Vol. 24, No. 3, 275-285, December 2013
Original Article
Received on August 29, 2013. Revised on October 1, 2013. Accepted on October 1, 2013 Correspondence to: Sang Min Park
Department of Emergency Medicine, Konkuk University Chungju Hospital, Gukwon St. 82, Chungju 380-704, Korea Tel: 82-43-843-3396, Fax: 82-43-840-8965, E-mail: [email protected]
비 외상 환자에서 대량수혈 필요에 대한 예측 인자 분석
유광열1ㆍ김정윤1ㆍ최성혁1ㆍ윤영훈1ㆍ임채승2ㆍ박상민3
고려대학교 구로병원 응급의학과1, 진단검사의학과2, 건국대학교병원 응급의학과3
Prediction of Massive Blood Transfusion at Emergency Department in Non-trauma Patients
Kwang Yul You1, Jung Youn Kim1, Sung Hyuk Choi1, Young Hoon Yoon1, Chae Seung Lim2, Sang Min Park3
Departments of Emergency Medicine1, Laboratory Medicine2, Korea University Medical Center, Seoul, Department of Emergency Medicine, Konkuk University Medical Center3, Chungju, Korea
Background: Many patients received transfusion in emergency department because of blood loss. There are few studies on massive transfusion for non-traumatic patients. This study investigated mortality and risk factor for non-traumatic bleeding patients who received transfusion.
Methods: Non-trauma patients who received transfusion at the emergency department for 3 years from March 2009 to February 2011 were enrolled. The patients who are younger than 15 years, trauma patients, and transfused FFP or platelet alone are excluded. Medical records was investigated retrospectively. We investigated predictive factors for MT on non-trauma patients and predictive factors for mortality on MT patients.
Results: Among 1655 non-trauma patients, 150 patients (9.24%) received MT. The age of MT group was younger than that of non-MT group and systolic bloor pressure, diastolic blood pressure, mean arterial pressure were significantly lower. Base excess, pH, lactate levels were significantly different between MT and non-MT group.
Intensive care unit length of stay was longer, mortality of 24 hours was higher and survival discharge was lower than non-MT group. Mortality rate of MT group was 20.7% which was significantly higher than non-MT group’s 9.3%. FFP:RBC ratio was higher in MT group than non-MT group. Among the MT group, non-survival group used higher FFP:RBC ratio product than survival group. On multivariate analysis, sBP, MAP, lactate, pH, BE were significant as predictors of MT.
Conclusion: For non-trauma patients in emergency department, if sBP, MAP, lactate, pH, BE are abnormal, massive transfusion could be expected. Like trauma patients, basic scoring system that can predict MT would be necessary and useful. (Korean J Blood Transfus 2013;24:275-285)
Key words: Non-trauma, Massive blood transfusion, Prediction
Introduction
The chief complaint of many patients admitted to emergency departments is hemorrhage, which can become the main cause of death. As the general treatment for these patients is to recover the blood lost, resuscitation generally begins with a crystalloid or colloid, followed by blood transfusion when re- quired, and if severe blood loss is seen or expected, massive blood transfusion based on the loss is car- ried out. The main cause of death in patients aged 18∼45 years is trauma, and the majority of the liter- ature reports traumatic hemorrhage as the main cause of death in hemorrhage patients in emergency departments.1-3) Thus, studies on massive blood transfusion had mostly based on trauma patients. For example, the risk factors capable of predicting com- plications in trauma patients receiving massive blood transfusion, a clinical scoring system that can predict the need for massive blood transfusion in trauma pa- tients,4,5) a model capable of estimating death in massively transfused trauma patients,6) prognosis ac- cording to the FFP:RBC ratio,7,8) or the fresh frozen plasma to red blood cell (FFP:RBC) ratio,1,9-12) in massively transfused trauma patients. However, oth- er large numbers of critically ill patients admitted to emergency departments require massive blood trans- fusion due to non-traumatic massive hemorrhage, and there had been only a few reports related to massive blood transfusion in these patients.
Therefore, a study on massive hemorrhage and blood transfusion in non-trauma patients is required, and through such a study, a better long-term prog- nosis can be expected based on the development of an initial acute-phase treatment protocol. This study
aimed to determine the clinical characteristics of non-trauma, transfused patients in emergency depart- ments, the factors related to received massive blood transfusion in non-trauma patients and the factors re- lated to death in non-trauma patients who received massive blood transfusion.
