Syndrome
Clin Pediatr Hematol Oncol 55
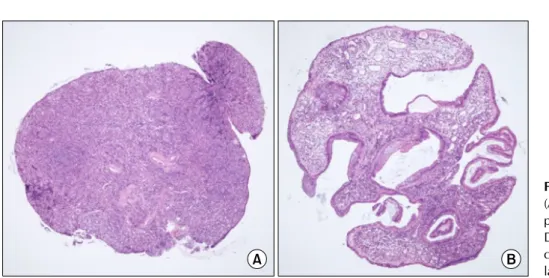
Fig. 2. Histopathological findings.
(A) Eroded and granulation tissue proliferation (H&E stain, 40×). (B) Dilated and haphazardly arranged crypts with ectatic capillaries in lamina propria (H&E stain, 40×).
the macroscopic and histopathological changes during childhood. Even in adults, the condition may go unrecog- nized or, more commonly, misdiagnosed for several years [5]. The average time from the onset of symptoms to diag- nosis is 3.2 years (range: 1.2-5 years) in children, which is shorter than that in adults (mean: 5 years; range: 3 months to 30 years) [1,2]. It should be recognized that a prolonged period of misdiagnosis may have important con- sequences, including anemia secondary to massive hemor- rhage or poor appetite in a growing child and distress to the child’s family [3].
SRUS occurs due to it being secondary to ischemia and trauma to the rectal mucosa and paradoxical contraction of the pelvic floor, due to which the pathophysiology of SRUS is not completely understood. The excessive straining gen- erates a high intrarectal pressure, which pushes the anterior rectal mucosa into the contracting puborectalis muscle, re- sulting in pressure necrosis of the rectal mucosa, and the anterior rectal mucosa is frequently forced into the closed anal canal, causing congestion, edema, and ulceration [1,2].
SRUS is usually a benign condition; however, significant morbidity can occur if complicated by underlying disease states [7]. The clinical features are as follows: rectal bleed- ing, copious mucus discharge, prolonged excessive strain- ing, perineal and abdominal pain, feeling of incomplete defecation, constipation, and rarely, rectal prolapse. Some children present with apparent diarrhea (because of pro- longed visits to the bathroom), and associated bleeding, ab- dominal pain, and tenesmus, suggesting the presence of in-
flammatory bowel disease to clinicians [6]. Anemia is incon- sistently present in SRUS. A prolonged period of mis- diagnosis may cause anemia secondary to massive bleed- ing; however, blood transfusion in SRUS is rare [7]. Iron deficiency anemia was observed in the present case and was treated with oral iron supplements; however, blood transfusion was not required.
The clinical presentation varies; therefore, early diagnosis requires a high index of suspicion of both the clinician and pathologist [3,6]. The diagnosis of SRUS is usually based on the clinical symptoms combined with the endoscopic and histologic findings [4]. A complete and thorough history is most important in the initial diagnosis of SRUS. The most common clinicopathologic diagnostic confusion may be in- flammatory bowel disease (IBD), infectious proctocolitis, intussusception, hemorrhoids, prolapsing rectal polyp, or sexual abuse in children, whereas villous adenoma or ad- enocarcinoma should also be included in the differential di- agnosis of SRUS in adulthood [3,6]. IBD should be consid- ered in case of prolonged diarrhea, abdominal pain and growth delay. The histological features of SURS should be differentiated from to other diseases of rectum including IBD and infective or nonspecific colitis, which may show chronic and acute inflammatory cells in lamina propria, cryptitis, crypt abscess and granuloma formation, with dis- tortion of epithelial and glandular structures [8]. SRUS is a misnomer, because the lesion may be solitary or multiple and different in shape and size (ulcerative, polypoidal/
nodular, or erythematous mucosa only). Macroscopically,
Sun Hee Jung, et al
56 Vol. 23, No. 1, April 2016
SRUS typically appears as shallow ulcerating lesions on a hyperemic sur-rounding mucosa, most often located on the anterior wall of the rectum at 5-10 cm from the anal verge(diameter range: 0.5-4 cm), but usually 1-1.5 cm in diameter [1]. The SRUS-polypoid variant may lead to a seri- ous misdiagnosis, because its appearance may be confused with an inflammatory polyp, hyperplastic polyps, or rectal carcinoma [5,9,10]. Our patient had multiple polypoid le- sions that were circumferential with an ulcerated surface that mimicked rectal cancer in its appearance. Misdiagnosis of SRUS as malignancy can lead to unnecessary surgery or treatment [11]. Histopathological examination is key to the diagnosis of SRUS. A combination of fibromuscular ob- literation of the lamina propria, crypt distortion, and surface serration can establish the diagnosis in most cases [5].
