http://dx.doi.org/10.15656/kjcg.2014.15.2.45
Received: September 19, 2014 Revised: December 16, 2014 Accepted: December 16, 2014.
Corresponding author: Dong-Kuck Lee
Department of Neurology, Catholic University of Daegu, School of Medicine, 33 Duryugongwon-ro 17-gil, Nam-gu, Daegu 705-718, Korea Tel: +82-53-650-4267, Fax: +82-53-654-9786, E-mail: dklee@cu.ac.kr
Copyright Ⓒ 2014 The Korean Academy of Clinical Geriatrics
This is an open access article distributed under the term s of the Creative Com m ons Attribution Non-Com m ercial License (http://creativecom m ons.org/ licenses/by-nc/3.0) which perm its unrestricted non-com m ercial use, distribution, and reproduction in any m edium , provided the original work is properly cited.
노인 어지럼증에 대한 임상적 이해
이동국
대구가톨릭대학교 의과대학 신경과학교실
Clinical Understanding to Dizziness in the Elderly
Dong-Kuck Lee
Department of Neurology, Catholic University of Daegu, School of Medicine, Daegu, Korea
Dizziness is a broad term used to describe a variety of sensations such as vertigo, unsteadiness, lightheadedness, and similar symptoms. Dizziness is a common and potentially serious complaint among the elderly. Left untreated, it can lead to falls and serious injuries. The prevalence of dizziness increases steadily with age. Although debate is still ongoing about the underlying causes of this increase in prevalence, there is universal agreement on its devastating consequences and high physical, emotional, and financial toll on the older population. It is estimated that one-fourth to one-third of the population older than 65 years has experienced some form dizziness. The history is often critical to determining the most likely causes of dizziness. Especially medications as a risk factor for dizziness in the older adult population. Older individuals who suffer from dizziness appear to be at significantly higher risk of accidental falls and consequent injuries. Therefore the strong association between falls and symptoms of dizziness and imbalance highlights the importance of understanding the causes of these symptoms and designing effective methods for managing them in the older population. When possible, a multidisciplinary approach with an integrated strategy is more effective in the diagnosis and management of dizziness because the understanding the underlying causes often span multiple systems.
Key Words: Dizziness, Older
서 론
어지럼증(dizziness)은 노인에서 흔히 볼 수 있는 증상 이다. 그러나 대부분 노인들이 어지럼증에 대해서는 모 호하거나 애매하게 표현하는 경우가 많다. 특히 나이가 들수록 더 어지러워지는 것은 연령에 따른 생리적 변화 와 더불어 전정계, 고유감각(proprioception)계, 시각계, 운 동계, 및 중추 통합(integration)계 등과 균형계의 퇴행 등
이 그 원인으로 생각된다. 80세 이상 되는 사람들 중 15∼
40% 이상에서 어지럼증을 호소한다. 젊은 사람들에 비 해 노인 어지럼증은 일상 생활에 심각한 장애를 일으키 고 더 만성적으로 생기며 훨씬 더 다양한 원인에 의해 발생한다. 어지럼증의 진단에 가장 중요한 것은 상세한 병력청취이다. 감별진단을 위해선 전정계의 해부 및 생 리에 대한 이해와 각 질환의 특징적인 증상 및 징후을 알고 어지럼증 환자를 진찰할 수 있어야 한다. 특히 노
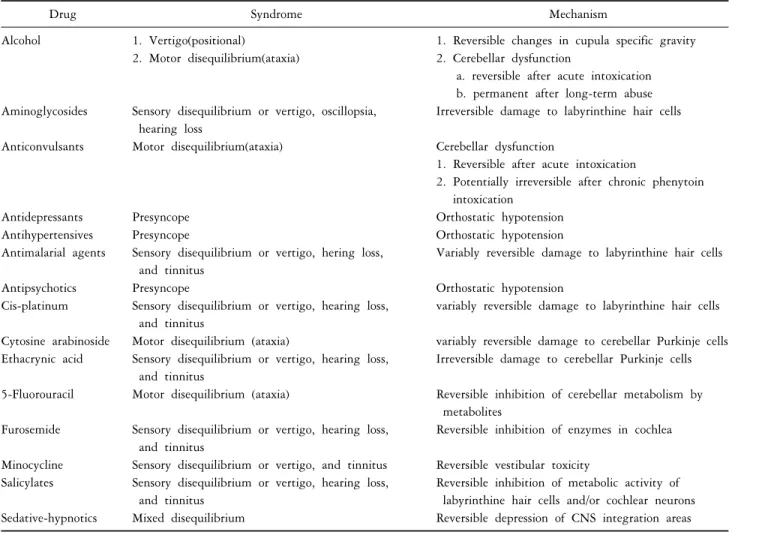
Table 1. Drug associated with dizziness
Drug Syndrome Mechanism
Alcohol 1. Vertigo(positional) 1. Reversible changes in cupula specific gravity 2. Motor disequilibrium(ataxia) 2. Cerebellar dysfunction
a. reversible after acute intoxication b. permanent after long-term abuse Aminoglycosides Sensory disequilibrium or vertigo, oscillopsia,
hearing loss
Irreversible damage to labyrinthine hair cells
Anticonvulsants Motor disequilibrium(ataxia) Cerebellar dysfunction
1. Reversible after acute intoxication
2. Potentially irreversible after chronic phenytoin intoxication
Antidepressants Presyncope Orthostatic hypotension
Antihypertensives Presyncope Orthostatic hypotension
Antimalarial agents Sensory disequilibrium or vertigo, hering loss, and tinnitus
Variably reversible damage to labyrinthine hair cells
Antipsychotics Presyncope Orthostatic hypotension
Cis-platinum Sensory disequilibrium or vertigo, hearing loss, and tinnitus
variably reversible damage to labyrinthine hair cells
Cytosine arabinoside Motor disequilibrium (ataxia) variably reversible damage to cerebellar Purkinje cells Ethacrynic acid Sensory disequilibrium or vertigo, hearing loss,
and tinnitus
Irreversible damage to cerebellar Purkinje cells
5-Fluorouracil Motor disequilibrium (ataxia) Reversible inhibition of cerebellar metabolism by metabolites
Furosemide Sensory disequilibrium or vertigo, hearing loss, and tinnitus
Reversible inhibition of enzymes in cochlea
Minocycline Sensory disequilibrium or vertigo, and tinnitus Reversible vestibular toxicity Salicylates Sensory disequilibrium or vertigo, hearing loss,
and tinnitus
Reversible inhibition of metabolic activity of labyrinthine hair cells and/or cochlear neurons Sedative-hypnotics Mixed disequilibrium Reversible depression of CNS integration areas
인 어지럼증은 단순한 진단명이라기 보다는 포괄적인증후군(syndrome)으로 생각하고 다각적으로 접근하는 것 이 중요하다.