Materials and Methods
This study was carried out in the emergency med- ical center in Korea University Guro hospital, a ter- tiary medical institution visited by approximately 60,000 patients annually. Among the patients who visited the center over the span of 3 years (March 2009∼February 2012), we targeted non-trauma adult patients who received blood transfusions.
Non-trauma patients defined as patients categorized as non-trauma (eg. disease, poisoning, others) at ini- tial triage by trained nurse in ED. All patients with an RBC prescription code were included, while pe- diatric patients under 15 years old and trauma pa- tients were excluded. Having selected 1655 patients for the study, we carried out retrospective analysis of their medical records.
Massive blood transfusion patients were defined as patients who received ≥5 units of blood within 6 hours,4,13,14) Demographics, vital signs, laboratory tests, transfused RBC and FFP volume, ICU stay du- ration, and mortality were investigated. First re- corded data were used for vital signs analysis.
Patients were divided into 2 groups whose re- spective characteristics were compared: those who received massive blood transfusion (massively trans- fused group), and those who received general blood transfusion (general transfusion group). The pre-
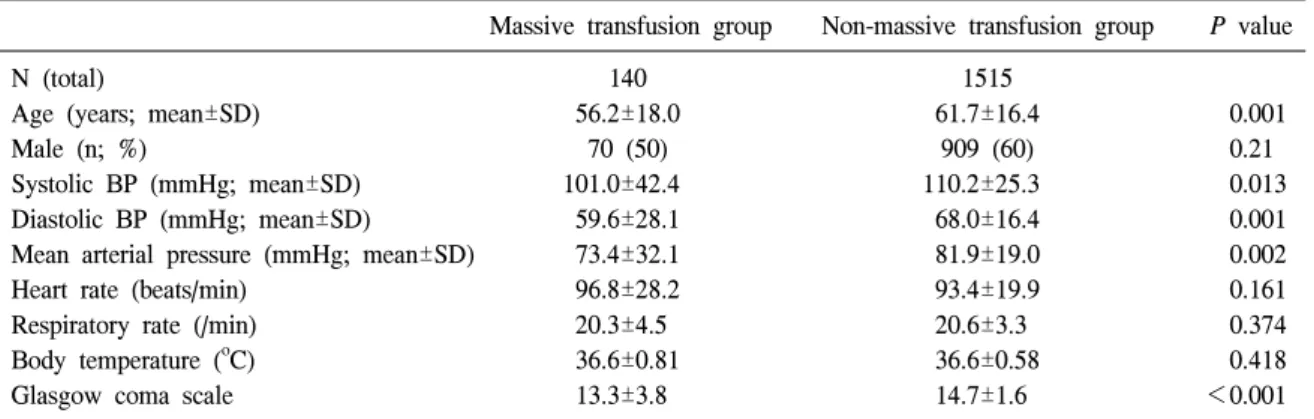
Table 1. Demographic & physiologic data of patients
Massive transfusion group Non-massive transfusion group P value
N (total) 140 1515
Age (years; mean±SD) 56.2±18.0 61.7±16.4 0.001
Male (n; %) 70 (50) 909 (60) 0.21
Systolic BP (mmHg; mean±SD) 101.0±42.4 110.2±25.3 0.013
Diastolic BP (mmHg; mean±SD) 59.6±28.1 68.0±16.4 0.001
Mean arterial pressure (mmHg; mean±SD) 73.4±32.1 81.9±19.0 0.002
Heart rate (beats/min) 96.8±28.2 93.4±19.9 0.161
Respiratory rate (/min) 20.3±4.5 20.6±3.3 0.374
Body temperature (oC) 36.6±0.81 36.6±0.58 0.418
Glasgow coma scale 13.3±3.8 14.7±1.6 <0.001
dictive factors of the massively transfused patients were identified. In addition, the massively transfused patients were divided into survival and non-survival groups, and the respective characteristics were com- pared.
SPSS 14.0 (SPSS, Inc, an IBM Company, Chicago, Illinois, USA)was used for statistical analysis, and the results are presented as mean±standard deviation (SD), the chi-squared test and Student’s t-test were carried out for comparison between 2 groups, and logistic regression analysis was used to obtain risk factors. Statistical significance was defined as P
<0.05.
Results
We studied total 1655 patients, of which 140 pa- tients received massive blood transfusion.
