143 책임저자:최영현, 614-052, 부산시 부산진구 양정동 산 45번지
동의대학교 한의과대학 생화학교실 Tel: 051-850-7413, Fax: 051-853-4036 E-mail: [email protected]
접수일:2007년 8월 13일, 게재승인일:2007년 9월 10일
Correspondence to:Yung Hyun Choi
Department of Biochemistry, Dongeui University College of Oriental Medicine, San 45, Yangjeong-dong, Busanjin-gu, Busan 614-052, Korea Tel: +82-51-850-7413, Fax: +82-51-853-4036
E-mail: [email protected]
Gastric Cancer; Epidemiology and Causes
You Ho Myong and Yung Hyun Choi1
Korea Science Academy, Busan 614-822, 1Department of Biochemistry, Dongeui University College of Oriental Medicine and Department of Biomaterial Control (BK21 Program),
Dongeui University Graduate School, Busan 614-052, Korea
In this review, we conducted a deep analysis of the epidemiology of gastric carcinoma. As the conclusion of this study, we could find that there has been a steady decline in the incidence of gastric carcinogenesis in most societies. However, we could also conclude that there has existed a mild increase in the incidence of lower esophagus and cardia adenocarcinoma in White male societies. Although Helicobacter pylori infection is suggested to be the primary risk factor of gastric carcinogenesis in Asian countries, it accounts for less than half the cases in Western society. Still, the roles of dietary constituents, as salt and nitrites and the beneficial effects of a high fruit and vegetable diet are yet to be more specifically analyzed. (Cancer Prev Res 12, 143-153, 2007)
Key Words: Gastric cancer, Epidemiology, Diet, Helicobacter pylori
INTRODUCTION
Both the incidence and mortality of gastric cancer has de- clined drastically during the latter half of the 20th century.
Nevertheless, gastric cancer still remains the world’s second leading cause of cancer-related deaths, following lung cancer.1∼3) Recently gastric cancer has gotten much attention from investigators, particularly from epidemiologic ones with the official recognition of Helicobacter pylori as a causal factor for the disease. This has led to a deeper understanding of the pathogenesis and etiology of gastric carcinogenesis and there- fore, made it more possible to actively prevent the disease.
Different exposures to H. pylori and a variation of other environmental factors are thought to account for most of the variation observed in the incidence of gastric carcinoma between populations and over time. In this review, we will discuss the pathology of gastric cancer, consider descriptive epidemiology, and finally review the evidence of etiologic factors.
PATHOLOGY
Adenocarcinomas consist of roughly 90% of total stomach cancer cases. The remaining 10% is consisted of leiomyosar- comas and Non-Hodgkin’s lymphomas. There are some cases of adenosquamous, squamous, and undifferentiated carcinomas but these are quite rare. Choriocarcinomas, rhabdomyosar- comas, carcinoid tumors, and hemangiopericytomas can be counted as ‘very rare’ malignant tumors of the stomach. There also has been a report of Kaposi’s sarcoma, in association with the acquired immunodeficiency syndrome (AIDS).4) There are two histologic categories of adenocarcinomas: (1) an intestinal type or a well-differentiated type with cohesive neoplastic cells that form glandlike structures that usually ulcerate; and (2) a diffuse type, in which cell cohesion is absent, causing thickening and infiltration of the stomach wall without any discrete mass. In younger age groups, diffuse carcinomas are comparatively more common. Diffuse type carcinomas also have a more equal male-to-female ratio.5) The intestinal type
Table 1. Gastric cardia and noncardia cancer incidence rates (/100,000) in selected countries (age-standardized). Data taken from Cancer Incidence in Five Continents, Volume VII, 1996
Cardia Non-cardia
Country, region
Male Female Ratio Male Female Ratio
Singapore (Chinese) 2.4 0.6 4.0 27.0 13.0 2.1
Japan, Hiroshima 4.6 1.5 3.1 78.6 34.4 2.3
Japan, Osaka 2.4 0.8 3.0 62.6 26.5 2.4
China, Shanghai 8.1 2.0 4.1 38.5 19.0 2.0
US, SEERa (Black) 1.8 0.5 3.6 12.7 5.4 2.4
US, SEER (White) 2.9 0.5 5.8 4.6 2.5 1.8
United Kingdom 2.9 0.6 4.8 13.1 5.6 2.3
Australia, NSW 2.1 0.4 5.3 8.1 3.8 2.1
New Zealand (Non-Maori) 2.9 0.6 4.8 8.1 3.8 2.1
New Zealand (Maori) 1.5 0.5 3.0 26.4 13.3 2.0
aSurveillance, Epidemiology and End Results Program.
is more common in older age and male groups.
EPIDEMIOLOGY
By looking at the study of gastric cancer epidemiology, we can see notable distinctions between cancer of the gastric cardia and cancer localized to the rest of the stomach.
1. Time Trends
As previously stated, mortality and incidence rates for gastric cancer have decreased substantially over the second half of 20th century in many countries.1) In Japan, the mortality rate has declined to less than half over the same period. However the decline did not become distinct before the early 1970s. In Australia, the age-standardized mortality rate for gastric cancer in men has decreased consistently from 25.9/105 in 1950 to 6.7/105 in 1994.6) Nevertheless, in developed countries, a rapid increase in the incidence of gastric cardia cancer had been observed.7) An increasing incidence of gastric cardia adenocar- cinoma has also been described from the UK, Australia, Sweden and Switzerland.8∼11) Studies of the factor propose that there are supposed to be two primary factors. Barrett’s Esophagus, a complex of reflux esophagitis, has for decades been regarded as possessing unquantified malignant potential with a research conducted in Sweden which demonstrates a strong link between reflux symptoms and adenocarcinoma of the lower esophagus. Among those with frequent long-term and severe symptoms the OR was 43.5 (18.3∼103.5) for
adenocarcinoma of the esophagus and 4.4 (1.7∼11.0) for carcinoma of the cardia. However no link between esophageal squamous carcinoma and reflux was shown.12) A firm sugges- tion has been made that obesity is the fundamental cause in the reflux and esophageal troubles.13,14) Although it is not certain how this associates with gastric cardia cancer is not clear, two threads relative to dietary factors that may be relevant are suggested. A Swedish research demonstrated a firm negative correlation between dietary fiber intake and gastric cardia carcinoma (P trend<0.0001).15) This is probably because of the ability of cereal fiber to counterbalance salivary nitrite, which is discussed as a gastric carcinogen below.