Therapeutic experience in children with SRUS is limited, with variable treatment protocols and clinical outcomes.
Patient education and behavioral modification are the first steps in the treatment of SRUS. The treatment includes re- assurance of the patient that the lesion is benign, encour- agement of a high-fiber diet, avoidance of straining, and regulation of toilet habits [6]. The present treatment in- cludes bulking agents (lactulose), enemas (steroid and me- salamine), oral 5-ASA, sucralfate, bowel retraining with or without biofeedback, endoscopical steroid injection, and surgery (rectopexy, excision of ulcer) in refractory cases not responding to conservative treatments [1,11]. Repeat endos- copies were not routinely conducted unless patients had persistent symptoms, particularly bleeding [1].
There are no specific clinical features of this disease;
therefore, SRUS can be easily mistaken for other common diseases observed in children and result in inappropriate management of these patients [4,5,9].
In summary, physicians must have a high index of suspi-
cion for SRUS in patients who present with the presence of a rectal polypoid masswith ulceration, rectal bleeding, and anemia [4,5]. We report an adolescent case of SRUS developed in a 16-year-old adolescent girl who presented with iron deficiency anemia.
References
1. Urgancı N, Kalyoncu D, Eken KG. Solitary rectal ulcer syn- drome in children: a report of six cases. Gut Liver 2013;7:
752-5.
2. Hahn WH, Kim ES, Kim HJ, Cha SH. A case of solitary rectal ulcer syndrome. Korean J Pediatr 2004;47:896-9.
3. Ertem D, Acar Y, Karaa EK, Pehlivanoglu E. A rare and often unrecognized cause of hematochezia and tenesmus in child- hood: solitary rectal ulcer syndrome. Pediatrics 2002;110:e79.
4. Dehghani SM, Haghighat M, Imanieh MH, Geramizadeh B.
Solitary rectal ulcer syndrome in children: a prospective study of cases from southern Iran. Eur J Gastroenterol Hepatol 2008;20:93-5.
5. Saadah OI, Al-Hubayshi MS, Ghanem AT. Solitary rectal ulcer syndrome presenting as polypoid mass lesions in a young girl.
World J Gastrointest Oncol 2010;2:332-4.
6. Zhu QC, Shen RR, Qin HL, Wang Y. Solitary rectal ulcer syn- drome: clinical features, pathophysiology, diagnosis and treat- ment strategies. World J Gastroenterol 2014;20:738-44.
7. Urganc N, Kalyoncu D, Usta M, Eken KG. A rare cause of severe rectal bleeding: solitary rectal ulcer syndrome. Pediatr Emerg Care 2014;30:736-8.
8. Keshtgar AS. Solitary rectal ulcer syndrome in children. Eur J Gastroenterol Hepatol 2008;20:89-92.
9. Park HB, Park HC, Chung CY, et al. Coexistence of solitary rectal ulcer syndrome and ulcerative colitis: a case report and literature review. Intest Res 2014;12:70-3.
10. Choi YM, Song HJ, Kim MJ, Chang WY, Kim BS, Hyun CL.
Solitary rectal ulcer syndrome mimicking rectal cancer. Ewha Med J 2016;39:28-31.
11. Park HB, Park HC, Chung CY, et al. Coexistence of solitary rectal ulcer syndrome and ulcerative colitis: a case report and literature review. Intest Res 2014;12:70-3.