1. Characteristics of targeted patients
Over 3 years (March 2009∼February 2012), 1655 non-trauma patients aged 15 years or more received blood transfusions at the emergency department.
Among them, 140 (8.5%) were in the massive blood transfusion group and 1515 (91.5%) were in the gen- eral blood transfusion group. In the massively trans- fused group, the systolic blood pressure (BP) (P=
0.013), diastolic BP (P=0.001), mean arterial pres- sure (MAP) (P=0.002), and Glasgow coma scale (GCS) (P≤0.001) were statistically significantly low, and ICU length of stay (P=0.047), lactate (P=
0.005), pH (P<0.001), and BE (P=0.003) were sig- nificantly high as compared to the general trans- fusion group. Conversely, there were no significant differences in the hemoglobin (Hb) (P=0.659), hem- atocrit (Hct) (P=0.465), platelet (P=0.566), pro- thrombin time and international normalized ratio (PT INR) (P=0.111), and activated partial thromboplastin time (aPTT) (P=0.187) between the 2 groups (Table 1, 2).
The most common cause of blood loss was the hemorrhage of gastrointestinal (GI) origin for both groups. Then, in the order of decreasing frequency, the massively transfused group required transfusion due to obstetric and gynecologic hemorrhage, ane- mia, and hemorrhage by malignancy while the gen-
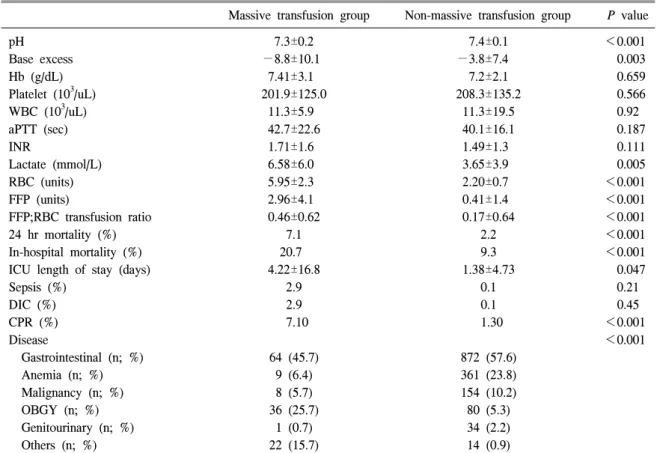
Table 2. Laboratory & clinical data of patients
Massive transfusion group Non-massive transfusion group P value
pH 7.3±0.2 7.4±0.1 <0.001
Base excess −8.8±10.1 −3.8±7.4 0.003
Hb (g/dL) 7.41±3.1 7.2±2.1 0.659
Platelet (103/uL) 201.9±125.0 208.3±135.2 0.566
WBC (103/uL) 11.3±5.9 11.3±19.5 0.92
aPTT (sec) 42.7±22.6 40.1±16.1 0.187
INR 1.71±1.6 1.49±1.3 0.111
Lactate (mmol/L) 6.58±6.0 3.65±3.9 0.005
RBC (units) 5.95±2.3 2.20±0.7 <0.001
FFP (units) 2.96±4.1 0.41±1.4 <0.001
FFP;RBC transfusion ratio 0.46±0.62 0.17±0.64 <0.001
24 hr mortality (%) 7.1 2.2 <0.001
In-hospital mortality (%) 20.7 9.3 <0.001
ICU length of stay (days) 4.22±16.8 1.38±4.73 0.047
Sepsis (%) 2.9 0.1 0.21
DIC (%) 2.9 0.1 0.45
CPR (%) 7.10 1.30 <0.001
Disease <0.001
Gastrointestinal (n; %) 64 (45.7) 872 (57.6)
Anemia (n; %) 9 (6.4) 361 (23.8)
Malignancy (n; %) 8 (5.7) 154 (10.2)
OBGY (n; %) 36 (25.7) 80 (5.3)
Genitourinary (n; %) 1 (0.7) 34 (2.2)
Others (n; %) 22 (15.7) 14 (0.9)
Abbreviations: Hb, hemoglobin; WBC, white blood cell; aPTT, activated partial thromboplastin time; INR, international normalized ratio; RBC, red blood cell; FFP, fresh frozen plasma; DIC, disseminated intravascular coagulopathy; CPR, cardiopulmonary resuscitation; OBGY, obstetric gynecology.
eral transfusion group required transfusion due to anemia, malignancy, obstetric and gynecologic hem- orrhage, and urologic hemorrhage.