2. Ethnicity, Age and Sex
Ethnicity plays a notable role in differences of gastric cancer incidence. Significant variations can be observed in the overall incidence of gastric cancer among distinct ethnic groups residing in the same region.16) Gastric cardia cancer prevalence differs between ethnic groups. Whites in the United States are suggested to be more susceptible over blacks, and non-Maoris over Maoris in New Zealand (Table 1).17) Gastric cancer incidence grows gradually as age increases. At presentation, most patients are between the ages of 50 and 70. Cases in patients below 30 are quite rare. Males are more susceptible to noncardia cancer than females by a ratio of roughly 2:1.
Gastric cardia cancer has a higher M:F ration. The ratio goes up to 6:1 in U.S. Whites (Table 1).17)
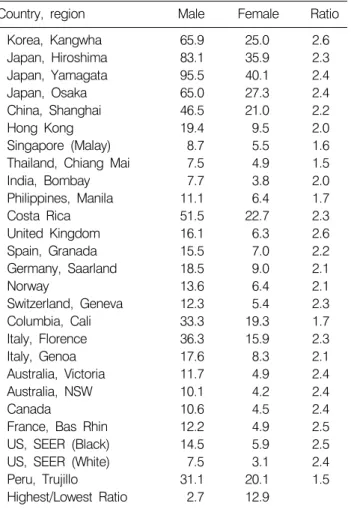
Table 2. International comparison of gastric cancer incidence rates (/100,000) in selected countries (age-standardized). Data taken from Cancer Incidence in Five Continents, Volume VII, 1996
Country, region Male Female Ratio
Korea, Kangwha 65.9 25.0 2.6
Japan, Hiroshima 83.1 35.9 2.3
Japan, Yamagata 95.5 40.1 2.4
Japan, Osaka 65.0 27.3 2.4
China, Shanghai 46.5 21.0 2.2
Hong Kong 19.4 9.5 2.0
Singapore (Malay) 8.7 5.5 1.6
Thailand, Chiang Mai 7.5 4.9 1.5
India, Bombay 7.7 3.8 2.0
Philippines, Manila 11.1 6.4 1.7
Costa Rica 51.5 22.7 2.3
United Kingdom 16.1 6.3 2.6
Spain, Granada 15.5 7.0 2.2
Germany, Saarland 18.5 9.0 2.1
Norway 13.6 6.4 2.1
Switzerland, Geneva 12.3 5.4 2.3
Columbia, Cali 33.3 19.3 1.7
Italy, Florence 36.3 15.9 2.3
Italy, Genoa 17.6 8.3 2.1
Australia, Victoria 11.7 4.9 2.4
Australia, NSW 10.1 4.2 2.4
Canada 10.6 4.5 2.4
France, Bas Rhin 12.2 4.9 2.5
US, SEER (Black) 14.5 5.9 2.5
US, SEER (White) 7.5 3.1 2.4
Peru, Trujillo 31.1 20.1 1.5
Highest/Lowest Ratio 2.7 12.9
Table 3. Migrant comparison of gastric cancer incidence rates (/100,000). Data taken from Cancer Incidence in Five Con- tinents, Volume VII, 1996
Ethnicity Region Male Female
Chinese China, Shanghai 46.5 21.0
Singapore 29.3 13.6
Hong Kong 19.4 9.5
Hawaii 12.3 5.2
Los Angeles 11.7 7.6
Highest/lowest ratio 4.0 2.8
Japanese Yamagata 95.5 40.1
Osaka 65.0 27.3
Hawaii 21.5 10.6
Los Angeles 21.2 12.0
Highest/lowest ratio 4.5 3.8 3. International Variations
The incidence of gastric cancer varies notably according to various geographic regions. In Table 2, International Agency for Research on Cancer data for 1996, age-standardized in- cidence rates in male subjects varying from 7.5/105 in Whites in the United States to 95.5/105 in Yamagata, Japan. Con- siderable parts of central and South America and China are included in high gastric cancer incidence regions.16) Most of the geographic variation can be explained by differences in the incidence of noncardia cancer. Cardia-localized cancer is distri- buted more uniformly (Table 1). Cardia-localized gastric cancer contribute for only 4 % of total gastric cancer in Osaka, Japan, whereas it accounts for 39% in white males in the United States.17) Histologically, diffuse adenocarcinoma incidence is suggested to be uniform in most societies. On the other hand,
the intestinal type predominates in the high-prevalence regions.
It also is the type that has decreased drastically in many societies studied.18,19) Migratory groups who came from high- to low-incidence countries tend to show an average risk of that of their homeland and of their new country (Table 3). In some cases, first generation migrants more or less maintained their high-risk while following generations showed approximating that of the host country.20)
4. Socioeconomic Status
One of quite noteworthy facts is that although low socioe- conomic status has been continuously proven to be related to an increased incidence of gastric carcinoma,1) the incline in risk of gastric cardia cancer has been predominant.8)
POSSIBLE CAUSES OF GASTRIC CANCER 1. H. pylori Infection
H. pylori was first officially reported by Marshall in 1983.
A pool of evidence concerning this organism and its role in the etiology of gastric cancer has been accumulated since it was classified.21) In 1994, the International Agency for Research on Cancer classified H. pylori as carcinogenic to humans.22) Evidence backing a causal correlation between gastric cancer and H. pylori can be found in case-control studies, ecologic studies, and prospective cohort studies. An international po- pulation study conducted by the Eurogast study group demonstrated that countries with high gastric cancer rates tend to have a high prevalence of H. pylori infection.23) H. pylori
infection rate has decreased in developed countries over recent decades, paralleling the decline in gastric cancer incidence.
