Electromyographic Analysis of Gluteus Maximus, Gluteus Medius, Hamstring and Erector Spinae Muscles Activity During the
Bridge Exercise With Hip External Rotation in Different Knee Flexion Angles in Healthy Subjects
Kyung-eun Lee1, BPT, PT, Seung-min Baik1, BPT, PT, Chung-hwi Yi2, PhD, PT, Seo-hyun Kim1, BPT, PT
1Dept. of Physical Therapy, The Graduate School, Yonsei University
2Dept. of Physical Therapy, College of Health Science, Yonsei University
Abstract
1)Background: The bridge exercise targets the gluteus maximus (Gmax) and gluteus medius (Gmed).
However, there is also a risk of dominant hamstring (HAM) and erector spinae (ES) muscles.
Objects: To analyze the muscle activity the of Gmax, Gmed, HAM and ES during the bridge exercise with and without hip external rotation in different degrees of knee flexion.
Methods: Twenty-three subjects were participated. The electormyography (EMG) activity of the Gmax, Gmed, HAM and ES muscles was recorded during the exercise. The subjects performed the bridge exercise under four different conditions: (a) with 90˚ knee flexion, without hip external rotation (b) with 90˚ knee flexion, with hip external rotation (c) with 135˚ knee flexion, without hip external rotation (d) with 135˚ knee flexion, with hip external rotation.
Results: There was no significant interaction effect between the degree of knee flexion and hip external rotation. There was a significant main effect for degree of knee flexion in Gmax, HAM muscles activity. Gmax muscle activity was significantly greater in the 135˚ knee flexion position than in the 90˚
knee flexion position (p<.001). While HAM muscle activity was significantly less in 135˚ knee flexion position than in the 90˚ knee flexion position (p<.001). ES muscle activity was significantly less in the 135˚ knee flexion position than in the 90˚ knee flexion position (p=.002). The activity of both the Gmax and Gmed muscles was significantly greater with hip external rotation (p<.001 and p=.005, respectively).
Conclusion: For patients performing the bridge exercise, positioning the knee in 135° of flexion with hip external rotation is effective for improving Gmax and Gmed muscle activity while decreasing HAM, and ES muscle activity.
Key Words: Bridge exercise; Erector spinae; Gluteal muscle; Hamstring; Synergistic muscle.
Introduction
The gluteus maximus (Gmax) is the major ex- tensor and external rotator of the hip and the supe- rior portion also acts as a hip abductor (Choi et al, 2015; Neumann, 2010a). The gluteus medius (Gmed) is the main abductor and external rotator of the hip along with the Gmax. The gluteal muscles comprise about 33% of the hip musculature and play an im-
portant role in normalizing the gait pattern and pos- ture, while preventing the injury and pain reduction (Ito et al, 2003; Lehecka et al, 2017; Marshell et al, 2011; Nelson-Wong et al, 2009).
The Gmax tends to be weak in most people due to a modern lifestyle that involves prolonged sitting (Sahrmann, 2002) and weakness of Gmax may be associated with tightness in the hamastring (HAM) (Massou Arab et al, 2011). In addition, Gmax weak- Corresponding author: Chung-hwi Yi [email protected]
Variables
Age (years) 24.3±2.0a
Height (㎝) 167.2±13.0
Weight (㎏) 65.5±11.8
Body mass index (㎏/㎡) 23.9±7.3
amean±standard deviation.
Table 1. Descriptive characteristics of the partic-
ipants (N=23)
ness during hip extension may lead to the over- compensation by the erector spinae (ES), which can cause the excessive lumbar lordosis and anterior pel- vic tilt (Sahrmann, 2002). Many researchers have re- ported that weakness of gluteal muscles may lead to lower back pain, patellofemoral pain syndrome and valgus positioning of the knee (Biship et al, 2018;
Bolga 2011; Earl et al, 2005; Marshall et al, 2016;
Powers, 2010; Tanamas et al, 2009).
Previous researchers have studied many exercises for activating the gluteal muscles. The bridge ex- ercise is the one of these exercises and it is effec- tive for improving the function of the trunk and lumbopelvic region (Kisner and Colby, 2007).