As the massively transfused group received 5.95±
2.3 units of RBC and the general transfusion group received 2.20±0.7 units, the former accounted for 20.01% of the total RBC units transfused to non- trauma patients in entire study period, and having re- ceived 2.96±4.1 units of FFP compared to the 0.41±
1.4 units transfused to the general blood transfusion group, the massive blood transfusion group received 39.67% of the FFP transfused.
In addition, survival analysis at 50 days de- termined that the survival rate of the massively transfused group (9.3%) was lower as compared to the general transfusion group (20.7%) (Fig. 1) (P
<0.001).
Fig. 1. Cox regression 50 days survival curve of massive transfusion (MT) patients vs. general transfusion patients (non-MT) (9.3% vs. 20.7.%, P
<0.001). Abbreviations: MT, massive transfusion;
Non-MT, non-massive transfusion.
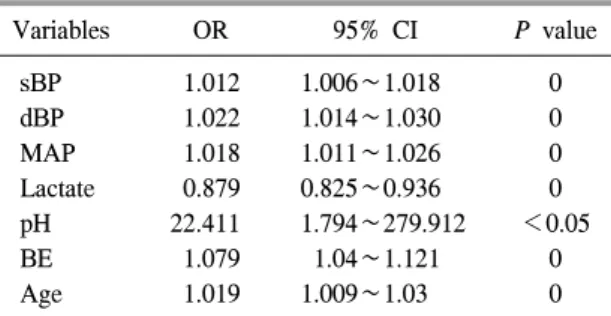
Table 3. Regression coefficients and ORs for prediction of massive blood transfusion
Variables OR 95% CI P value
sBP 1.012 1.006∼1.018 0
dBP 1.022 1.014∼1.030 0
MAP 1.018 1.011∼1.026 0
Lactate 0.879 0.825∼0.936 0
pH 22.411 1.794∼279.912 <0.05
BE 1.079 1.04∼1.121 0
Age 1.019 1.009∼1.03 0
Abbreviations: sBP, systolic blood pressure; dBP, diastolic blood pressure; MAP, mean arterial pressure; BE, base excess.
2. Predictive factors of massive blood transfusion
For predictive factors of massive blood trans- fusion obtained by logistic regression analysis, there were significant differences in the pH OR of 22.411, sBP odds ratio (OR) of 1.012, dBP OR of 1.022, MAP OR of 1.18, BE OR of 1.079, age OR of 1.019, and lactate OR of 0.879 (Table 3).
3. Survival rate predictive factors in massive blood transfusion
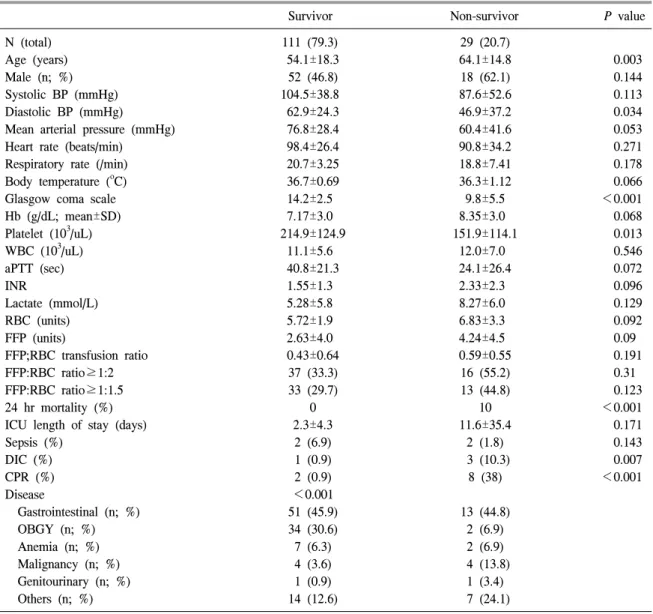
Subgroup analysis of the massively transfused group involved dividing the group into survival and non-survival groups; among the 140 patients who re- ceived massive blood transfusion, 111 (79.3%) sur- vived, while 29 (20.7%) did not. Age (P=0.003) was statistically significantly low, and diastolic BP (P=
0.034), platelet (P=0.013), and GCS (P<0.001)
were significantly high in the survival group as com- pared to the non-survival group. Meanwhile, there was no significant difference for Hb (P=0.068), Hct (P=0.055), lactate (P=0.129), PT INR (P=0.096), and aPTT (P=0.072) (Table 4).