본 론
1-14)
1. 병력
어지럼증이란 공간에서 지남력 변화 또는 불균형(dise- qilibrium)으로 인한 불쾌한 감각을 표현하는 비특이적 용어이다. 병적인 어지럼증은 크게 현기, 불균형, 전실신 (presyncope), 및 정신생리적 어지럼증 등으로 구분한다.
병력, 어지럼증 유발검사, 및 진찰 등을 통해 대부분의 어지럼증은 감별진단이 가능하다.
현기는 긴장형 전정 활동의 불균형으로 인한 운동 착 각이다. 현기는 대부분 회전성으로 나타나며 세반고리관 이나 중추 연결에 이상이 있다는 것을 나타내는 것이다.
몸이 한쪽으로 쏠리는 감이나 넘어지려는 것은 이석
(otolith)의 이상을 나타낸다. 현기는 안구진탕(nystagmus), 자세 불균형, 메스꺼움, 구토, 또는 진동시(oscillopsia) 등 을 동반한다. 중추성보단 말초성 현기에서 땀, 창백, 메 스꺼움, 및 구토 등의 자율신경 이상증상이 잘 나타난다.
노인성 현기의 흔한 원인으로는 양성 발작성 체위성 현 기, 바이러스성 신경미로염, 외상, 독소, 및 후뇌 또는 미 로 허혈 등이 있다. 젊은 성인 현기의 흔한 원인으로는 메니에르병, 바이러스성 신경미로염, 외상, 및 독소 등이 있다.
불균형이란 비현기성 정적(static) 또는 동적인(dynamic) 자세 균형에 문제가 생긴 상태를 말한다. 불균형 상태의 환자들은 자주 불안정하고 균형이 맞지 않아 넘어지려 한다. 불균형 상태는 크게 감각성과 운동성으로 나눈다.
감각성 불균형은 고유감각 장애, 전정 기능 장애, 시력- 전정 부조합, 및 다발성 감각장애 등으로 인한 공간 지 각력의 이상 때문에 발생한다. 감각성 불균형은 어두운 장소에서 더 악화되며 Romberg 징후가 자주 양성으로
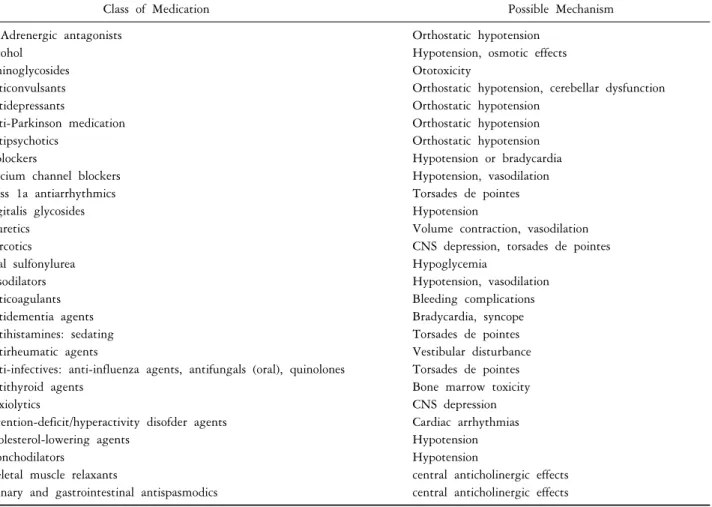
Table 2. Medications that often cause dizziness in older adults
Class of Medication Possible Mechanism
1-Adrenergic antagonists Alcohol
Aminoglycosides Anticonvulsants Antidepressants
Anti-Parkinson medication Antipsychotics
-blockers
Calcium channel blockers Class 1a antiarrhythmics Digitalis glycosides Diuretics
Narcotics Oral sulfonylurea Vasodilators Anticoagulants Antidementia agents Antihistamines: sedating Antirheumatic agents
Anti-infectives: anti-influenza agents, antifungals (oral), quinolones Antithyroid agents
Anxiolytics
Attention-deficit/hyperactivity disofder agents Cholesterol-lowering agents
Bronchodilators
Skeletal muscle relaxants
Urinary and gastrointestinal antispasmodics
Orthostatic hypotension Hypotension, osmotic effects Ototoxicity
Orthostatic hypotension, cerebellar dysfunction Orthostatic hypotension
Orthostatic hypotension Orthostatic hypotension Hypotension or bradycardia Hypotension, vasodilation Torsades de pointes Hypotension
Volume contraction, vasodilation CNS depression, torsades de pointes Hypoglycemia
Hypotension, vasodilation Bleeding complications Bradycardia, syncope Torsades de pointes Vestibular disturbance Torsades de pointes Bone marrow toxicity CNS depression Cardiac arrhythmias Hypotension Hypotension
central anticholinergic effects central anticholinergic effects
나타난다. 운동성 불균형은 중추 및 말초신경계중 운동신경로의 이상이나 기계적 인자들의 장애로 인해 나타 난다. 중추성 원인으로는 추체로, 추체외로, 및 소뇌 등 에 문제가 생긴 경우이고 말초성은 말초신경, 신경근육 접합부, 및 근육의 이상으로 인해 운동성 불균형이 생긴 다. 운동성 불균형은 어두운 곳에 가거나 눈을 감아도 더 악화되지는 않는다.