However, it is associated with the high HAM and ES muscle activation as compensation for gluteal muscle weakness. Choi et al (2015) used target bar for limiting the level of the lumbopelvis and prevent- ing the overactivation of the ES during the bridge exercise. Ekstrom et al (2007) reported that both the unilateral and bilateral bridge exercises produce a the high level of HAM activation. Lehecka et al (2017) studied HAM and gluteal muscle activation during the unilateral bridge in different degrees of knee flexion and found that HAM muscle activity was lower at 135˚ of knee flexion than at 90˚ of knee flexion. Few studies have compared the muscle ac- tivities of the Gmax, Gmed, HAM and ES in differ- ent degrees of knee flexion during the bridge exercise. Although the gluteal muscles can function not only as a hip extensor but also as a hip external rotator, no previous studies have analyzed the gluteal muscle activity when the bridge exercise isperformed
with hip external rotation.
The purpose of this study was to analyze the muscle activity of Gmax, Gmed, HAM, ES during bridge exercise performed with different degrees of knee flexion and after adding hip external rotation.
We hypothesized that the muscle activity of the Gmax and Gmed would be increased by adding hip external rotation and the muscle activity of the HAM and ES would be decreased in 135˚ of knee flexion.
Methods
Participants
Twenty-three healthy adults participated in this study (mean age=24.3, mean height=167.2 ㎝, mean weight=65.5 ㎏, mean body mass index=23.9 ㎏/㎡) (Table 1). Exclusion criteria were as follows: (1) previous fracture, subluxation, or dislocation; (2) his- tory of surgery in the trunk and lower extremity; (3) history of low back pain or lower extremity dys- function such as joint instability, tendinitis, bursitis or any condition that could restrict physical activity.
Prior to the study, written informed consent form was obtain from all subjects, and the study proce- dures were was approved by the Yonsei University Wonju Institutional Review Board (approval number:
1041849-201901-BM-017-01).
Instruments
(1) Surface electromyography
Surface electromyography (EMG) (Noraxon TeleMyo DTS; Noraxon Inc., Scottsdale, AZ, USA) was used to measure muscle activity of Gmax, Gmed, HAM and ES muscles on the participant’s dominant side during the bridge exercise. The sam- pling rate was 1000 ㎐ and a band-pass filter of be- tween 20 ㎐ and 450 ㎐ was used to filter the raw signal. The participant’s skin was shaved and cleaned with alcohol prior to placing the electrodes.
For the Gmax, the electrodes were placed between the trochanter and the sacral vertebrae in the middle
of the muscle at an oblique angle at the level of the trochanter. For the Gmed, the electrodes were placed parallel to the muscle fiber over the proximal third of the distance between the iliac crest and the greater trochanter. For general recordings of the HAM, the electrodes were placed parallel to the muscle in the center of the back of the thigh, ap- proximately halfway between the gluteal fold and the back of the knee. For the ES, the electrodes were placed parallel to the spine, 2 ㎝ apart and approx- imately 2 ㎝ from the spine over the muscle mass (Criswell, 2010). The root mean square (RMS) of the raw EMG data was calculated with a moving win- dow of 50 ㎳.
(2) Three-dimensional motion-tracking system A three-dimensional (3D) motion-tracking system (Noraxon Research MyoMotion; Noraxon Inc., Scottsdale. AZ, USA) was used to measure the ex- ternal rotation angle of the hip during the bridge exercise. Two wireless sensors were placed on the pelvis and anterior region of the thigh. The sampling rate was set at 200 ㎐ and Myo-Research ver. 3.10 (Noraxon Inc., Scottsdale. AZ, USA) was used to analyze the data.