Likewise, the surplus of gastric cancer seen in those of lower socioeconomic status is explained by a similar surplus of H.
pylori infection in these groups.24,25) Several case-control studies have demonstrated substantial correlations between overall gastric cancer risk and H. pylori positivity on serology,26∼28) others no correlation while two studies have reported notably increased incidence for noncardia gastric cancer,29,30) they did not observe any increase in gastric cardia cancer incidence.31,32) H. pylori infection may be lost with the development of atrophic gastritis and atrophy that are present in many gastric cancer patients. Therefore retrospective researches need to be interpreted with caution.33) Prospective researches supply the strongest support for the association.34∼36) Forman et al.37) attempted a pooled analysis of data from three such prospective researches. The risk of gastric cancer following H. pylori infection grew substantially with the length of follow-up observance, with an almost ninefold risk observed after 15 years or more. Meta-analyses of prospective studies propose that the incidence of gastric cancer is increased two- or threefold in subjects infected with H. pylori.38,39) A further prospective nested case-control study suggested a significant association between gastric adenocarcinoma and prior H. pylori infection, but the infection was not associated with gastric cardia cancer.40) The development and progression of chronic gastritis are ones of the mechanisms H. pylori uses to induce gastric cancer. The infection causes chronic gastritis in almost all infected subjects, and is the reason for nearly all cases of chronic gastritis.41,42) H. pylori-induced gastritis develop over time from an initially superficial nonatrophic stage to more sever stages, including severe atrophic gastritis with intestinal metaplasia in a small proportion of cases.43,44) In most cases of gastric cancer, chronic gastritis is found. Chronic gastritis is associated with an increased risk for gastric cancer.45) The risk increases with the severity of the gastritis, with reported risks in excess of tenfold for severe atrophic antral gastritis.45,46) Intestinal type gastric cancer is suggested to be more strongly related to severe atrophic gastritis, while the diffuse type is observed more often in nonatrophic gastritis.45) Strong evidence for a role for virulence factors in H. pylori carcinogenesis exists.
The CagA virulence factor is firmly associated with the risk of adenocarcinoma, while its absence carries, at most, a low risk of diffuse adenocarcinoma.47,48)
2. Gastric Non-Hodgkin's Lymphoma and H.
pylori
Most of non-Hodgkin’s lymphomas developing in the stomachs are B-cell tumors. These may be high-grade or low-grade lymphomas of mucosa-associated lymphoid tissue (MALT). These two subtypes may be components of the spectrum of the same disease.49,50) A correlation between gastric non-Hodgkin’s lymphoma and H. pylori infection has been demonstrated by numerous reports. Wotherspoon et al reported that H. pylori infection in 92% of 110 gastric MALT lymphoma,51) and Parsonnet et al.52) found that H. pylori infection before breakouts of the disease provided a sixfold increased incidence of gastric non-Hodgkin’s lymphoma over- all, with the correlation being more or less stronger for high- grade lymphomas. A regression of low-grade MALT lymphoma after eradication H. pylori was observed in five of six patients.53) A complete regression of low-grade MALT lymphoma for 16 months after H. pylori eradication with subsequent relapse of the lymphoma after reinfection with H. pylori has also been reported.54)
3. Peptic Ulcer Disease
H. pylori infection is a common risk factor among gastric ulcer, duodenal ulcer, and gastric cancer. An association between gastric cancer and prior peptic ulcer might be expected. Nonetheless, duodenal ulceration has been negatively associated with gastric cancer incidence.55∼57) Though previous researches could not show any increased long-term risk in patients with gastric ulcers, recent evidence supports a weak association with gastric cancer that develops other than in the cardia.55∼58) In searching for an explanation for this seeming paradox, Parsonnet has insisted that H. pylori infection can develop into gastric cancer or duodenal ulcer, but seldom to both.59) She suggested factors other than H. pylori infection must foster one disease while militating against the other, nominating genetic characteristics of the host and the organism, exogenous elements and, particularly, the time of life when H. pylori infection was acquired as important influences.
Early infection predisposes to atrophic gastritis and the incidence of carcinogenesis, however cuts down duodenal ulcer risk due to decreased acid production related to the gastritis.
Atrophic gastritis is less likely and gastric cancer incidence is reduced with later infection. It is yet uncertain whether the
risk of gastric carcinoma is modified by duodenal ulcer. The only firm data compare duodenal ulcer and gastric ulcer, both qualified by an accompanying gastritis. The primary issue is whether the adenocarcinoma rate following duodenal ulcer is distinct from that observed with a normal gastric mucosa; no data is usable nor likely on this subject. Nevertheless, the absence of gastritis means the absence of H. pylori, and there is decent data indicating that those without H. pylori colonization have a least risk of gastric cancer.60)
4. Radioactivity Exposure
Researches of survivors of the atomic bombings of Hiroshima and Nagasaki supply the best evidence concerning the role of ionizing radiation in the etiology of gastric cancer. Thompson et al.61) identified more than 2,600 cases of gastric cancer in a prospective incidence study of atomic bombing-victim cohort of approximately 80,000. A linear dose-response effect (p<
0.001) was observed between gastric cancer risk and radiation dose. Although the excess risk was small (0.32 at one Sievert, 95% CI, 0.16 to 0.50) and the creditable risk was low (6.5%), in the setting of a ghigh background rate of gastric cancer in this Japanese population. Patients going through therapeutic radiation to the region of the stomach for peptic ulcer (a treatment modality used from the late 1930s to the mid-1960s) and for testicular cancer,62∼64) also show notable confirmation for this association. Studies of these patients suggest a two- to fourfold increased risk in patients exposed to radiation doses of 15 to 30 Gy. Occupational radiation exposure in radiologists and radiographers is not likely to be a confirmation of the association.25,65,66) This presumably is due to the much lower radiation doses involved compared to the atomic bomb sur- vivors and the therapeutically irradiated. Distinction of risk based on the type of gastric carcinoma is not possible from the available evidence.
