Abstract : Background : Puerarin, the main component of kudzu root, has been shown to lower blood glucose levels in vivo and in vitro. However, no clinical trials were performed in diabetic patients. The purpose of this study was to determine whether kudzu root lowers blood glucose or hemoglobin A1c in diabetic patients.
Methods : We performed a retrospective study to evaluate whether the use of daily herbal medicine including kudzu root with conventional therapy lowers fasting blood glucose, as compared to conven-
회원학술보고
갈근 함유탕제의 혈당 강하 효과
김종윤, 김진숙
a, 정지현
b, 김정태
c, 윤현옥
d�, 유기연
b�서울대학교병원 약제부, 한국한의학연구원
a, 동덕여자대학교 약학대학
b, 경희대학교 약학대학 강동경희대학교병원
c, 경상대학교 약학대학
dEffectiveness of Herbal Medicines Containing Kudzu Root as a Principal Ingredient in Patients with Diabetes Mellitus
Jong Yoon Kim, Jin Sook Kim
a, Ji Hyun Chung
b, Jung Tae Kim
c, Hyon Ok Yoon
d�and Ki Yon Rhew
b�Seoul National University Hospital, Seoul, Korea
Korea Institute of Oriental Medicine Herbal TKM-Based Herbal Drug Research Group, Daejeon, Korea
aCollege of Pharmacy, Dongduk Women’s University, Seoul, Korea
bCollege of Pharmacy, Kyung Hee University Hospital at Gangdong, Seoul, Korea
cCollege of Pharmacy, Research Institute of Pharmaceutical Sciences, Gyeongsang National University, Jinju, Korea
d투고일자 2014.10.27; 심사완료일자 2014.11.17; 게재확정일자 2014.11.28
�교신저자 유기연 Tel:02-940-4519 E-mail:[email protected] 윤현옥 Tel:055-772-2422 E-mail:[email protected]
As the worldwide diabetic rate rises, the search for dietary adjuncts to treat this life- altering disease has become extensive. Also the mortality of lifestyle-related diseases such as diabetes and cardiovascular disease has con- siderably increased in many countries.
1),2)Diabetic Mellitus (DM) is the fifth-leading cause of death all over the world and con- tributes to the leading causes of death, cancer and cardiovascular disease (CVD). In addition, glycemic management still remains a corner- stone of DM care, although the co-manage- ment of atherosclerosis, cardiovascular risk reduction, and prevention of long-term conse-
quences associated with DM are now well rec- ognized to improve long-term survival.
3)Besides pharmacological interventions, life style modification is also important in diabetes management. The use of complementary and alternative medicine is expected to play a criti- cal role in effectively managing diabetes.
Complementary and alternative medicine (CAM) is defined as the medical practices, products, and health care systems that are not considered as parts of conventional care by the National Institutes of Health (NIH).
4)In spite of the advanced conventional medicine, the use of CAM in the United States has increased signif- tional therapy alone. 65 patients with diabetes were included in the study. 20 patients consumed 32- 48 g of kudzu root extract daily for at least 20 days (median 34 days) with conventional therapy, and 45 patients received conventional diabetic care alone. Fasting blood glucose level was obtained at baseline and after the administration of herbal medicine. Hemoglobin A1c, cholesterol profiles [LDL(Low-density lipoprotein), HDL(High-density lipoprotein, TG(Triglyceride)] and AST(Aspartate transaminase), ALT(Alanine transaminase) were measured.
Results : The difference between basal and index day fasting glucose level was 14.1 mg/dL (±24.65, p= 0.011) in the kudzu root group was statistically significant. Hemoglobin A1c data were obtained from 27 participants and there was a significant improvement in both, the kudzu root treatment group and the control group, with p values of 0.004 and 0.022, respectively. Cholesterol profiles and liver enzymes did not reveal significant changes.
Conclusion : The study findings suggested that kudzu root intake might help to lower serum fasting blood glucose levels in diabetic patients when combined with conventional therapy.
[Key words] Blood glucose, Puerarin, Kudzu root, Diabetic mellitus, Glucose lowering effect
icantly between 2002 and 2007
5)Naturopathic medicine, a part of CAM, is a unique whole system of medicine that focuses on patient wellness through the delivery of health-pro- motion counseling in clinical practice and has shown improvement in health care outcome in diabetes.; However, these improvements were not explained in detail by which herbal medi- cine contribute to the effectiveness because of limited availability of laboratory data.