Procedure
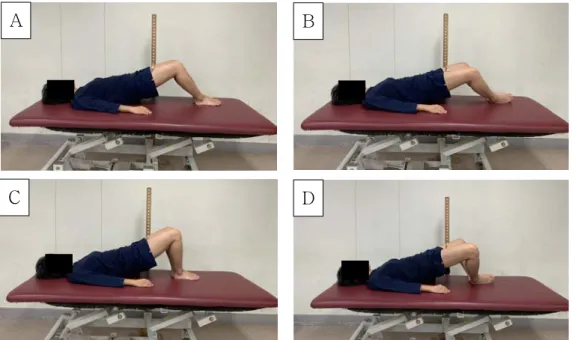
The subjects were instructed on how to perform the bridge exercise within the four different con- ditions, and data were not collected until after the subjects were familiarized with proper positioning. The four different bridge exercises were as follows: (a) with 90˚ of knee flexion, without hip external rotation (b) with 90˚ of knee flexion, with hip external rotation (c) with 135˚ of knee flexion, without hip external ro- tation, and (d) with 135˚ of knee flexion, with hip ex- ternal rotation. The four different bridge exercises were performed in randomized order, which was de- termined using a random number generator in Excel software (Microsoft Corp., Redmond, WA, USA).
(1) Bridge exercise with 90˚ of knee flexion and without hip external rotation
The bridge exercise began with the subjects
placed in a supine position. Both arms were placed on the side of the subject’s body with the palms facing down. Both knees were flexed to 90˚ with the feet hip-width and the flat on the floor. The subjects lifted their hip and trunk until the pelvis and thigh were in line with each other. The wooden target bar was placed at the height of the middle point of the thigh, and the subjects were instructed to form a straight line across the trunk, pelvis and thighs (Figure 1A).
(2) Bridge exercise with 90˚ of knee flexion with hip external rotation
The bridge exercise began with the subjects placed in a supine position. Both arms were placed on the side of the subject’s body with the palms facing down. Both knees were flexed to 90˚ with the sole of the feet facing together. For start position, the subject externally rotated their hips to half of their full range of motion (ROM) in the start posi- tion (Lee et al, 2014). Then the subjects lifted their hips to the target bar, until the trunk and pelvis were in a straight line (Figure 1B).
(3) Bridge exercise with 135˚ of knee flexion and without hip external rotation
The bridge exercise began with the subjects placed in a supine position. Both arms were placed on the side of the subject’s body with the palms facing down. Both knees were flexed to 135˚ with the feet hip-width and flat on the floor. The subjects lifted their hips to the target bar until they made a straight line over the trunk, pelvis and thighs (Figure 1C).
(4) Bridge exercise with 135˚ of knee flexion with hip external rotation
The bridge exercise began with the subjects in a supine position. Both arms were placed on the side of the subject’s body with the palms facing down.
Both knees were flexed to 135˚ with the sole of the feet facing each other. For the start position, the subject externally rotated their hips to half of their full ROM. Then the subjects lifted their hips to the target bar, until the trunk and pelvis formed a straight line (Figure 1D).
A B
C D
Figure 1. The four different birdge exercise (A: with 90˚ of knee flexion and without hip external rotation, B: with 90˚ of knee flexion with hip external rotation, C: with 135˚ of knee flexion and without hip external rotation, D: with 135˚ of knee flexion with hip external rotation).
Data collection
All EMG data were collected during the four dif- ferent bridge exercises for a total 5 seconds and the middle 3 seconds (representing the isometric phase) was used for analyses. Three trials were conducted for each position, and the mean of the three trials was used for analyses. To normalize the EMG data, the RMS of the maximal voluntary isometric con- traction (MVIC) was collected for each muscle in the manual muscle testing position and the data were calculated as a percentage of the MVIC (%MVIC) (Kendall et al, 2005). To ensure the angle of hip ex- ternal rotation was half of subject's full ROM, the target bars were positioned at the lateral sides of both knees and the 3D motion tracking system was used to monitor maintain the hip external rotation angle during the exercises.
Statistical Analysis
Statistical analyses were performed using stat- istical package for the social sciences (SPSS) ver.
22.0 software (SPSS Inc., Armonk, NY, USA). A one-sample Kolmogorov-Smirnov test was performed
to confirm a normal distribution. A two-way re- peated measure analysis of variance (ANOVA) with two within subjects factors (hip external rotation and knee flexion) was used to compare EMG data col- lected from each muscle during the four bridge exercises. A p-value ≤.05 was selected to indicate statistical significance, a paired t-test was performed for post hoc analysis.