전실신은 곧 의식을 잃을 것 같은 감각으로 힘이 빠 지고 메스꺼우며 땀이 나고 속이 불편하다. 그 외에도 얼굴이 창백해 지고 눈이 침침해 지며 암점(scotoma)도 생기고 두통, 가슴이 두근거림, 이상감각 및 손발이 수 축되는 것 같는 증상도 보인다. 전실신은 뇌대사가 갑자 기 전반적으로 장애가 와서 생긴다. 그런 원인으로는 뇌 허혈, 저혈당, 및 저산소증 등이 있다. 그 외에도 심박출 량의 감소, 말초 혈관수축기능의 저하, 뇌혈관 수축, 정 맥순환 부전, 및 혈량저하증(hypovolemia) 등이 있다. 과 호흡이나 저혈당 상태에서도 진정한 실신은 드물다. 전 실신은 누우면 회복된다.
정신생리적 어지럼증은 막연하고 모호한 어지럼증으 로 급성 또는 만성 불안이 있는 사람들이 잘 호소한다.
이런 어지럼증은 기분에 따라 증상이 변한다. 특히 복잡 하고 답답한 환경, 갇힌 공간, 또는 심한 스트레스 받는 상황에서 잘 발병한다. 이런 어지럼증에서는 얼굴이 창 백해 지는 일은 없고 누워도 호전되지 않는다.
모든 어지럼증 환자를 진찰할 때는 항상 약물과의 연 관성을 생각해 보아야 한다. 어지럼증을 잘 일으키는 약 물로는 Table 1, 2 등이 있다. 특히 노인들은 귀독성 (ototoxicity) 약물을 자주 먹고 신체 예비력(reserve)은 떨 어져 있으며 신장 기능도 약하므로 약물에 의한 이독성 이 잘 생긴다.
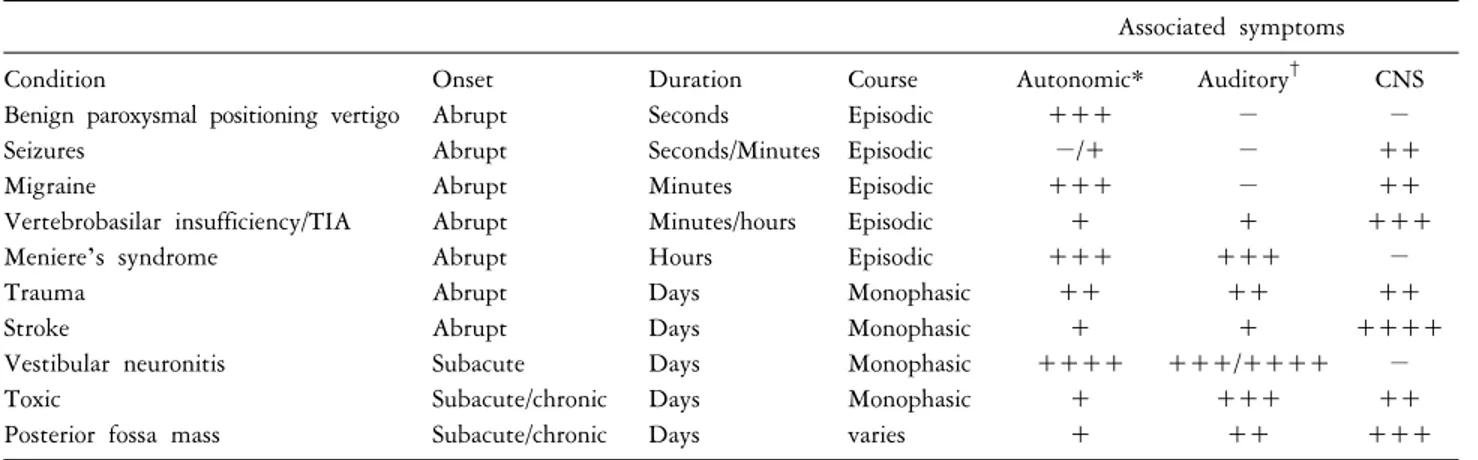
어지럼증의 감별진단에 필요한 병력은 Table 3, 4와 같다. 특히 현기의 발병(onset), 기간, 경과 및 자율신경, 청신경, 및 중추신경계 동반 증상을 잘 살펴 보는 것이 감별진단에 중요하다. 현기를 해부학적 위치에 따라 감 별진단 하는데 도움이 되는 신경 증상은 Table 5와 같다.
어지럼증은 머리 운동, 기침 재채기, 또는 큰 소리 등에
Table 3. Key features in history
Vertigo Acute onset or more gradual Preceding or precipitating factors Hearing loss
Auditory symptoms Tinnitus
Ear discharge or pain
Sense of fullness or blockage in the ear Headache Before, during or after the vertigo Associated neurology Diplopia
Other visual disturbance Dysarthria or dysphagia Paraesthesia or muscle weakness
Medication Aminoglycosides
Anticonvulsant Risk factors for
cerebrovascular accident or transient ischaemic attack
Previous angina or myocardial infarction Diabetes mellitus
Hypertension Smoking Atrial fibrillation Past history Head injury
Chronic ear infections Migraine
Table 4. History in the differential diagnosis of vertigo
Associated symptoms
Condition Onset Duration Course Autonomic* Auditory
†CNS
Benign paroxysmal positioning vertigo Abrupt Seconds Episodic +++ − −
Seizures Abrupt Seconds/Minutes Episodic −/+ − ++
Migraine Abrupt Minutes Episodic +++ − ++
Vertebrobasilar insufficiency/TIA Abrupt Minutes/hours Episodic + + +++
Meniere’s syndrome Abrupt Hours Episodic +++ +++ −
Trauma Abrupt Days Monophasic ++ ++ ++
Stroke Abrupt Days Monophasic + + ++++
Vestibular neuronitis Subacute Days Monophasic ++++ +++/++++ −
Toxic Subacute/chronic Days Monophasic + +++ ++
Posterior fossa mass Subacute/chronic Days varies + ++ +++
−: never, +: uncommon, ++: common, +++: typical, ++++: universal. TIA: transient ischemic attack. *Autonomic symptoms (sweating, pallor, nausea, vomiting) are much more common and much more severe with vertigo of peripheral origin (labyrinth or eighth nerve) than with vertigo of CNS origin.