Identified etiologies in the order of decreasing fre- quency were hemorrhage of GI origin and obstetric and gynecologic origin for the survival group, while for non-survival group, they were of GI origin, and hemorrhage due to malignancy.
Discussion
As hemorrhage is a highly emergent situation that can be life threatening, it is also the common chief complaint of many patients admitted to emergency department. Moreover, traumatic hemorrhage is the most common reason that massive blood transfusion is required, followed by ruptured aneurysm of the aorta and GI bleeding.15) In previous study on mas- sive blood transfused patients, the mortality was once reported as 93% in 1971,7) but recently re-
Table 4. Characteristics of survivors and non-survivors in massive transfusion
Survivor Non-survivor P value
N (total) 111 (79.3) 29 (20.7)
Age (years) 54.1±18.3 64.1±14.8 0.003
Male (n; %) 52 (46.8) 18 (62.1) 0.144
Systolic BP (mmHg) 104.5±38.8 87.6±52.6 0.113
Diastolic BP (mmHg) 62.9±24.3 46.9±37.2 0.034
Mean arterial pressure (mmHg) 76.8±28.4 60.4±41.6 0.053
Heart rate (beats/min) 98.4±26.4 90.8±34.2 0.271
Respiratory rate (/min) 20.7±3.25 18.8±7.41 0.178
Body temperature (oC) 36.7±0.69 36.3±1.12 0.066
Glasgow coma scale 14.2±2.5 9.8±5.5 <0.001
Hb (g/dL; mean±SD) 7.17±3.0 8.35±3.0 0.068
Platelet (103/uL) 214.9±124.9 151.9±114.1 0.013
WBC (103/uL) 11.1±5.6 12.0±7.0 0.546
aPTT (sec) 40.8±21.3 24.1±26.4 0.072
INR 1.55±1.3 2.33±2.3 0.096
Lactate (mmol/L) 5.28±5.8 8.27±6.0 0.129
RBC (units) 5.72±1.9 6.83±3.3 0.092
FFP (units) 2.63±4.0 4.24±4.5 0.09
FFP;RBC transfusion ratio 0.43±0.64 0.59±0.55 0.191
FFP:RBC ratio≥1:2 37 (33.3) 16 (55.2) 0.31
FFP:RBC ratio≥1:1.5 33 (29.7) 13 (44.8) 0.123
24 hr mortality (%) 0 10 <0.001
ICU length of stay (days) 2.3±4.3 11.6±35.4 0.171
Sepsis (%) 2 (6.9) 2 (1.8) 0.143
DIC (%) 1 (0.9) 3 (10.3) 0.007
CPR (%) 2 (0.9) 8 (38) <0.001
Disease <0.001
Gastrointestinal (n; %) 51 (45.9) 13 (44.8)
OBGY (n; %) 34 (30.6) 2 (6.9)
Anemia (n; %) 7 (6.3) 2 (6.9)
Malignancy (n; %) 4 (3.6) 4 (13.8)
Genitourinary (n; %) 1 (0.9) 1 (3.4)
Others (n; %) 14 (12.6) 7 (24.1)
Abbreviations: BP, blood pressure; Hb, hemoglobin; WBC, white blood cell; aPTT, activated partial thromboplastin time;
INR, international normalized ratio; RBC, red blood cell; FFP, fresh frozen plasma; DIC, disseminated intravascular coagulopathy; CPR, cardiopulmonary resuscitation; OBGY, obstetric gynecology.
ported as being 25∼45%.8,15) In particular, the death rate in massive blood transfusion for trauma patients is known to reach 40.3%,16) and a study targeting
all traumatic and non-traumatic causes reported a death rate of 34.4%,5) whereas that in this study was 20.7%, which indicates that the death rate is lower
in non-trauma patients as compared to trauma patients.
Currently, studies on massive hemorrhage and massive blood transfusion have mainly been carried out on trauma patients, and there are few studies on non-trauma patients.17) Thus, there are many reports on the definition of massive blood transfusion, treat- ment, complications after treatment, and so on in trauma patients, but few similar data for non-trauma patients to date.17) This study targeted non-trauma patients at the emergency department who had re- ceived blood transfusion; in particular, the clinical characteristics and risk factors of massively trans- fused patients were investigated.