Results
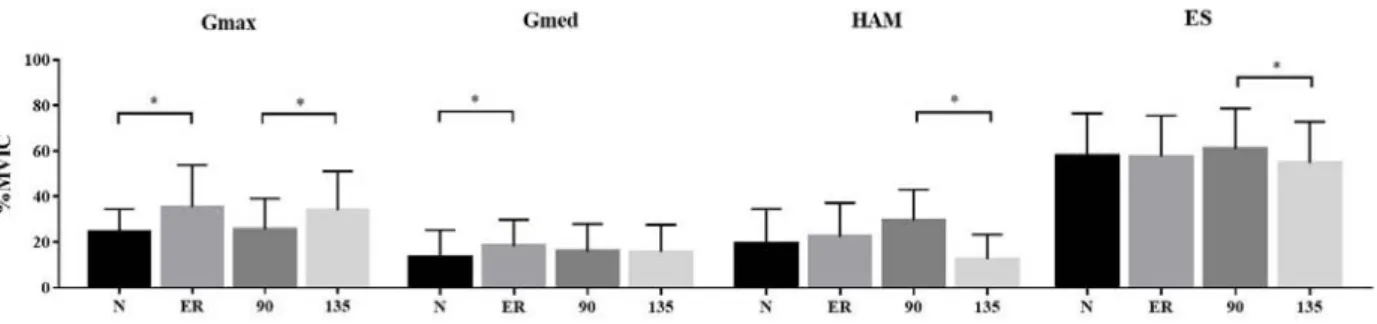
There was no significant interaction effect between the degree of knee flexion and hip external rotation.
A significant main effect was observed between hip external rotation and muscle activity in the Gmax and Gmed muscles. The muscle activity of both the Gmax (F=14.141, p=.001) and Gmed (F=9.491, p=.005) was significantly greater with hip external rotation than without. There was also a significant main ef- fect between the degree of knee flexion and muscle activity in the Gmax, HAM muscles. Gmax muscle activity was significantly greater at 135˚ of knee
Main effect/Interaction effect Gmaxa Gmedb HAMc ESd
F p F p F p F p
Hip external rotation 14.141 .001* .034 .856 3.560 .072 .149 .703 Knee flexion 16.987 .000* 9.491 .005* 77.894 .000* 12.299 .002*
Hip external rotation × knee flexion 2.140 .158 .003 .954 3.176 .089 .000 .989
agluteus maximus, bgluteus medius, chamstrings, derector spinae, *p<.05.
Table 2. The results of two-way repeated ANOVA on muscle activity
Figure 2. Comparison of muscle activity in the Gmax, Gmed, HAM, ES between without hip external rotation and with hip rotation, knee flexion 90˚ and 135˚ during bridge exercise (Gmax:
gluteus maximus, Gmed: gluteus medius, HAM: hamstrings, ES: erector spinae, N: without hip external rotation, ER: with hip external rotation, 90: 90˚ knee flexion, 135: 135˚ knee flexion,
*p<.05).
flexion than 90˚ of knee flexion (F=16.987, p<.001).
Mean while, HAM muscle activity was significantly decreased when the knee flexed at 135˚ versus 90˚
(F=77.894, p<.001). ES muscle activity was also sig- nificantly less in the 135˚ knee flexion position than in the 90˚ position (F=12.299, p=.002) (Figure 2).
Discussion
The purpose of this study was to analyze the muscle activity of the Gmax, Gmed, HAM and ES muscles during the bridge exercise with different de- grees of knee flexion and hip external rotation. The results supported the research hypothesis. The activ- ity of the Gmax and Gmed muscles was significantly increased with hip external rotation than without it during bridge exercise. In addition, HAM and ES muscle activity was decreased at 135˚ of knee flexion compared to knee flexion 90˚. While Gmax activity was increased at 135˚ of knee flexion 135˚ than in the 90˚ position.