†Auditory symptoms generally only occur if the vascular event involves either the inner ear or the acoustic nerve.
Table 5. Neurologic symptoms associated with vertigo due to lesions at different anatomic sites
Inner ear ㆍHearing loss ㆍTinnitus
Internal auditory canal ㆍFacial weakness ㆍHearing loss ㆍTinnitus
Cerebellopontine angle ㆍFacial numbness ㆍFacial weakness ㆍHearing loss ㆍTinnitus
ㆍExtremity incoordination Brainstem
ㆍDiplopia ㆍFacial numbness ㆍFacial weakness ㆍDysarthria ㆍDysphagia
ㆍExtremity weakness ㆍExtremity incoordination ㆍExtremity numbness Cerebellum
ㆍExtremity incoordination
의해 악화된다.2. 원인
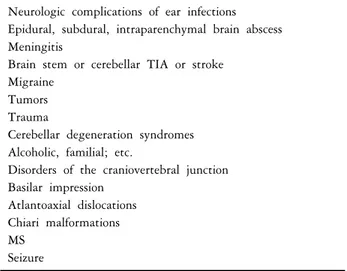
어지럼증은 다양한 원인에 의해 발생한다. 말초 현기 의 원인과 중추 현기의 원인들은 Table 6∼9와 같다.
3. 진찰
어지럼증을 호소하는 환자를 진찰하는 것은 쉬운 일
이 아니다. 특히 노인에서 여러 가지 신체 가능이 떨어 진 상태이거나 뇌졸중 또는 치매가 있는 경우에는 더욱 진찰이 힘들다. 만약 가끔씩 어지럼증이 있는 경우라면 유발시켜 보는 것도 좋다. 머리를 빠르게 회전시키거나 caloric 검사를 하면 현기가 유발된다. 과호흡을 하면 전
Table 6. Common causes of dizziness
Type Cause
Vertigo Benign paroxysmal positional vertigo, Meniere disease, labyrinthitis, vestibular neuronitis, inner ear auto- immune diesease, perilymphatic fistula, migraine*, labyrinthine concussion*, transverse temporal bone fracture, vertebrobasilar ischemia, lateral medullary infarct (Wallenberg syndrome), cervical injury Disequilibrium Peripheral neuropathy, acoustic neuroma*, ototoxic drugs, cerebellar atrophy, cerebellar infarction, tumors
of the posterior fossa, aging, multiple sclerosis*, Wernicke encephalopathy
Dizziness, light headedness Cardiac arrhythmia, vasovagal reaction, postural hypotension, systemic viral or bacterial infection, hypo- glycemia, hyperglycemia, electrolyte disturbances, thyrotoxicosis, anemia, psychophysiologic
†, adverse drug reaction, ocular dizziness due to rapid vision change (after cataract surgery, a change in a corrective prescription)
*May also present with dizziness,
†May also present with vertigo.
Table 8. Common causes of central vertigo Neurologic complications of ear infections Epidural, subdural, intraparenchymal brain abscess Meningitis
Brain stem or cerebellar TIA or stroke Migraine
Tumors Trauma
Cerebellar degeneration syndromes Alcoholic, familial; etc.
Disorders of the craniovertebral junction Basilar impression
Atlantoaxial dislocations Chiari malformations MS
Seizure Table 7. Common causes of peripheral vertigo
Benign paroxysmal positional vertigo Bacterial or viral infections
Vestibular neuritis Meniere disease
Labyrinthine ischemia or hemorrhage Tumor
Trauma
Temporal bone fracture Labyrinthine concussion
Perilymphatic fistula (fistula may also be caused by cholesteatoma) Metabolic disorders
Diabetes mellitus Uremia
Hypothyroidism Paget disease
Acute alcohol intoxication Ototoxicity
Aminoglycosides Cisplatin
Autoimmune inner ear disease
Superior semicircular canal dehiscence syndrome
실신이 유발되며 이때 입 주위나 발목에 이상감각과 연 축(spasm)이 동반될 수도 있다. 기립 저혈압을 알기 위해 선 누운 상태와 선 상태에서 맥박과 혈압을 측정한다.
선 상태에서 3분 지나 수축기 혈압이 20 mmHg 또는 이 완기 혈압이 10 mmHg 이상 떨어지면 기립 저혈압이라 고 한다. 그러나 기립 저혈압 증상을 보여도 일부에서는 서서 10분 이상 지나도 혈압이 떨어지지 않는 경우도 있 다. 어지럼증을 호소하는 모든 환자에서는 눈, 귀, 심혈 관계, 신경계, 및 전정계 기능을 잘 살펴야 한다. 특히 안구진탕은 중추성과 말초성 어지럼증을 감별하는데 중 요하므로 모양, 악화 및 억제 인자들을 잘 봐야 한다. 병
적 안구진탕은 자발성으로도 나타나고 안구와 머리 위 치를 변동해도 나타난다. 말초 전정 안구진탕을 억제하 는 가장 중요한 방법은 고정(fixation)이다. 중추 및 말초 안구진탕의 특징적인 소견은 Table 10∼12와 같다.
Dix-Hallpike 검사는 양성 돌발성 체위 현기같이 체위에 따라 유발되는 안구진탕의 진단에 유용하다. 특히 caloric 검사는 말초 전정 병변을 진단하는 데 중요하다. 또한 눈을 감은 상태와 눈을 뜬 상태에서 직렬(tandem)보행을 하는 것도 중추성과 말초성 어지럼증을 진단하는데 도 움이 된다(Table 13∼15).