6)-8)Radix Puerariae, also known as Gegen, Yegen or kudzu root, is the dried root of Pueraria lobata. Kudzu root is native to South East Asia and has been used to treat fever, diarrhea, diabetes and cardiovascular diseases over 2000 years.
9)-11)Puerarin, the most abundant is of flavonoid of kudzu, has shown blood glucose lowering effects in vitro and in vivo. Co-incu- bation of puerarinin high glucose-treated preadipocytes potentiated the glucose uptake considerably in a dose-dependent manner.
12)Also in an in vivo study, puerarin (15 mg/kg, i.v.) decreased blood glucose level and increased endorphin content in the absence of insulin stimulation in streptozotocin (STZ) induced diabetic rats.
11),13)The mechanism of action is known as the activation of peroxisome prolif- erator-activated receptor gamma (PPAR-γ ), the glucose transporter subtype 4 (GULT-4), and α 1-adrenogenic pathways elucidate the hypoglycaemic effect of puerarin.
13)-15)Kudzu root is also used for lowering choles- terol.
8)The publication by Zheng and colleagues proposed that administration of puerarin (400 mg/kg/day) has dropped the hepatic total cho- lesterol and triglyceride concentrations in liver of Wistar rats.
16)Diabetic patients have increased risk of cardiovascular disease and hyperlipidemia is risks factor either.
17)Yer-dahan-so-tang, Chungpye-sagan-tang,
and Galgeun-haegi-tang are examples of CAM remedies that originated from Sasang consti- tutional medicine theory of Lee Je-ma.
18)This theory is widely used to diagnose and treat diseases in Korea, and represents an individu- alized Korean traditional medical approach.
The CAM remedies mentioned above contains dried kudzu roots and prescribed to treat a dis- ease symptomized by thirst and polyuria which are similar to the symptoms of contemporary DM. Also, as shown above, kudzu root has been shown to be effective in lowering blood glucose level in previous studies.
11),12),19)Therefore, we hypothesized that kudzu root could be used for diabetes as an adjuvant therapy. The objective of this study was to investigate the effect of kudzu root on lowering blood glucose level in hospitalized diabetics in South Korea.
MATERIALS AND METHODS Settings
This was a retrospective chart review study of diabetic patients who were admitted to the naturopathy clinic and conventional clinic of the Stroke and Neurological Disorders Center of Kyung Hee University Hospital at gangdong, Korea, between June 1st 2006 and December 31th, 2011. Medication chart review was per- formed to collect demographic characteristics, past medical history, medications, and blood workup including fasting blood glucose, hemo- globin A1c, and cholesterol profile. CAM group includes patients who received CAM, contain- ing kudzu root as a principle ingredient, with conventional medicine (CM) and patients who CM only were assigned to control group.
Patients can choose the CAM therapy based on
patients’preference by themselves. The pri-
mary indication of the CAM or CM treatment was to prevent secondary stroke after ischemic attack. Patients in both groups received opti- mal treatment of other disease including dia- betes through the cooperative care with other department when necessary. The study was conducted after protocol approval by the Kyung Hee University Hospital at gangdong Institutional Review Board (KHNMC-OH-IRB 2012-046).
Subjects
The overall cohort included sixty-five patients with diabetes who were hospitalized at the naturopathy clinic and conventional clinic of the Stroke and Neurological Disorders Center in the Kyung Hee University Hospital at gangdong between June 1, 2006 and December 31, 2011. The patients in the center could select the medication therapy method either including Korean traditional medicine (CAM group) or only western medicine (CM group), when they admitted in. The patients usually are not medically urgent or severe.
Therefore, patients were categorized to two groups, control group and CAM group. Twenty patients were assigned to CAM group and con- sumed 32-48 g of kudzu root extract daily for at least 20 days (median 34 days). In control group, forty-five patients received conven- tional diabetic care only. Patients were eligible for inclusion in the study if they were 18 years of age or older; and if they had documented diagnosis by conventional physician of DM.
Inclusion criteria were: (1)currently diabetes mellitus (2)hospitalization for at least 20 days, (3)administration of selected CAM with Conventional Medicine (CM) or CM only during his/her hospitalization. Exclusion criteria
were: (1)patients on CM lowering or raising blood glucose except oral hypoglycemic agents or insulin(i.e. steroids, beta-blockers), (2) patients who need an operation or are in a critical condition.
Medical charts were identified through data warehouse software (Hyperion) which can be searched by Korean Standard Classification of Diseases 5th version code (KCD-5) till 2010 or KCD-6 (2011).