Gmax and the posterior fiber of Gmed are power- ful hip external rotators; therefore, maintaining hip
external rotation during the bridge exercise may fa- cilitate their activation. Furthermore, pre-activation of Gmax and Gmed via hip external rotation may pos- sibly increase the activity of these muscles during the exercise. In the starting position for the bridge exercise with added hip external rotation, the sub- ject’s position was supine with the soles of the feet one another, which placed the hips at around half of their full external rotation ROM. Also, this position can lead the hip abduction. By initiating hip external rotation and abduction at the start of the exercise, this could facilitate the pre-activation of the Gmax and Gmed muscles, and as a result, the activity of these muscles may be increased during the bridge exercise. These results were in line with the results of a previous study (Choi et al, 2015), demonstrating the effect of applying a thera-band to initiate iso- metric hip abduction during the bridge exercise which caused the activity of the Gmax to be in- creased by 21.1%. In this study, Gmax and Gmed EMG activities were significantly increased in bridge exercise with hip external rotation by 10.88% and 4.75%, respectively. As a result of the thera-band’s facilitative effect on the activity of the Gmax before
the bridging position, the Gmax activation increased.
However, only Gmax and Gmed were cosidered in this study and there are many hip external rotator that not included in this study (e.g. piriformis, ob- turator internus, gemellus superior and inferior) be- cause of the difficulty of applying EMG. The activ- ities of the HAM and ES muscles were not sig- nificantly affected by the presence or absence of hip external rotation.
Gmax activity was significantly increased in 135˚ of knee flexion than in the 90˚ position. However, the HAM and ES activity was significantly decreased in 135˚ of knee flexion than in 90˚ position. Lehecka et al (2017) reported that the knee extensor moment was reduced at 135˚ of knee flexion during the unilateral bridge exercise, which led to a decrease in HAM ac- tivity from maintaining the knee flexion angle. Our results are similar. In addition, ES activity was sig- nificantly decreased when the knee was flexed at 135˚
compared to 90˚ during the bridge exercise. In sacroil- iac joint, the ES muscle and HAM muscles produce the nutation torque through ES muscle rotate the sac- rum anteriorly while the biceps femoris that one of the HAM muscles rotate the ilium posteriorly. The nutation torque stabilizes the sacroiliac joint. In the 135° knee flexion bridging position, a decrease in HAM activity may lead to a concomitant decrease in ES activity to maintain sacroiliac joint stabilization (Neumann, 2010b). In addition, during the bridge ex- ercise, the Gmax, HAM, and ES act synergistically to lift the pelvis (Choi et al, 2015). A change in the ac- tivity of one muscle may be associated with an in- crease or decrease in activation of a synergistic mus- cle (Jonkers et al, 2003). Thus, a decrease in HAM and ES muscle activity may lead to an increase in Gmax activity.
Meanwhile, the activity of the Gmed was not sig- nificantly different in either knee flexion position. In previous study (Lehecka et al, 2017) also reported that there was no significant difference between 90˚ knee flexion and 135˚ knee flexion during the modified sing-leg bridge exercises. Gmed is primary hip ab-
ductor muscle and secondary hip external rotator muscle (Neumann, 2010b). Thus, knee flexion during birdge exercsie may not affect for activating Gmed muscle.
Our study had several limitations. The primary limitation was that the participants are were all healthy young subjects. Therefore our findings may not be generalizable to a wider population. The sec- ond limitation is that this study had a cross-sec- tional study design. In the future, a longitudinal study would be useful to determine the long-term effects of the different bridge exercise used in this study. Future researchers could examine the long-term effects of bridge exercise with hip external rotation to the patients with back pain, patellofemoral pain who have difficulty to use the hip external rotator.
Conclusion
This research analyzed the muscle activity of the Gmax, Gmed, HAM, and ES during bridge exercises with and without hip external rotation and with dif- ferent degrees of knee flexion. The bridge exercise with hip external rotation and 135° of knee flexion showed preferential activation of the Gmax and Gmed over the HAM and ES. Therefore, this may be more effective than the traditional bridge exercise for increasing gluteal muscle activity while decreas- ing overcompensation with the HAM and ES muscles.
References
Bishop BN, Greenstein J, Etnoyer Slaski, JL, et al.
Electromyographic analysis of gluteus maximus, gluteus medius, and tensor fascia latae during therapeutic exercises with and without elastic resistance. J Sports Phys. 2018:13(4);668-675.
Bolgla LA, Malone TR, Umberger BR et al.
Comparison of hip and knee strength and neu- romuscular activity in subjects with and without patellofemoral pain syndrome. J Sports Phys.