4. 검사
어지럼증은 병력과 진찰을 통해 대부분 진단된다. 그 러나 중추성과 말초성 어지럼증을 감별하기 위해선 적 절한 검사를 선택적으로 이용해야 한다. 진단에 도움이 되는 검사들로는 청력검사, 뇌간청각 유발전위, 뇌영상
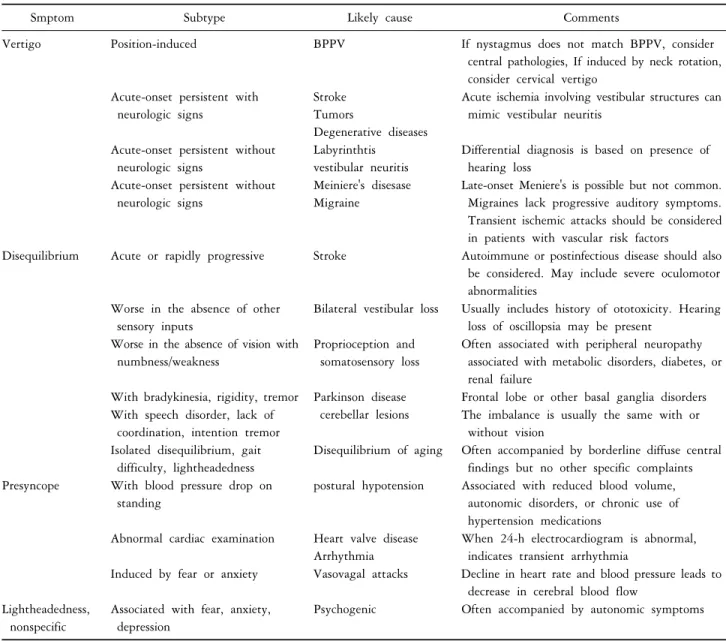
Table 9. Common causes of dizziness in the elderly for different types of symptoms
Smptom Subtype Likely cause Comments
Vertigo Position-induced BPPV If nystagmus does not match BPPV, consider
central pathologies, If induced by neck rotation, consider cervical vertigo
Acute-onset persistent with neurologic signs
Stroke Tumors
Degenerative diseases
Acute ischemia involving vestibular structures can mimic vestibular neuritis
Acute-onset persistent without neurologic signs
Labyrinthtis vestibular neuritis
Differential diagnosis is based on presence of hearing loss
Acute-onset persistent without neurologic signs
Meiniere's disesase Migraine
Late-onset Meniere's is possible but not common.
Migraines lack progressive auditory symptoms.
Transient ischemic attacks should be considered in patients with vascular risk factors
Disequilibrium Acute or rapidly progressive Stroke Autoimmune or postinfectious disease should also be considered. May include severe oculomotor abnormalities
Worse in the absence of other sensory inputs
Bilateral vestibular loss Usually includes history of ototoxicity. Hearing loss of oscillopsia may be present
Worse in the absence of vision with numbness/weakness
Proprioception and somatosensory loss
Often associated with peripheral neuropathy associated with metabolic disorders, diabetes, or renal failure
With bradykinesia, rigidity, tremor Parkinson disease cerebellar lesions
Frontal lobe or other basal ganglia disorders With speech disorder, lack of
coordination, intention tremor
The imbalance is usually the same with or without vision
Isolated disequilibrium, gait difficulty, lightheadedness
Disequilibrium of aging Often accompanied by borderline diffuse central findings but no other specific complaints Presyncope With blood pressure drop on
standing
postural hypotension Associated with reduced blood volume, autonomic disorders, or chronic use of hypertension medications
Abnormal cardiac examination Heart valve disease Arrhythmia
When 24-h electrocardiogram is abnormal, indicates transient arrhythmia
Induced by fear or anxiety Vasovagal attacks Decline in heart rate and blood pressure leads to decrease in cerebral blood flow
Lightheadedness, nonspecific
Associated with fear, anxiety, depression
Psychogenic Often accompanied by autonomic symptoms
Table 10. Clinical features of peripheral and central spontaneous vestibular nystagmus
Peripheral Central
Appearance ㆍJerk
ㆍMixed linear and rotatory
ㆍUnidirectional (beats away from hypofunctioning labyrinth)
ㆍJerk or pendular
ㆍMay be pure linear or pure rotatory
ㆍMay change direction with gaze in different directions
Fixation ㆍInhibits nystagmus ㆍLittle effect
Associated symptoms and signs
ㆍSevere vertigo ㆍSevere nausea
ㆍHearing loss and tinnitus common
ㆍNo central nervous system symptoms or signs
ㆍMild or absent vertigo ㆍMild or absent nausea
ㆍHearing loss and tinnitus uncommon
ㆍCentral nervous system symptoms and signs common
검사, 안진계(nystagmography), 및 caloric 검사 등이 있다.
만약 진단이 힘들면 신경과와 이비인후과 의사들의 자 문도 필요하다.
5. 감별진단
어지럼증이 중추성인지 말초성인지를 감별하는 것은 중요하다. 현기와 기타 다른 형태의 어지럼증을 감별하
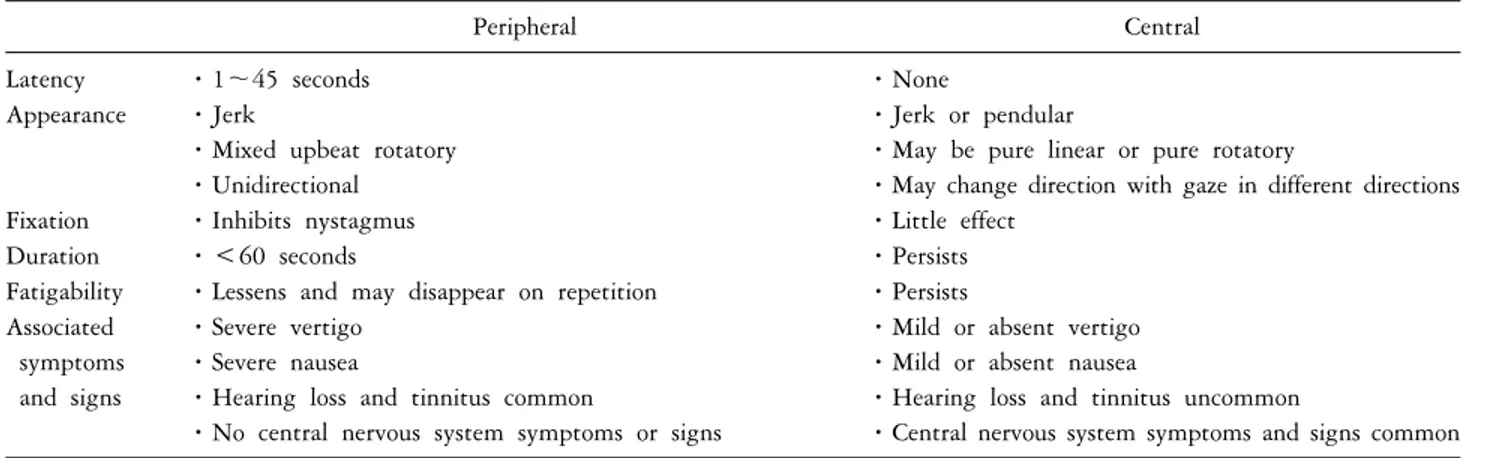
Table 11. Clinical features of peripheral and central positional vestibular nystagmus
Peripheral Central
Latency ㆍ1∼45 seconds ㆍNone
Appearance ㆍJerk
ㆍMixed upbeat rotatory ㆍUnidirectional
ㆍJerk or pendular
ㆍMay be pure linear or pure rotatory
ㆍMay change direction with gaze in different directions
Fixation ㆍInhibits nystagmus ㆍLittle effect
Duration ㆍ<60 seconds ㆍPersists
Fatigability ㆍLessens and may disappear on repetition ㆍPersists Associated
symptoms and signs
ㆍSevere vertigo ㆍSevere nausea
ㆍHearing loss and tinnitus common
ㆍNo central nervous system symptoms or signs
ㆍMild or absent vertigo ㆍMild or absent nausea
ㆍHearing loss and tinnitus uncommon
ㆍCentral nervous system symptoms and signs common
