Clinical Features and Prognostic Factors in Elderly Koreans with Advanced Non-Small- Cell Lung Cancer in a Tertiary Referral
Hospital
Background: More than half of cases for advanced non-small-cell lung cancer (NSCLC) occur in elderly patients with a median age at diagnosis of 70 years. The aim of our study was to examine the clinical features and prognostic factors contributing to mortality in elderly patients with advanced NSCLC.
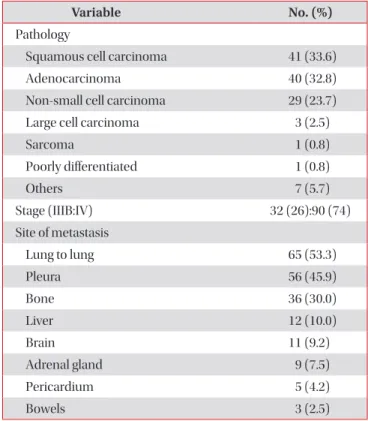
Methods: Following a retrospective review of clinical data, 122 patients aged 70 years and over with a histopathological diagnosis of locally advanced (stage IIIB, n=32) and metastatic (stage IV, n=90) NSCLC between 2005 and 2011 were enrolled.
Results: The median age was 76 years (interquartile range, [IQR], 72−80 years), and 85 (70%) patients were male. Fifty- seven (46%) patients had never smoked, and 17 (19%) were in a malnourished state with a body mass index (BMI) of <18.5 kg/m
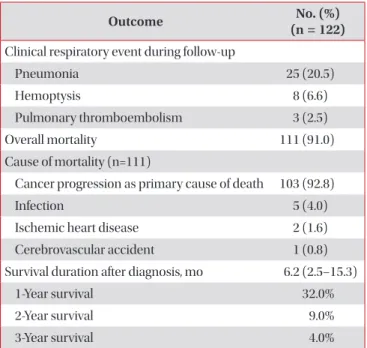
2. The initial treatments included chemotherapy (40%) and radiotherapy (7%), but 57% of the patients received supportive care only. The 1-year survival rate was 32%, and the 3-year survival rate was 4%, with a median survival duration of 6.2 months (IQR, 2.5−15.3 months). Male gender (hazard ratio [HR], 2.2; 95% confidence interval [CI], 1.3−3.9; p=0.005), low BMI (HR, 2.3; 95% CI, 1.3−3.9; p=0.004), and supportive care only (HR, 1.9; 95% CI, 1.2−2.9; p=0.007) were independent predictors of shorter survival based on a Cox proportional hazards model.
Conclusion: Elderly patients with advanced NSCLC had a poor prognosis, particularly male patients, those with a low BMI, and those who received supportive care only.
Keywords: Carcinoma, Non-Small-Cell Lung; Aged; Prognosis; Mortality
Copyright © 2013 The Korean Academy of Tuberculosis and Respiratory Diseases. All rights reserved.
Seo Woo Kim, M.D.
1, Mi Yeon Kim, M.D.
1, Yoon Pyo Lee, M.D.
1, Yon Ju Ryu, M.D., Ph.D.
1, Seok Jeong Lee, M.D.
1, Jin Hwa Lee, M.D., Ph.D.
1, Jung Hyun Chang, M.D., Ph.D.
1and Sung Shine Shim, M.D., Ph.D.
21
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine,
2Department of Radiology, Ewha Medical Center and Ewha Medical Research Institute, Ewha Womans University School of Medicine, Seoul, Korea
Address for correspondence: Yon Ju Ryu, M.D., Ph.D.
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Ewha Medical Center and Ewha Medical Research Institute, Ewha Womans University Mokdong Hospital, Ewha Womans University School of Medicine, 1071 Anyangcheon-ro, Yangcheon-gu, Seoul 158-710, Korea Phone: 82-2-2650-2840, Fax: 82-2-2650-2559, E-mail: [email protected]
Received: Apr. 8, 2013 Revised: May 10, 2013 Accepted: May 27, 2013
cc