2011;6(4);285-296.
Choi SA, Cynn HS, Yi CH, et al. Isometric hip ab- duction using a Thera-Band alters gluteus max- imus muscle activity and the anterior pelvic tilt angle during bridging exercise. J Electromyogr Kinesiol. 2015;25(2):310-315.
Criswell E. Cram’s Introduction to Surface Electromyography. 2nd ed. Jones & Bartlett Publishers, 2010.
Earl JE, Hertel J, Denegar CR. Patterns of dynamic malalignment, muscle activation, joint motion, and patellofemoral-pain syndrome. J Sport Rehabil.
2005;14(3):216-233.
Ekstrom RA, Donatelli RA, Carp KC. Electromyo- graphic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37(12)754-762.
https://doi.org/10.2519/jospt.2007.2471
Ito J, Moriyama H, Inikuchi S, et al. Human lower limb muscles: An evaluation of weight and fiber size. Okajimas Folia Anat Jpn. 2003;80(2.3):
47-56.
Jonkers I, Stewart C, Spaepen A. The comple- mentary role of the plantarflexors, hamstrings and gluteus maximus in the control of stance limb stability during gait. Gai Posture. 2003;
17(3):264-272.
Kendall FP, McCreary EK, Provance PG, et al.
Muscles: Testing and Function with Posture and Pain. 5th ed. Baltimore: Williams & Wilkins, 2005.
Kisner C, Colby LA, Borstad J. Therapeutic Exercise:
Foundations and Techniques. 7th ed. FA Davis, 2017.
Lee JH, Cynn HS, Kwon OY et al. Different hip rota- tions influence hip abductor muscles activity dur- ing isometric side-lying hip abduction in subjects with gluteus medius weakness. J Electromyogr Kinesiol. 2014;24(2):318-324. https://doi.org/10.1016/
j.jelekin.2014.01.008
Lehecka BJ, Edwards M, Haverkamp R et al. Building a better gluteal bridge: Electromyographic analy- sis of hip muscle activity during modified sin- gle-leg bridges. Int J Sports Phys Ther.
2017;12(4):543-549.
Marshall AR, Noronha MD, Zacharias A, et al.
Structure and function of the abductors in pa- tients with hip osteoarthritis: Systematic review and meta-analysis. J Back Musculoskelet Rehabil.
2006;29(2):191-204. https://doi.org/10.3233/BMR- 150614
Marshall PW, Patel H, Callaghan JP. Gluteus medius strength, endurance, and co-activation in the development of low back pain during prolonged standing. Hum Mov Sci. 2011;30(1):63-73.
https://doi.org/10.1016/j.humov.2010.08.017
Massoud Arab A, RezaNourbakhsh M, Mohammadifar A. The relationship between hamstring length and gluteal muscle strength in individuals with sacroiliac joint dysfunction. J Man Manip Ther.
2011;19(1):5-10. https://doi.org/10.1179/106698110X1 2804993426848
Nelson-Wong E, Flynn T, Callaghan JP. Development of active hip abduction as a screening test for identifying occupational low back pain. J Orthop Sports Phys Ther. 2009;39(9):649-657.
https://doi.org/10.2519/jospt.2009.3093
Neumann DA. Kinesiology of the hip: A focus on muscular actions. J Orthop Sports Phys Ther.
2010a;40(2):82-94. https://doi.org/10.2519/jospt.
2010.3025
Neumann DA. Kinesiology of the Musculoskeletal System: Foundation for Rehabilitation. 2nd ed.
Mosby, 2010b:364-365.
Powers CM. The influence of abnormal hip mechan- ics on knee injury: A biomechanical perspective.
J Orthop Sports Phys Ther. 2010:40(2);42-51.
https://doi.org/10.2519/jospt.2010.3337
Sahrmann S. Diagnosis and Treatment of Movement Impairment Syndromes. Elsevier Health Sciences, 2001.
This article was received August 1, 2019, was re- viewed August 1, 2019, and was accepted September 5, 2019.
Tanamas S, Hanna FS, Cicuttini FM, et al. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A sys- tematic review. Arthritis Rheum. 2009;61(4):
459-467. https://doi.org/10.1002/art.24336