In this study, approximately 0.97% of all the pa- tients who visited the emergency department re- ceived blood transfusion. Studies such as that of Rose et al.17) reported that around 1% of transfused patients received massive blood transfusion, and 0.4
∼3% of trauma patients received massive blood transfusion.5,16) However, massively transfused pa- tients are known to account for the greatest total blood transfusion amount, and have higher death rates as compared to general transfusion patients, in- dicating that it is important to study the clinical characteristics and predictive factors of massively transfused patients.
In this study, 140 patients, who comprised 8.45%
of the 1655 patients studied, received massive blood transfusion. However, among the total 4163 units of RBC transfused, almost 833 units were for mas- sively transfused patients, as were 39.67% of FFP and 32.2% of platelets, which indicated that a pro- portionately large amount of blood products were used. According to the investigation by Rose et al.17)
into trauma and non-trauma patients, 1.3% of pa- tients received massive blood transfusion and 7% of the total sum of transfused RBC were for the mas- sively transfused patients.
Also in this study, there was a significant differ- ence in the in-hospital mortality, being 20.7% in massively transfused patients and 9.3% in general transfusion patients. Although the death rate is low compared to that of post-massive blood transfusion in trauma patients, it remains a significantly high rate when compared with the general blood trans- fusion group.
Mitra et al.4) have stated that the predictive factors mainly identified in studies targeting trauma patients are pulse rate, systolic BP, and type of damage.16) In this study, high pulse rate, low BP, high lactate value, and low BE at initial admission emerged as the predictive factors. Although massive blood trans- fusion and general blood transfusion differ in terms of the cause of hemorrhage, the risk factors of non-trauma patients to massive blood transfusion are seems similar to that of trauma patients.
The definition of massive blood transfusion is not unified.16) In trauma patients, massive hemorrhage is generally defined as the loss of whole body fluid within 24 hours or loss of half of the total amount of blood in 3 hours, or when there is hemorrhage of 150 mL per minute. Additionally, the definition of massive blood transfusion is where ≥10 units packed RBC (pRBC) are transfused within 24 hours, or when 4 units per hour are transfused, but as defi- nitions are selectively used in some studies and the above definitions may not reflect the acute re- suscitative phase of treatment appropriately, there are acute definitions modified with the criterion of
a small amount of pRBC being transfused within short period of time, such as 5 units of pRBC within the first 4 hours, ≥10 units of pRBC within 6 hours, or ≥8 units of pRBC within 12 hours.4,13) As this study targeted emergency department patients, and considering the time spent in the emergency depart- ment, massively transfused patients were defined as patients who received ≥5 units of blood within the first 6 hours in this study.4,13,14)
In descending order of frequency, the causes of blood transfusion for non-trauma patients in the emergency department were GI bleeding, anemia, malignancy, obstetric and gynecologic hemorrhage, and urologic bleeding, and GI bleeding and obstetric and gynecologic causes were the most common rea- sons for massive blood transfusion. Many in the non-survival group required transfusion due to GI causes, whereas obstetric and gynecologic hemor- rhage composed only 6.9% of the causes of patients despite its need for massive blood transfusion.
Although detailed analysis was not carried out re- garding this cause, it is perhaps because the patients who were transfused due to obstetric and gyneco- logic hemorrhage were relatively young and healthy without underlying disease as compared to the pa- tients with GI bleeding, therefore there was a higher possibility of full recovery for these patients after the hemorrhage was treated. In addition, as hemor- rhage due to malignancy was the second most fre- quent reason for transfusion among the non-survival group, and that there was not much difference in the parameters that imply clotting disorders, such as PT, aPTT, platelet values, compared to survival group, we may presume that death is due to the underlying disease itself rather than complications due to clot-
ting disorders or massive blood transfusion in mas- sively transfused, non-trauma patients. And for fu- ture studies, this can be used as research material on clotting disorders followed by massive blood transfusion in non-trauma patients.
The FFP:RBC ratio in the non-survival group was statistically significantly high; more FFP was trans- fused in massive blood transfusion or poor patient condition. Recent studies have reported cases where the FFP:RBC ratio gradually increases up to 1:1;5,11,12,18) maintenance of the appropriate amount is considered necessary as excessive FFP may in- crease volume, augmenting hemorrhage, and because it goes against the permissive hypotension theory.