Quality control and process of CAM components
Kudzu root was prepared in three different ways, Yer-dahan-so-tang, Chungpye-sagan- tang, and galgeun-haegi-tang. Each prepara- tion has 7-8 ingredients including Pueraria Radix. For better quality control, all prescrip- tions were prepared by Kyung Hee Herb Pharm Co Ltdand under supervision of Korea Food &
Drug Administration in accordance with quali- ty assurance criteria of Korean pharma- copoeia. Herbal extracts were added to water to obtain final products of 360 ml solution and patient ingested 120 ml per dose three times a day. Table 1 represents components of each preparation.
Efficacy outcomes
Fasting blood glucose (FBG) was defined as
the first morning blood glucose of the day
without continuous tube feeding or parenteral
nutrition. Also we collected FBG level, choles-
terol profiles (LDL, HDL, TG) on index day,
defined as day 20 after CAM administration in
patients whose hospitalization is 20 days or
greater but less than 30 days or day 30 in
patients who were admitted hospital for at
least 30 day. The glycated hemoglobin A1c
(HbA1C) was monitored in patients who were admitted for at least 4 weeks.
Safety outcomes
Adverse effects of kudzu root were monitored with aspartate transaminase (AST) and alanine transaminase (ALT). Reference ranges for AST
and ALT are 0-40 IU/L. Drug-induced liver injury was defined as: (1)a rise of over two times the upper limit of reference range in ALT or (2)a combined rise in AST, provided above 2 times upper limit of reference range.
20)Statistical analyses
Dose (g) Raw material codea
Name of CM intervention Name of herb Table 1. Constituents of interventions per dose
Pueraria Radix Angelicae Temissimae Radix
Scutellariae Radix Angelicae Dahuricae Radix
Platycodi Radix Raphani Semen Cimilifugae Rhizoma
KHHP001 KHHP053 KHHP047 KHHP022 KHHP009 KHHP010 KHHP032
16 8 8 4 4 4 4 Yer-dahan-so-tang
Pueraria Radix Angelica Temissimae Radix
Scutellariae Radix Angelicae Dahiricae Radix
Rei Rhizoma Platycodi Radix Raphani Semen Cimilifugae Rhizoma
KHHP001 KHHP053 KHHP047 KHHP022 KHHP058 KHHP009 KHHP010 KHHP032
16 8 8 4 4 4 4 4 Chungpye-sagan-tang
Pueraria Radix Cimilifugae Rhizoma
Scutellariae Radix Armeniacae Semen Angelicae Dahiricae Radix
Platycodi Radix ZizyphiSpinosi Radix
KHHP001 KHHP032 KHHP047 KHHP194 KHHP022 KHHP009 KHHP030
12 8 6 6 4 4 4 Galgeun-haegi-tang
a Approved and regulated by Korea Food & Drug Administration
Differences between the treatment groups were evaluated by using the paired t-test for continuous variables. For categorical variables, Chi squared test and Fisher’s exact test were performed. All reported p values are two-
sided; a p value under 0.05 was considered to show statistical significance. SPSS software, version 20.0 (Chicago, USA), was used for sta- tistical analysis.
RESULTS
Table 2 represents demographics characteris- tics of the participants. There was no signifi- cant difference in age between two groups with a median of 66.5 years in CAM and with a median of 69.67 years in CM. 14 males (70%) were included in CAM and 25 males (44%) were included in CM. Majority of participants were diagnosed with type 2 diabetes. CAM cohort group has lower FBG than CM cohort at base- line. HbA1c was higher in CAM with a median of 8.39 but it was statistically not significant.
Either new medication or dose increase in anti-diabetic medication was initiated in 3 patients (15%) in CAM group and 10 patients (22.2%) in control group on observations and it was statistically insignificant (p= 0.594).