Table 12. Features of peripheral and central vertigo
Sign or symptom Peripheral (Labyrinth or vestibular nerve) Central (Brainstem or Cerebellum) Direction of associated nystagmus Unidirectional, fast phase opposite lesiona* Bidirectional (direction-changing)
or unidirectional Purely horizontal nystagmus without
torsional component
Uncommon May be present
Purely vertical or purely torsional nystagmus Never present
†No inhibition
Visual fixation Inhibits nystagmus usually absent
Tinnitus and/or deafness Often present usually absent
Associated central nervous system abnormalities
None Extremely common (diplopia, hiccups,
cranial neuropathies, dysarthria) Common causes Benign paroxysmal positional vertigo,
infection (labyrinthitis), vestibular neuritis, Meniere's disease, labyrinthine ischemia, trauma, toxin
Vascular, demyelinating, neoplasm
*In Meniere's disease, the direction of the fast phase is variable,
†Combined vertical-torsional nystagmus suggests BPPV.
Table 13. Key features on examination Eye movements Range of movement
Diplopia
Gaze evoked or spontaneous nystagmus Nystagmus Ratatory, horizontal, vertical or mixed
Direction of gaze in which most pronounced
Does it change direction on changing direction of gaze Ears Tympanic membrane for any perforation
Hearing Whispered voice at arm's length with other ear occluded
Weber's and Rinne's test to determine whether sensorineural or conductive deafness Other neurology Cranial and peripheral nerves
Gait and balance Romberg's test
Ability to stand and walk unaided
기 위해서는 어지럼증이 돌발적, 아급성, 또는 만성인지 알아보고 발병이 주기적인지 또는 일회성인지 알아 보 아야 한다. 또는 어지럼증의 지속시간도 알아 본다. 또 한 어지럼증이 현기, 불균형, 전실신, 또는 정신과 어지
럼증인지 감별한다. 동반증상으로 메스꺼움이나 구토 같 은 자율신경이상, 청력소실이나 이명 같은 청신경 증상, 또는 복시, 얼굴 감각이상, 또는 사지 마비 같은 중추신 경계 증상이 있는지 확인한다. 또한 Dix-Hallpike 검사,
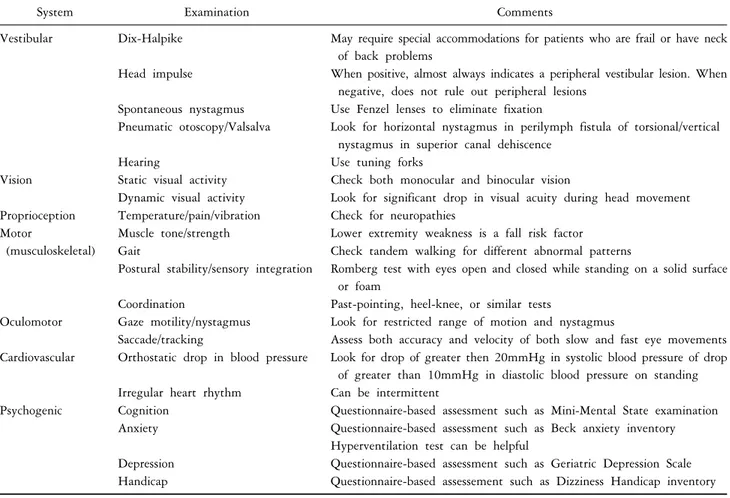
Table 14. Common components of physical examination
System Examination Comments
Vestibular Dix-Halpike May require special accommodations for patients who are frail or have neck of back problems
Head impulse When positive, almost always indicates a peripheral vestibular lesion. When negative, does not rule out peripheral lesions
Spontaneous nystagmus Use Fenzel lenses to eliminate fixation
Pneumatic otoscopy/Valsalva Look for horizontal nystagmus in perilymph fistula of torsional/vertical nystagmus in superior canal dehiscence
Hearing Use tuning forks
Vision Static visual activity Check both monocular and binocular vision
Dynamic visual activity Look for significant drop in visual acuity during head movement Proprioception Temperature/pain/vibration Check for neuropathies
Motor
(musculoskeletal)
Muscle tone/strength Lower extremity weakness is a fall risk factor Gait Check tandem walking for different abnormal patterns
Postural stability/sensory integration Romberg test with eyes open and closed while standing on a solid surface or foam
Coordination Past-pointing, heel-knee, or similar tests
Oculomotor Gaze motility/nystagmus Look for restricted range of motion and nystagmus
Saccade/tracking Assess both accuracy and velocity of both slow and fast eye movements Cardiovascular Orthostatic drop in blood pressure Look for drop of greater then 20mmHg in systolic blood pressure of drop
of greater than 10mmHg in diastolic blood pressure on standing Irregular heart rhythm Can be intermittent
Psychogenic Cognition Questionnaire-based assessment such as Mini-Mental State examination Anxiety Questionnaire-based assessment such as Beck anxiety inventory
Hyperventilation test can be helpful
Depression Questionnaire-based assessment such as Geriatric Depression Scale Handicap Questionnaire-based assessement such as Dizziness Handicap inventory
과호흡, 또는 머리 회전(rotation)같은 유발방법으로 어지 러운 증상이 나오는지 본다. 특히 두위변환검사 중 Dix-Hallpike 검사는 말초성 두위 현훈의 진단을 위해 가 장 흔히 이용되는 방법이다. 이 검사법은 우선 눕혔을 때 환자의 어깨가 침대 끝에 닿을 수 있을 정도의 적당 한 위치에 환자를 앉힌 후 검사자는 환자의 머리를 양손 으로 잡은 다음 머리를 45도 돌린 상태에서 빠르게 뒤로 눕혀 침대 끝에서 환자의 머리가 45도 각도로 지면을 향 하도록 한다(Figure 1). 이 검사를 하기 전에는 우선 환자 를 안심시킨 상태에서 온몸의 긴장을 풀도록 해야 한다.