5. Gastric Surgery
A possible correlation between gastric surgery and following gastric cancer was first reported in 1922. Since then there have been various reports on the subject.67) Many studies, including prominent long-term follow-up studies, suggest an increased incidence of gastric cancer particularly 15 years or more after gastric surgery.57,68∼70) The correlation is strongest for gastrec- tomy performed for gastric ulcer. Vagotomy or Gasrectomy performed for duodenal ulcer do not suggest as much cor-
relation. The link does not extend to gastric cardia cancer.57) A potential association is with gastritis, a distinguished ante- cedent of cancer. Antrum gastritis related to H. pylori coloni- zation is an aspect of duodenal ulcer; gastric resection leaves a normal mucoasa, whereas gastritis of the body of the stomach and so of the gastric stump is an aspect of gastric ulcer; thus sparing of the cardia from active carcinoma would be predicted after partial gastrectectomy for duodenal ulcer.
6. Pernicious Anemia
A positive correlation between gastric cancer and pernicious anemia has long been suggested. Hsing et al. reported a threefold growth in the incidence of gastric carcinoma in a cohort of 4,517 pernicious anemia patients, traced for up to 20 years.71)
7. Epstein-Barr Virus Infection
Various investigators succeeded to isolate Epstein-Barr virus from poorly differentiated carcinomas with lymphoid infiltrate and gastric adenocarcinomas. Although the data is limited, Epstein-Barr virus infection is one of many possible risk factors of gastric carcinogenesis.
8. Dietary Factors
The etiologic importance of dietary variation can be noticed from the different variations in the mortality and incidence of gastric carcinoma over time, in varying socioeconomic groups, between and within countries and in migrants and their offspring. The role dietary factors take has been widely studied with inconclusive outcome.7,47,60)
9. Vegetables and Fruits
General people find it easy to believe that fresh fruits and vegetables have protective function against gastric cancer. This is indeed a dominant hypothesis. Various researches have demonstrated a protective correlation with fruits and vege- tables. However the result has been less convincing in limited cohort studies.72) Vitamins C (ascorbate) and E (α-tocopherol), selenium, carotenoids are ones of potential protective mole- cules.72) Vitamin C shows the strongest protective results with nearly halving of risk related to high intake vs. low intake shown in case-control studies.73) Nonetheless, a 5-year inter- vention trial which involved 30,000 subjects (age 40 to 69) in China failed to demonstrate any change in risk of gastric cancer
in subjects who received additional vitamin C.74) 10. Salt
In 1965, a hypothesis suggested that the continuous intake of high doses of salt may contribute in early atrophic gastritis.
As atrophic gastritis is, in many cases, believed to be related to gastric carcinogenesis, naturally it was postulated that excessive intake of salt would result in gastric cancer.75) Although not much quantitative data exists, excessive salt intake has been shown to be associated with an increased risk of gastric carcinogenesis.75∼83)
11. Nitrite and Nitrate
Thanks to animal experiments, many N-nitroso compounds have been proved to be carcinogenic. N-nitroso compounds are thought to be produced in the human stomach from dietary nitrate or nitrite. Therefore a hypothesis that nitrite- or nitrate-high cuisine might cause gastric carcinoma was suggested. Vegetables and preserved meats are the primary origin of nitrite and nitrate. Although potable water is a source of nitrate, the dose is negligible. Generally, daily nitrate consumption is roughly 100 folds that of nitrite. Small amounts of pre-formed N-nitroso compounds may as well found in some foods, including cured meats.73∼85) Although many case-control studies on dietary consumption of nitrate and the risk of gastric cancer consistently showed a negative correlation, it can be reasonably assumed that increased vegetable intake has been continuously related to a declined risk incidence of gastric cancer. Nitrate intake was an indicator of vegetable con- sumption and the negative association is not astounding.72) Several case-control researches have all reported a weak, statis- tically insignificant increased incidence of gastric cancer (relative risks from 1.12 to 1.28) for high versus low nitrite intake.81,84,86,87) Nitrite intake may reflect consumption of cured meats, generally high-salt foods, hence identifying an effect of nitrite consumption is not easy. Further evidence proposes that the interaction of the above dietary factors is crucial. For instance, a diet high in nitrite does not appear to result in an increased risk if that diet is also high in antioxidants from fruit and vegetables.84)
12. Other Dietary Factors
Published literature on gastric cancer and diet provides data for a broad array of food groups, food-storage methods,
nutrients and micronutrients. Obstacles in gathering and understanding this evidence limit the conclusions that can be drawn. The advent of widely available refrigeration, the con- sequent availability of fresh food and the decreased con- sumption of preserved foods may have accounted for the decline in gastric cancer incidence in the latter half of the 20th century. A research has suggested the way of virulent strains of H. pylori release reactive oxygen metabolites that could destroy neighboring glandular tissue leading to gastric glan- dular atrophy, hurried by factors as high-salt intake or bile reflux but slowed by antioxidants as alpha tocopherol, cysteine, β-carotene, and ascorbic acid.88)
13. Tobacco
While the relationship between gastric cancer and smoking has been extensively studied, the association remains uncertain.