According to our results, among non-trauma pa- tients who received blood transfusion after admit- tance to the emergency department, massive blood transfusion should be expected when the systolic and diastolic BP, MAP, BE, pH, and the age of the pa- tient is lower, and the lactate value is higher; thus, more aggressive treatment and monitoring would be required for patients who meet the above conditions, keeping massive blood transfusion in mind.
As this was a retrospective study of medical re- cords, the limitations of this study are that the chro- nological relationships between the predictive factors and massive blood transfusion may not be clear;
thus, we believe that a prospective multicenter study is required in the future. Second, information regard- ing whether certain treatment such as surgical treat- ment or non-invasive treatment resulted in better prognosis for patients who required massive blood transfusion was not available because we did not an- alyze progressions according to the type of treatment received by the massively transfused patients. Third,
we did not investigated transfusion related complica- tions such as hemolysis, fever, skin reaction, etc. So it is possible that transfusion related complications affect prognosis of transfused patients and then the result could be influenced.
As only a simple comparison and predictive fac- tors were obtained in this study, a prospective multi- center study carried out based on the present results may enable the development of a scoring system to estimate massive blood transfusion, and accordingly, the patient may undergo early treatment to effect a positive change in the death rate and prognosis.
This study identified the characteristics of mas- sively transfused, non-trauma patients, and the pre- dictive factors of massive blood transfusion for pa- tients in the emergency department were confirmed.
Conclusively, among non-trauma patients who re- quire blood transfusion after being admitted to an emergency medical center, massive transfusion may be predicted when such patients have lower systolic and diastolic BP, MAP, BE, pH, and age, and higher lactate value. Based on the present results, future prospective multicenter studies may be able to de- termine early treatment protocols or prognosis deter- mination when blood transfusion is deemed neces- sary for non-trauma patients in emergency medical centers through the development of a clinical scoring system similar to that used for trauma patients.
Summary
배경: 많은 환자들이 출혈을 주소로 응급실에 내원하며 수혈을 받는다. 대량수혈에 대한 많은 연구들은 이에 대한 예측인자 또는 임상적으로 적용 가능한 scoring system 등에 관한 연구가 많
으며 이들 대부분은 외상 환자만을 대상으로 진 행되어 왔고, 비 외상 환자를 대상으로 하는 대량 수혈에 관한 연구는 거의 없는 실정이다. 이 연구 에서는 수혈환자 중 비 외상 환자를 대상으로 임 상적 특성 및 사망률, 대량수혈에 대한 위험인자 등을 조사하였다.
방법: 서울지역에 위치한 3차 병원인 고려대학 교 부속 구로병원에 2009년 3월부터 2011년 2월 까지 3년 동안 내원한 환자 중에서 수혈을 시행 받은 비 외상 환자를 대상으로 의무기록을 후향 적으로 분석하여 연구를 진행하였다. 15세 미만 이거나 외상 환자이거나 신선동결혈장 및 혈소판 을 단독으로 투여 받은 환자는 제외하였다. 대량 수혈은 응급실 내원 후 6시간 내 5단위 이상을 수 혈한 경우로 정의하였다. 비 외상 환자에서 대량 수혈을 예측할 수 있는 예측 인자와 대량수혈을 받은 환자들에서 사망률에 대한 예측 인자를 조 사하였다.
결과: 연구 기간 동안 총 1,655명의 비 외상 환 자가 수혈을 받았고, 그 중에서 140명(9.24%)이 대량수혈을 받았다. 대량수혈군에서 중환자실 재 실 기간은 더 길었고, 사망률은 높았다. 두 군 모 두에서 위장관출혈이 가장 많은 원인을 차지했 다. FFP:RBC 비는 대량수혈군에서 비 대량수혈 군에 비해 더 높았다. 대량수혈군 중에서 비 생존 군이 생존군에 비해 FFP:RBC 비가 더 높았다. 대 량수혈에 대한 예측인자로는 수축기혈압, 평균동 맥압, 젖산, pH, Base excess가 의미 있는 결과를 보였다.
결론: 응급실에 내원하는 비외상환자에서 대 랑수혈군의 예후는 비 대량수혈군에 비해 좋지 않았다. 응급실에 내원하여 수혈을 시행 받은 비 외상환자 중 수축기혈압, 평균동맥압, 젖산, Base excess, pH가 비정상일수록 대량수혈을 예상할 수 있을 것이다. 이는 외상환자에서와 같이 대량
수혈을 예측하는 clinical scoring system 등에 적용 하여 조기 치료방침이나 예후를 판정하는데 도움 이 될 것이다.