또한 검사에 의해 현훈이 유발 되면 환자는 자동적으로 눈을 감는 경향이 있으므로 환자에게 검사 도중 눈을 뜨 고 있도록 이야기 해 주어야 한다. 두위 변환 후 적어도 20초 이상 두위를 유지하여 안진의 잠복기와 지속시간, 및 시간경과에 따른 크기 변화를 기록하여 진단한다. 두 위변환검사는 양성 돌발성 체위성 어지러움의 국소진단 에 유용한 검사법 인데 중요한 것은 어떤 두위변환에서 안진이 나오는가 보다 어떤 성분의 안진이 나오는가 하
는 것이다.
특히 이 검사는 뒤반고리관(posterior semicircular canal) 또는 앞반고리관에서 기원하는 양성 돌발성 체위성 어지 러움의 진단에 유용하다. 그러나 예를 들어 양성 돌발성 체위성 어지러움이 의심되는 환자에서 우측 Dix-Hallpike 검사에서 향지성 안진이 나타나더라도 수평성분의 향지 성 안진이 나오는 경우에는 뒤반고리관의 결석이기 보 다는 측반고리관의 반고리결석(canalolithiasis)일 가능성이 높다.
한편 혹시 약물에 의한 어지럼증인지도 확인한다. 또 한 진찰상 안구진탕이나 지시검사(pastpointing) 등 전정 불균형 증상이 있는지 확인한다.
6. 치료
어지럼증의 치료는 형태와 원인에 따라 다양하다. 일 반적으로는 증상 치료이며 근본 원인을 확인하고 교정 하는 것이 치료의 핵심이다. 예를 들어 현기에서는 전정 진정제를 쓰면 호전되지만 전실신과 불균형에서는 반대
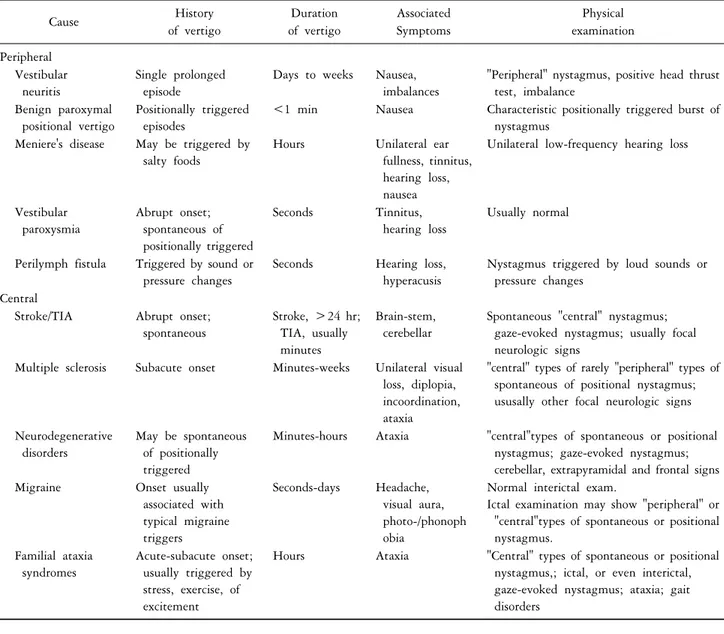
Table 15. Distinguishing among common peripheral and central vertigo syndromes
Cause History
of vertigo
Duration of vertigo
Associated Symptoms
Physical examination Peripheral
Vestibular neuritis
Single prolonged episode
Days to weeks Nausea, imbalances
"Peripheral" nystagmus, positive head thrust test, imbalance
Benign paroxymal positional vertigo
Positionally triggered episodes
<1 min Nausea Characteristic positionally triggered burst of nystagmus
Meniere's disease May be triggered by salty foods
Hours Unilateral ear fullness, tinnitus, hearing loss, nausea
Unilateral low-frequency hearing loss
Vestibular paroxysmia
Abrupt onset;
spontaneous of positionally triggered
Seconds Tinnitus,
hearing loss
Usually normal
Perilymph fistula Triggered by sound or pressure changes
Seconds Hearing loss, hyperacusis
Nystagmus triggered by loud sounds or pressure changes
Central
Stroke/TIA Abrupt onset;
spontaneous
Stroke, >24 hr;
TIA, usually minutes
Brain-stem, cerebellar
Spontaneous "central" nystagmus;
gaze-evoked nystagmus; usually focal neurologic signs
Multiple sclerosis Subacute onset Minutes-weeks Unilateral visual loss, diplopia, incoordination, ataxia
"central" types of rarely "peripheral" types of spontaneous of positional nystagmus;
ususally other focal neurologic signs
Neurodegenerative disorders
May be spontaneous of positionally triggered
Minutes-hours Ataxia "central"types of spontaneous or positional nystagmus; gaze-evoked nystagmus;
cerebellar, extrapyramidal and frontal signs
Migraine Onset usually
associated with typical migraine triggers
Seconds-days Headache, visual aura, photo-/phonoph obia
Normal interictal exam.