Although most studies have reported a weak to moderate correlation, a few have found none.89∼94) In studies that re- ported a positive association concluded that generally less than twofold increase exists. Only a few researches have reported a dose-response relationship.91∼93) A particular limitation of the reports has been a deficiency of control for confounding factors, particularly by H. pylori infection, which is positively associated with smoking, and by fruit and vegetable intake, which is inversely correlated. Most of the evidence does not report any distinction of risk by histologic type or by anatomic subsite.
Although a case-control research reported a stronger correlation for gastric cardia cancer than for other gastric cancer across multiple categories of smoking, others did not.92,95,96)
14. Alcohol
Little supporting evidence was found by a review of the experimental, descriptive, and analytical evidence relating to alcohol and gastric cancer.97) The investigators examined over 50 cohort and case-control studies and concluded that alcohol consumption was not to be considered as a possible etiological risk factor of gastric carcinogenesis. Following studies have not challenged that statement.91,92) Numerous case-control resear- ches reported no correlation between gastric cardia cancer and alcohol consumption,92,96,98∼100) and one a doubling of risk in drinkers versus nondrinkers.101)
15. Asbestos
Although various researches on workers with occupational
exposure to asbestos have described limited evidence of an association between asbestos exposure and breakouts of the disease, methodological problems propose doubt on the association.102∼105) In a case-control research conducted in Western Australia, heavily exposed asbestos minders and millers did not show any correlation between gastric cancer mortality and level of exposure, duration of employment, or time since employment began.106)
16. Other Risk Factors
In first-degree relatives of gastric cancer patients, the incidence of gastric carcinoma is increased by roughly two- to threefold.107∼109) Genetic factor is not the sole cause of this phenomenon. Familial clustering of H. pylori infection is possible to contribute to this risk; other prospective risk factors include gastric polyps and blood type A groups. The conclud- ing decision on heredity in gastric carcinoma may be made by the Scandinavian Twin Study of 44,788 pairs of twins in the Finnish, Danish, and Swedish registries.110) The research found an increased incidence of gastric cancer in the twin of a patient.
Statistical analysis could conclude that inherited genes con- tributed 28% (95% C.I. 0∼51%), shared environmental fac- tors 10% (95% CI, 0∼34%), and environmental factors 62%
(95% CI, 0∼76%). The statistical model employed showed a perfect fitness (p<1.0). This result can be significant in the role of H. pylori infection. A review drafts our growing knowledge of the nearly boundless possibilities for a hereditary basis to resistance to pathogens, granting a role for H. pylori in both the shared environmental and hereditary causes of gastric cancer.111)
CONCLUSIONS
Although many profound advances have been made over the last few decades, much about the causes of gastric cancer still is not quite clear to us. Particularly baffling is the rise in adenocarcinoma around the cardia. One clue to solve this mystery is that this phenomenon is mostly confined to White males in affluent societies. Contrary to a developing view that H. pylori is a primary factor of gastric carcinogenesis, epide- miologic analysis presents that it may be one of the minor causes in Western societies. If chronic H. pylori infection increases the risk of cancer by a factor of about 2.5 in a population with a prevalence in older persons of about 50%,38)
then the Population Attributable Risk or Etiologic Fraction is only about 40%.112) Given the increasing reflux symptoms on eradication of H. pylori and the positive association between longstanding reflux symptoms and obesity with lower eso- phageal adenocarcinoma, this may be the ultimate irony.12,14,113) As our civilized society becomes more hygienic and affluent, it cuts its risk of gastric cancer down. Nevertheless, at least in males, it increases the prevalence of adenocarcinoma around the cardia at the same time.
REFERENCES
1) Howson CP, Hiyama T, Wynder EL. The decline in gastric cancer: epidemiology of an unplanned triumph. Epidemiol Rev 8, 1-27, 1986.
2) Parkin DM, Pisani P, Ferlay J. Estimates of the worldwide incidence of eighteen major cancers in 1985. Int J Cancer 54, 594-606, 1993.
3) Pisani P, Parkin DM, Ferlay J. Estimates of worldwide mortality from eighteen major cancers in 1985. Implications for prevention, and projections of future burden. Int J Cancer 54, 891-903, 1993.
4) Jass JR. Tumours of the stomach. In: eds, McGee JO’D, Isaacson PG, Wright NA. Oxford Textbook of Pathology, Oxford, Oxford University Press, pp 1165-1173, 1992.
5) Lauren P. The two histological main types of gastric car- cinoma: diffuse and so-called intestinal-type carcinoma: an attempt at a histoloclinical classification. Acta Pathol Microbiol Scand 64, 31-49, 1965.
6) International Agency for Research on Cancer Unit of De- scriptive Epidemiology. 2001. WHO cancer mortality data- bank. Cancer Mondial. www-dep.iarc.fr/dataava/globocan/
who.htm.
7) Blot WJ, Devesa SS, Kineller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 265, 1287-1289, 1991.
8) Powell J, McConkey CC. The rising trend in oesophageal adenocarcinoma and gastric cardia. Eur J Cancer Prev 1, 265-269, 1992.
9) Lord RV, Law MG, Ward RL, Giles GG, Thomas RJ, Thursfield V. Rising Incidence of oesophageal adenocarcinoma in men in Australia. J Gastroenterol Hepatol 13, 356-362, 1998.
10) Hansson LE, Sparén P, Nyrén O. Increasing incidence of both major histological types of esophageal carcinomas among men in Sweden. Int J Cancer 54, 402-407, 1993.
11) Levi F, La Vecchia C. Adenocarcinoma of the esophagus in Switzerland [letter]. JAMA 265, 2960, 1991.
