Effect of Mirror Therapy Combined with Lower Extremity Muscle Strength Exercise on Gait and Balance of Patients with Chronic Stroke
8
0
0
전체 글
(3)
(4)
(5)
(6)
(7)
(8)
수치
관련 문서
Purpose: This study examined the effects of a virtual reality‐based exercise program on the functional recovery of balance and gait in chronic stroke subjects.. Methods: A
PURPOSE: Balance exercise as well as lower extremity strengthening exercise (LESE) is known to be effective in patients with knee osteoarthritis (KOA). The purpose of this
Background: The purpose of this study was to determine the effects of whole body vibration (WBV) exercise on lower extremity muscle activity and gait ability in stroke
Effects of Sling Exercise Therapy on Trunk Muscle Activation and Balance in Chronic Hemiplegic Patients. The value of the NDT-Bobath method in post-stroke gait
tDCS: 2times aday(morning andafternoon, 5 times a week for 2 weeks(prior to PNMES) PNMES: 2 times a day(morning and afternoon, 5 timesa week for 2 weeks(prior to CIMT) Intensity:
Objective : The purpose of this study is to evaluate the effect of task-oriented mirror therapy involve visual illusion on upper extremity functions in
Koseoglu, "Mirror therapy enhances lower-extremity motor recovery and motor functioning after stroke: a randomized controlled trial," Archives of
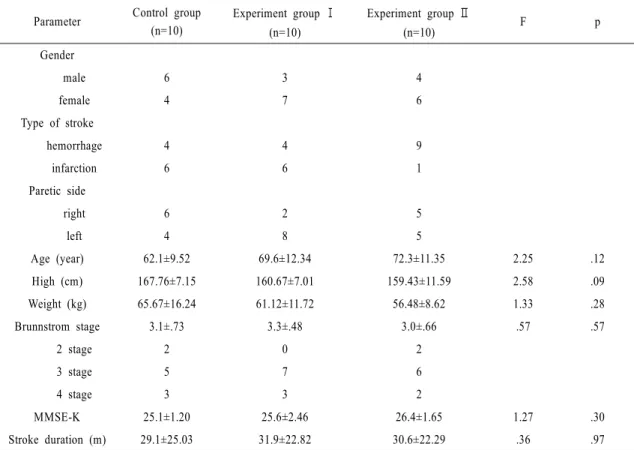
The control group received the general physical therapy including of strengthening and balance exercise five times a week whereas the experimental group received