Ictal examination may show "peripheral" or
"central"types of spontaneous or positional nystagmus.
Familial ataxia syndromes
Acute-subacute onset;
usually triggered by stress, exercise, of excitement
Hours Ataxia "Central" types of spontaneous or positional nystagmus,; ictal, or even interictal, gaze-evoked nystagmus; ataxia; gait disorders
Figure 1. Dix-Hallpike test.
로 악화된다. 말초성 급성 현기에서는 전정운동을 하면 효과를 보지만 전실신, 불균형, 및 정신과적 어지럼증에 서는 도움이 되지 않는다. 어떤 형태의 어지럼증도 넘어 짐을 조심해야 한다. 특히 노인에서는 잘못 넘어지면 심 각한 문제가 생길 수 있으므로 주변 환경, 실내외 조명, 신발, 보조기, 바닥재 및 기타 안전장치 등에 신경을 써 야 한다.
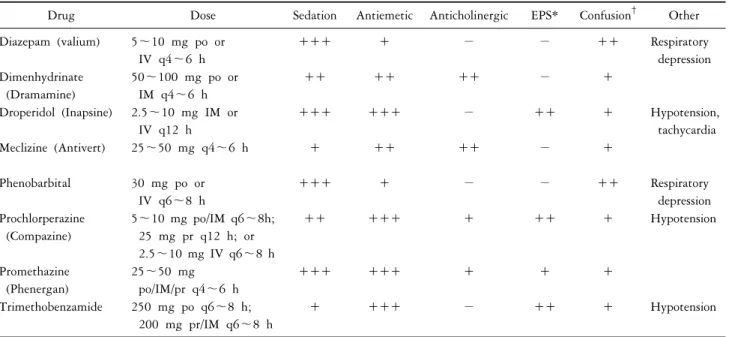
흔히 쓰이는 항현기약의 종류와 용량은 Table 16과 같 다. 약제는 환자의 증상을 보고 임상 경험에 따라 선택 한다. 특히 메스꺼움과 구토를 동반하는 급성 중증 현기 는 정말 힘드므로 항현기약과 더불어 진정제와 항구토 제를 같이 쓰면 효과적이다. 만성 재발성 현기에서는 어 떤 자세와 운동시 현기가 발생하는지를 파악한 다음 전
Table 16. Dosage and common effects of antivertigo medications
Drug Dose Sedation Antiemetic Anticholinergic EPS* Confusion
†Other
Diazepam (valium) 5∼10 mg po or IV q4∼6 h
+++ + − − ++ Respiratory
depression Dimenhydrinate
(Dramamine)
50∼100 mg po or IM q4∼6 h
++ ++ ++ − +
Droperidol (Inapsine) 2.5∼10 mg IM or IV q12 h
+++ +++ − ++ + Hypotension,
tachycardia
Meclizine (Antivert) 25∼50 mg q4∼6 h + ++ ++ − +
Phenobarbital 30 mg po or IV q6∼8 h
+++ + − − ++ Respiratory
depression Prochlorperazine
(Compazine)
5∼10 mg po/IM q6∼8h;
25 mg pr q12 h; or 2.5∼10 mg IV q6∼8 h
++ +++ + ++ + Hypotension
Promethazine (Phenergan)
25∼50 mg po/IM/pr q4∼6 h
+++ +++ + + +
Trimethobenzamide 250 mg po q6∼8 h;
200 mg pr/IM q6∼8 h
+ +++ − ++ + Hypotension
정기관이 적응할 수 있도록 반복적으로 적응운동을 한 다. 적응운동 중 생기는 현기와 자율신경증상을 조절하 기 위해 항현기약을 쓰는 것도 도움이 된다. 그러나 항 현기약은 증상이 호전되면 되도록 빨리 중단하여 전정 기능이 신속하게 회복되도록 하는 것이 좋다.
특히 노인 어지럼증으로 인한 낙상을 예방하기 위해 선 청력과 시력검사를 규칙적으로 하고 주머니에 손을 넣지 않고 천천히 걸으며 굽이 낮고 바닥이 평평한 신발 을 신고 마루에 카펫을 깔며 조명을 밝게 하고 욕실에 몸을 지탱할 손잡이를 설치하며 바닥 물기는 항상 제거 하고 침대 옆에 등을 달아 어두운 상태에서는 나가지 않 게 하며 전선, 걸개, 가구 등 발걸음에 걸리는 장애물을 없애고 넘어질 때는 무릎을 구부리면서 그 자리에 천천 히 주저 앉도록 평소에 교육시킨다.
결 론
나이가 들수록 더 자주 생기는 어지럼증은 임상적으 로 아주 흔한 증상이다. 병적인 어지럼증은 크게 현기, 불균형, 전실신, 및 정신과적 어지럼증 등으로 구분한다.
만성적으로 자주 생기는 노인 어지럼증은 생활에 큰 불 편함을 일으킨다. 특히 노인들은 약물에 의한 귀독성이 잘 생기므로 노인 어지럼증에서는 반드시 약력을 확인 해 봐야 한다, 진찰할 때는 귀, 눈, 심혈관계, 신경계, 및 전정계 이상을 잘 살펴야 한다. 만약 어지럼증이 주관적
이거나 애매할 때는 유발시켜 보는 것도 진단에 도움이 된다. 현기를 억제하는 약을 쓰면 전실신과 불균형이 악 화되기도 한다. 전실신, 불균형, 및 정신과적 어지럼증에 서는 전정운동이나 항현기약이 도움이 되지 않는다. 어 지럼증은 주관적이던 객관적이던 상당히 힘든 증상이므 로 다양한 원인을 파악하여 적극적으로 치료하는 것이 좋다. 특히 노인에서는 어지럼증을 호소한 후 잘 넘어지 므로 항상 주의해야 하며 생활환경도 안전하게 해 두어 야 한다. 노인 어지럼증은 전반적인 신체기능 저하에 의 한 포괄적 증후군이라 생각하고 다각적으로 접근하는 것이 중요하다.
REFERENCES