12) Lagergren J, Bergström R, Lindgren A, Nyrén O. Sympto- matic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 340, 825-831, 1999.
13) Chow WH, Blot WJ, Vaughan TL, Risch HA, Gammon MD,
Stanford JL, Dubrow R, Schoenberg JB, Mayne ST, Farrow DC, Ahsan H, West AB, Rotterdam H, Niwa S, Fraumeni JF Jr. Body mass index and risk of adenocarcinomas of the esophagus and gastric cardia. J Natl Cancer Inst 90, 150-155, 1998.
14) Lagergren J, Bergstrom R, Nyren O. Association between body mass and adenocarcinoma of the oesophagus and gastric cardia. Ann Intern Med 130, 883-890, 1999.
15) Terry P, Lagergren J, Ye W, Wolk A, Nyren O. Inverse association between intake of cereal fiber and risk of gastric cardia cancer. Gastroenterology 120, 387-391, 2001.
16) Parkin DM, Whelan SL, Ferlay J. Cancer incidence in five continents, vol VII. Lyon, International Agency for Research on Cancer, pp 822-823, 1997.
17) Parkin DM, Whelan SL, Ferlay J. Cancer incidence in five continents, Vol VII. Lyon, International Agency for Research on Cancer, pp 922-924, 1997.
18) Munoz N, Correa P, Cuello C, Duque E. Histological types of gastric carcinoma in high and low risk areas. Int J Cancer 3, 809-818, 1968.
19) Sipponen P, Järvi O, Kekki M, Siurala M. Decreased inci- dences of intestinal and diffuse types of gastric carcinoma in Finland during a 20-year period. Scand J Gastroenterol 22, 865-871, 1987.
20) Haenszel W, Kurihara M. Studies of Japanese migrants. I.
Mortality from cancer and other diseases among Japanese in the United States. J Natl Cancer Inst 40, 43-68, 1968.
21) Marshall BJ. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1, 1273-1277, 1983.
22) International Agency for Research on Cancer. Schistosomes, liver flukes and Helicobacter pylori. IARC monographs on the evaluation of carcinogenic risks to humans. Vol. 61. Lyon, International Agency for Research on Cancer, 1994.
23) The Eurogast Study Group. An international association between Helicobacter pylori infection and gastric cancer. Lancet 341, 1359-1362, 1993.
24) Banatvala N, Mayo K, Megraud F, Jennings R, Deeks JJ, Feldman RA. The cohort effect and Helicobacter pylori. J Infect Dis 168, 219-221, 1993.
25) Wang JX, Inskip PD, Boice JD Jr, Li BX, Zhang JY, Fraumeni JF Jr. Cancer Incidence among medical diagnostic X-ray workers in China, 1950 to 1985. Int J Cancer 45, 889-895, 1990.
26) Asaka M, Kimura T, Kato M, Kudo M, Miki K, Ogoshi K, Kato T, Tatsuta M, Graham DY. Possible role of Helicobacter pylori infection in early gastric cancer development. Cancer 73, 2691-2694, 1994.
27) Kikuchi S, Wada O, Nakajima T, Nishi T, Kobayashi O, Konishi T, Inaba Y. Serum anti-Helicobacter pylori antibody and gastric carcinoma among young adults. Cancer 75, 2789-2793, 1995.
28) Sipponen P, Kosunen TU, Valle J, Riihela M, Seppala K.
Helicobacter pylori infection and chronic gastritis in gastric
cancer. J Clin Pathol 45, 319-323, 1992.
29) Kuipers EJ, Gracia-Casanova M, Peña AS, Pals G, Van Kamp G, Kok A, Kurz-Pohlmann E, Pels NF, Meuwissen SG.
Helicobacter pylori serology in patients with gastric carcinoma.
Scand J Gastroenterol 28, 433-437, 1993.
30) Lin JT, Wang JT, Wang TH, Wu MS, Lee TK, Chen CJ.
Helicobacter pylori infection in a randomly selected population, healthy volunteers, and patients with gastric ulcer and gastric adenocarcinoma. A seroprevalence study in Taiwan. Scand J Gastroentol 28, 1067-1072, 1993.
31) Hansson LE, Engstrand L, Nyren O, Evans DJ Jr, Lindgren A, Bergstrom R, Andersson B, Athlin L, Bendtsen O, Tracz P. Helicobacter pylori infection: independent risk indicator of gastric adenocarcinoma. Gastroenterology 105, 1098-1103, 1993.
32) Talley NJ, Zinsmeister AR, Weaver A, DiMagno EP, Car- penter HA, Perez-Perez GI, Blaser MJ. Gastric adeno- carcinoma and Helicobacter pylori infection. J Natl Cancer Inst 83, 1734-1739, 1991.
33) Webb PM, Forman D. Helicobacter pylori as a risk factor for cancer. Baillieres Clin Gastroenterol 9, 563-582, 1995.
34) Forman D, Newell DG, Fullerton F, Yarnell JW, Stacey AR, Wald N, Sitas F. Association between infection with Helico- bacter pylori and risk of gastric cancer; evidence of a prospective investigation. BMJ 302, 1302-1305, 1991.
35) Nomura A, Stemmermann GN, Chyou PH, Kato I, Perez- Perez GI, Blaser MJ. Helicobacter pylori infection and gastric carcinoma among Japanese Americans in Hawaii. N Engl J Med 325, 1132-1136, 1991.
36) Parsonnet J, Friedman GD, Vandersteen DP, Chang Y, Vo- gelman JH, Orentreich N, Sibley RK. Helicobacter pylori infection and the risk of gastric cancer. N Engl J Med 325, 1127-1131, 1991.
37) Forman D, Webb P, Parsonnet J. Helicobacter pylori and gastric cancer. Lancet 343, 243-244, 1994.