References
1. Borgman MA, Spinella PC, Perkins JG, Grathwohl KW, Repine T, Beekley AC, et al.
The ratio of blood products transfused affects mortality in patients receiving massive trans- fusions at a combat support hospital. J Trauma 2007;63:805-13
2. Acosta JA, Yang JC, Winchell RJ, Simons RK, Fortlage DA, Hollingsworth-Fridlund P, et al.
Lethal injuries and time to death in a level I trauma center. J Am Coll Surg 1998;186:528-33 3. Sauaia A, Moore FA, Moore EE, Moser KS,
Brennan R, Read RA, et al. Epidemiology of trauma deaths: a reassessment. J Trauma 1995;
38:185-93
4. Mitra B, Rainer TH, Cameron PA. Predicting massive blood transfusion using clinical scores post-trauma. Vox Sang 2012;102:324-30 5. Nunez TC, Dutton WD, May AK, Holcomb JB,
Young PP, Cotton BA. Emergency department blood transfusion predicts early massive trans- fusion and early blood component requirement.
Transfusion 2010;50:1914-20
6. Barbosa RR, Rowell SE, Sambasivan CN, Diggs BS, Spinella PC, Schreiber MA, et al. A predictive model for mortality in massively transfused trauma patients. J Trauma 2011;71(2 Suppl 3):S370-4
7. Wilson RF, Mammen E, Walt AJ. Eight years of experience with massive blood transfusions.
J Trauma 1971;11:275-85
8. Campos A, Muñoz M, García-Erce JA, Ramírez
G. Incidence and mortality of massive trans- fusion in a university hospital: study of the period 2001-2005. Med Clin (Barc) 2007;129:
366-71
9. Sperry JL, Ochoa JB, Gunn SR, Alarcon LH, Minei JP, Cuschieri J, et al. Inflammation the Host Response to Injury Investigators. An FFP:
PRBC transfusion ratio >/=1:1.5 is associated with a lower risk of mortality after massive transfusion. J Trauma 2008;65:986-93
10. Borgman MA, Spinella PC, Holcomb JB, Blackbourne LH, Wade CE, Lefering R, et al.
The effect of FFP:RBC ratio on morbidity and mortality in trauma patients based on transfusion prediction score. Vox Sang 2011;101:44-54 11. Kashuk JL, Moore EE, Johnson JL, Haenel J,
Wilson M, Moore JB, et al. Postinjury life threatening coagulopathy: is 1:1 fresh frozen plasma:packed red blood cells the answer? J Trauma 2008;65:261-70
12. Scalea TM, Bochicchio KM, Lumpkins K, Hess JR, Dutton R, Pyle A, et al. Early aggressive use of fresh frozen plasma does not improve out- come in critically injured trauma patients. Ann Surg 2008;248:578-84
13. Levi M, Fries D, Gombotz H, van der Linden P, Nascimento B, Callum JL, et al. Prevention and treatment of coagulopathy in patients re- ceiving massive transfusions. Vox Sang 2011;
101:154-74
14. Mitra B, Cameron PA, Gruen RL, Mori A, Fitzgerald M, Street A. The definition of massive transfusion in trauma: a critical variable in examining evidence for resuscitation. Eur J Emerg Med 2011;18:137-42
15. Harvey MP, Greenfield TP, Sugrue ME, Rosenfeld D. Massive blood transfusion in a tertiary referral hospital. Clinical outcomes and
haemostatic complications. Med J Aust 1995;
163:356-9
16. Fuller G, Bouamra O, Woodford M, Jenks T, Stanworth S, Allard S, et al. Recent massive blood transfusion practice in England and Wales: view from a trauma registry. Emerg Med J 2012;29:118-23
17. Rose AH, Kotzé A, Doolan D, Norfolk DR,
Bellamy MC. Massive transfusion--evaluation of current clinical practice and outcome in two large teaching hospital trusts in Northern England.
Vox Sang 2009;97:247-53
18. Mitra B, Mori A, Cameron PA, Fitzgerald M, Paul E, Street A. Fresh frozen plasma (FFP) use during massive blood transfusion in trauma resuscitation. Injury 2010;41:35-9