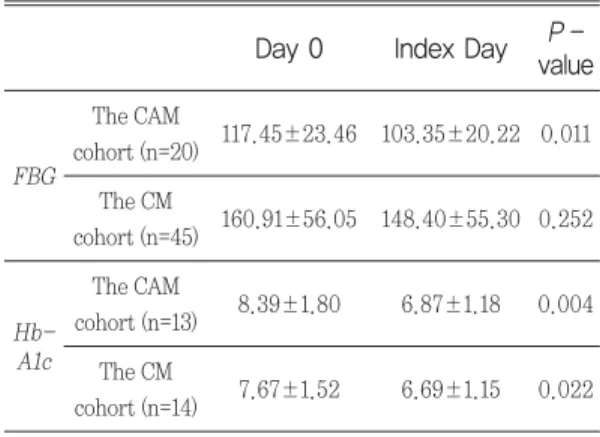
Fasting Blood Glucose (FBG)
As shown in the Table 3, FBG decreased from 117.45±23.46 to 103.35±20.22 in CAM group and it was statistically significant with P value of p= 0.011. On the other hand, the control group did not show a significant change in FBG (p= 0.252). Due to different preparations of kudzu root, 5 subjects consumed 32 g of kudzu root daily and 14 patients received 48 g of kutzu root daily. There was only one patient prescribed 36 g of kudzu root daily. Mean FBG drop (FBG index day - FBG baseline ) in 32 g of kudzu root group was 7 mg/dL and 48 g of kudzu root group showed a mean FBG drop with 25.5 mg/dL (Fig. 1). The patient consumed P -
value
�Feature The CAM
cohort (n=20)
The CM cohort (n=45)
Table 2. Baseline features of subjects in the selected CAM and the CM cohorts
Age (years)* 66.50±11.89 69.67±11.71 0.32 Sex
Males 14 (70%) 25 (56%)
Females 6 (30%) 20 (44%) 0.004 Type of DM
T2DM 19 (95%) 45 (100%)
IDDM 1 (5%) -
FBG(mg/dL) 117.45±23.46 160.91±56.05 0.001 HbA1c(%)* 8.39±1.80(n=13) 7.67±1.52(n=14) 0.686
* Plus-minus values are means ± standard deviation.
�Analysis by unpaired t test (with Welch’s correction when variances are unequal).
T2DM= Type 2 diabetes mellitus; IDDM= Insulin-Dependent Diabetes Mellitus; FBG= Fasting Blood Glucose; HbA1c = Hemoglobin A1c
P - value Day 0 Index Day Table 3. FBG and HbA1c changes in each cohort
The CAM
cohort (n=20) 117.45±23.46 103.35±20.22 0.011 The CM
cohort (n=45) 160.91±56.05 148.40±55.30 0.252 FBG
The CAM
cohort (n=13) 8.39±1.80 6.87±1.18 0.004 The CM
cohort (n=14) 7.67±1.52 6.69±1.15 0.022 Hb-
A1c
FBG= Fasting Blood Glucose; HbA1c = Hemoglobin A1c; CAM = Complementary and Alternative medicine; CM = Conventional Medicine
36 g of kudzu root dropped 6 mg/dL of FBG during the kudzu root intake.
HbA1c
HbA1c analysis only included patients whose baseline and index day HbA1c data were avail- able. Hemoglobin A1c analysis showed signifi- cant improvement in both kudzu root treat- ment group and control group with p value of 0.004 and 0.022 respectively.
Lipid Panels
There was no significant improvement in LDL, HDL and TG observed in the experimental group and the control group.
Safety outcomes
One patient in CAM group showed high ALT as 135 during the kudzu root intake with base- line 100, but no changes in AST with baseline 64. The others showed no significant changes
compared with their baseline in AST and ALT.
Discussions
This study confirms the previous in vivo and in vitro study, which showed the blood glucose lowering effects in kudzu root, and extends to clinical use in human subjects. The publication by Peng and colleagues proposed that supple- mentation of 0.2% of kudzu root in normal diet for two months has dropped fasting blood glu- cose and insulin levels in stroke prone sponta- neously hypertensive rats.
21)As shown in Fig. 1, the results from this analysis have shown dose dependent blood sugar lowering effects sup- porting kudzu root as the key factor for blood glucose lowering effect.
Recent study has proposed that administra- tion of puerarin (400 mg/kg/day) dropped the hepatic total cholesterol and triglyceride con- centrations in liver of Wistar rats.
16)Although this was an animal model based study, the result was obtained by administering the 4 times higher dose of medication than that of Song, et al (2004) which reported the hypo- glycemic effect when administering puerarin 100 mg/kg/day to Male SD rats.
22)Therefore, when taking herbal medications containing kudzu root as a major component, the hypo- glycemic effect was produced as anticipated from the literature, while the lipid lowering effect was not produced; however, the lipid lowering effect may be expected to be pro- nounced in case of long-term treatment with medication containing higher level of kudzu root.
Liver toxicity is known as a potential adverse effect of herbal medicines. The prevalence of concurrent medicine-induced liver injury was reported 0.5~1.4% prevalence of drug-induced Fig. 1 FBG variations depending on the amount
of Kudzu root intake a day
Drop in FBG = FBG index day - FBG day0