38) Danesh J. Helicobacter pylori and gastric cancer; systematic review of epidemiological studies. Aliment Pharmacol Ther 13, 851-856, 1999.
39) Eslick GD, Lim LL, Byles JE, Xia HH, Talley NJ. Association of Helicobacter pylori infection with gastric carcinoma: a meta-analysis. Am J Gastroenterol 94, 2373-2379, 1999.
40) Simán JH, Forsgren A, Berglund G, Florén CH. Association between Helicobacter pylori and gastric carcinoma in the city of Malmo, Sweden. A prospective study. Scand J Gastroenterol 32, 1215-1221, 1997.
41) Kuipers EJ, Uyterlinde AM, Pena AS, Roosendaal R, Pals G, Nelis GF, Festen HP, Meuwissen SG. Long-term sequelae of Helicobacter pylori gastritis. Lancet 345, 1525-1528, 1995.
42) Valle J, Kekki M, Sipponen P, Ihamäki T, Siurala M. Long- term course and consequences of Helicobacter pylori gastritis.
Results of a 32 year follow up study. Scand J Gastroenterol 31, 546-550, 1996.
43) Sipponen P. Atrophic gastritis as a premalignant condition.
Ann Med 21, 287-290, 1989.
44) Siurala M, Sipponen P, Kekki M. Chronic gastritis: dynamic and clinical aspects. Scand J Gastroenterol 109(Suppl), S69-76, 1985.
45) Sipponen P, Riihelä M, Hyvärinen H, Seppälä K. Chronic nonatrophic (“superficial”) gastritis increases the risk of gastric carcinoma. A case-control study. Scand J Gastroenterol 29, 336-340, 1994.
46) Sipponen P, Kekki M, Haapakoski J, Ihamaki T, Siurala M.
Gastric cancer risk in chronic atrophic gastritis: statistical calculations of cross-sectional data. Int J Cancer 35, 173-177, 1985.
47) Parsonnet J, Friedman GD, Orentreich N, Vogelman H. Risk of gastric cancer in people with CagA positive or CagA negative Helicobacter pylori infection. Lancet 40, 297-301, 1997.
48) Ponzetto A, Soldati T, De Giuli M. Helicobacter pylori screening and gastric cancer (letter). Lancet 348, 758, 1996.
49) Isaacson PG. Gastric lymphoma and Helicobacter pylori. N Engl J Med 330, 1310-1311, 1994.
50) Isaacson PG. Recent developments in our understanding of gastric lymphomas. Am J Surg Pathol 20, S1-7, 1996.
51) Wotherspoon AC, Ortiz-Hidalgo C, Falzon MR, Isaacson PG.
Helicobacter pylori-associated gastritis and primary B-cell gastric lymphoma. Lancet 338, 1175-1176, 1991.
52) Parsonnet J, Hansen S, Rodriguez L, Gelb AB, Warnke RA, Jellum E, Orentreich N, Vogelman JH, Friedman GD.
Helicobacter pylori infection and gastric lymphoma. N Engl J Med 330, 1267-1271, 1994.
53) Bayerdorffer E, Neubauer A, Rudolph B, Thiede C, Lehn N, Eidt S, Stolte M. Regression of primary gastric lymphoma of mucosa-associated lymphoid tissue type after cure of Helicobacter pylori infection. MALT Lymphoma Study Group.
Lancet 345, 1591-1594, 1995.
54) Cammarota G, Montalto M, Tursi A, Vecchio FM, Fedeli G, Gasbarrini G. Helicobacter pylori reinfection and rapid relapse of low-grade B-cell gastric lymphoma. Lancet 345, 192, 1995.
55) Hansson LE, Nyren O, Hsing AW, Bergstrom R, Josefsson S, Chow WH, Fraumeni JF Jr, Adami HO. The risk of stomach cancer in patients with gastric or duodenal ulcer disease. N Engl J Med 335, 242-249, 1996.
56) Lee S, Iida M, Yao T, Shindo S, Nose Y, Akazawa K, Okabe H, Fujishima M. Risk of gastric cancer in patients with non- surgically treated peptic ulcer. Scand J Gastroenterol 25, 1223-1226, 1990.
57) Molloy RM, Sonnenberg A. Relation between gastric cancer and previous peptic ulcer disease. Gut 40, 247-252, 1997.
58) Hole DJ, Quigley EM, Gillis CR, Watkinson G. Peptic ulcer and cancer: an examination of the relationship between chronic peptic ulcer and gastric carcinoma. Scand J Gastroenterol 22, 17-23, 1987.
59) Parsonnet J. Helicobacter pylori in the stomach-a paradox unmasked. N Engl J Med 335, 278-280, 1996.
60) Uemura N, Okamoto S, Yamamoto S, Matsumura N, Yamaguchi S, Yamakido M, Taniyama K, Sasaki N,
Schlemper RJ. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med 345, 784-789, 2001.
61) Thompson DE, Mabuchi K, Ron E, Soda M, Tokunaga M, Ochikubo S, Sugimoto S, Ikeda T, Terasaki M, Izumi S, et al. Cancer incidence in atomic bomb survivors. Part II: solid tumors, 1958-1987. Radiat Res 137, S17-67, 1994.
62) Griem ML, Kleinerman RA, Boice JD Jr, Stovall M, Shefner D, Lubin JH. Cancer following radiotherapy for peptic ulcer.
J Natl Cancer Inst 86, 842-849, 1994.
63) Moller H, Mellemgaard A, Jacobsen GK, Pedersen D, Storm HH. Incidence of second primary cancer following testicular cancer. Eur J Cancer 29A, 672-676, 1993.
