Factors influencing the six therapeutic communication modes among occupational therapists †
Eun-Jeong Ryu 1 · Sun Wook Lee 2
1 Dream Child Development Center, Daegu, Korea
2 Department of Occupational Therapy, Daegu University
Received 27 August 2020, revised 7 September 2020, accepted 7 September 2020
Abstract
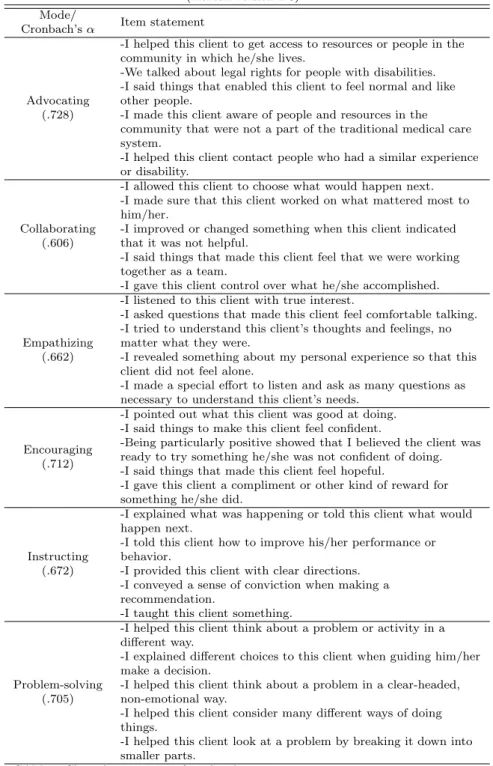
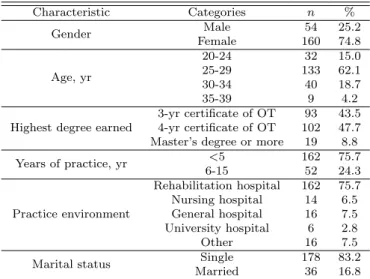
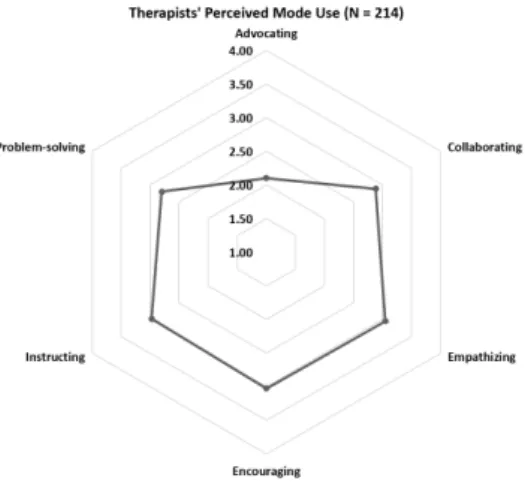
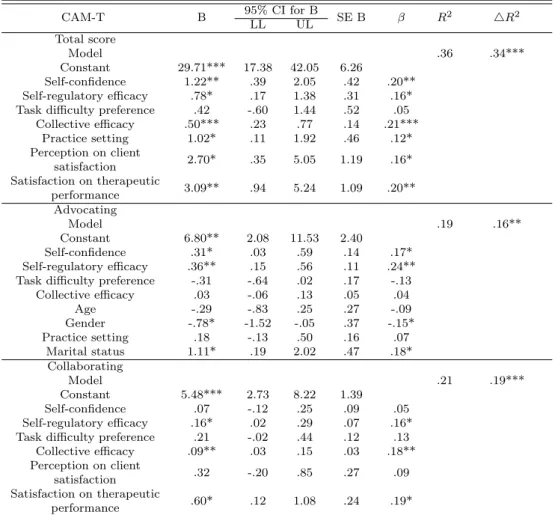
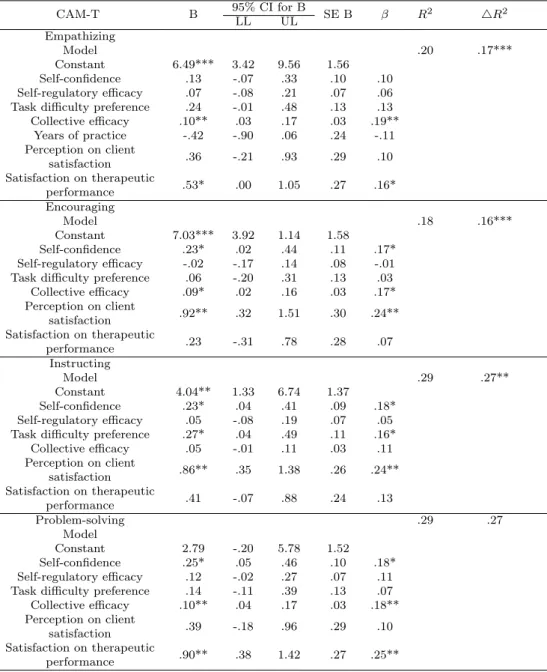
This cross-sectional study describes the perceived use of six therapeutic communi- cation modes among occupational therapists in Korea per the intentional relationship model and explores the factors influencing mode use. We conducted a paper-and-pencil survey with a convenience sampling method and analyzed a total of 214 responses (response rate: 64.88%) using the Vocational Self-Efficacy Scale and the Clinical As- sessment of Modes-Therapist ([CAM-T] Korean). Therapists reported that they used five of the six therapeutic communication modes with similar frequency and that they used the advocating mode least frequently. A multiple regression model comprising the three subscales of vocational self-efficacy-practice setting, therapists’ perception of client satisfaction, and satisfaction level on therapeutic performance-predicted the CAM-T total score of F (7, 205)=16.34, p<.0005, and adjusted R
2=.336. The strongest predictors across the six therapeutic modes were factors that pertained to perceptions of the therapeutic relationship. These findings suggest that efficacy-building efforts on individual confidence and collective efficacy, along with education for therapeutic relationships, are required to foster effective use of interpersonal skills.
Keywords: Intentional relationship model, occupational therapy, self-efficacy, therapeu- tic communication.
1. Introduction
Health care professionals such as occupational therapists face increasing responsibility due to recent legislation that requires them to take part in a concerted effort to increase mental health (Jung and Cha, 2009; Lee, 2020). The unique role of occupational therapists is to analyze the dynamics of life events and activities (i.e., occupation) and to facilitate factors that promote the optimal level of participation for multiple client populations, includ- ing a person with disabilities, an organization, and/or groups and populations (American
† This study was undertaken by Eun-Jeong Ryu in partial fulfillment of the requirements for the degree of Master’s in Rehabilitation Science at Daegu University.
1
Occupational Therapist, Dream Child Development Center, Daegu 41593, Korea
2