64) van Leeuwen FE, Stiggelbout AM, van den Belt-Dusebout AW, Noyon R, Eliel MR, van Kerkhoff EH, Delemarre JF, Somers R. Second cancer risk following testicular cancer: a follow-up study of 1,909 patient. J Clin Oncol 11, 415-424, 1993.
65) Matanoski GM, Seltser R, Sartwell PE, Diamond EL, Elliott EA. The current mortality rates of radiologists and other physician specialists: specific causes of death. Am J Epidemiol 101, 199-210, 1975.
66) Smith PG, Doll R. Mortality from cancer and all causes among British radiologist. Br J Radiol 54, 187-194, 1981.
67) Stalnikowicz R, Benbassat J. Risk of gastric cancer after gastric surgery for benign disorders. Arch Intern Med 150, 2022-2026, 1990.
68) Fisher SG, Davis F, Nelson R, Weber L, Goldberg J, Haenszel W. A cohort study of stomach cancer risk in men after gastric surgery for benign disease. J Natl Cancer Inst 85, 1303-1310, 1993.
69) Tersmette AC, Giardiello FM, Tytgat GN, Offerhaus GJ.
Carcinogenesis after remote peptic ulcer surgery: the long- term prognosis of partial gastrectomy. Scand J Gastroenterol 212(Suppl), 596-569, 1995.
70) Tersmette AC, Offerhaus GJ, Tersmette KW, Giardiello FM, Moore GW, Tytgat GN, Vandenbroucke JP. Meta-analysis of the risk of gastric stump cancer: detection of high risk patient subsets for stomach cancer after remote partial gastrectomy for benign condition. Cancer Res 50, 6486-6489, 1990.
71) Hsing AW, Hansson LE, McLaughlin JK, Nyren O, Blot WJ, Ekbom A, Fraumeni JF Jr. Pernicious anaemia and subsequent cancer: a population based cohort study. Cancer 71, 745-750, 1993.
72) Kono S, Hirohata T. Nutition and stomach cancer. Cancer Causes Control 7, 41-55, 1996.
73) Neugut AI, Hayek M, Howe G. Epidemiology of gastric cancer. Semin Oncol 23, 281-291, 1996.
74) Blot WJ, Li JY, Taylor PR, Guo W, Dawsey S, Wang GQ, Yang CS, Zheng SF, Gail M, Li GY, Yu Y, Liu B, Tangrea J, Sun Y, Liu F, Fraumeni JF Jr, Zhang YH, Li B. Nutrition intervention trials in Linxian, China: supplementation with specific vitamin/mineral combinations, cancer incidence, and disease-specific mortality in the general population. J Natl
Cancer Inst 85, 1483-1491, 1993.
75) Joossens JV, Hill MJ, Elliott P, Stamler R, Lesaffre E, Dyer A, Nichols R, Kesteloot H. Dietary salt, nitrate and stomach cancer mortality in 24 countries. Int J Epidemiol 24, 494-504, 1996.
76) Boeing H, Jedrychowski W, Wahrendorf J, Popiela T, Tobiasz-Adamczyk B, Kulig A. Dietary risk factors in in- testinal and diffuse types of stomach cancer: a multicentre case-control study in Poland. Cancer Causes Control 2, 227-233.
1991.
77) Knekt P, Jarvinen R, Dich J, Hakulinen T. Risk of colorectal and other gastro-intestinal cancers after exposure to nitrate, nitrite and N-nitroso compounds: a follow-up study. Int J Cancer 80, 852-856, 1999.
78) Buiatti E, Barchielli A, Bartolacci S, Bucchi L, De LV, Federico M, Ferretti S, Paci E, Vettorazzi M, Zanetti R.
Stage-specific incidence of breast cancer before the beginning of organized screening programs in Italy. Cancer Causes Control 13, 65-71, 2002.
79) Graham S, Haughey B, Marshall J, Brasure J, Zielezny M, Freudenheim J, West D, Nolan J, Wilkinson G. Diet in the epidemiology of gastric cancer. Nutr Cancer 13, 19-34, 1990.
80) Hansson LE, Nyrén O, Bergström R, Wolk A, Lindgren A, Baron J, Adami HO. Diet and risk of gastric cancer. A population-based case-control study in Sweden. Int J Cancer 55, 181-189, 1993.
81) Kim HJ, Kim MK, Chang WK, Choi HS, Choi BY, Lee SS.
Effect of Nutrient Intake and Helicobacter pylori Infection on Gastric Cancer in Korea: A Case-Control Study. Nutr Cancer 52,138-146, 2005.
82) Lee JK, Park BJ, Yoo KY, Ahn YO. Dietary factors and stomach cancer: a case-control study in Korea. Int J Epidemiol 24, 33-41, 1995.
83) Ramon JM, Serra L, Cerdo C, Oromi J. Dietary factors and gastric cancer risk. A case-control study in Spain. Cancer 71, 1731-1735, 1993.
84) Buiatti E, Palli D, Decarli A, Amadori D, Avellini C, Bianchi S, Bonaguri C, Cipriani F, Cocco P, Giacosa A. A case-control study of gastric cancer and diet in Italy: II. Association with nutrients. Int J Cancer 45, 896-901, 1990.
85) Gonzalez CA, Riboli E, Badosa J, Batiste E, Cardona T, Pita S, Sanz JM, Torrent M, Agudo A. Nutritional factors and gastric cancer in Spain. Am J Epidemiol 139, 466-473, 1994.
86) Hansson LE, Nyren O, Bergstrom R, Wolk A, Lindgren A, Baron J, Adami HO. Nutrients and gastric cancer risk. A population-based case-control study in Sweden. Int J Cancer 57, 638-644, 1994.
87) La Vecchia C, Ferraroni M, D'Avanzo B, Decarli A, Franceschi S. Selected micronutrient intake and the risk of gastric cancer.
Cancer Epidemiol Biomarkers Prev 3, 393-398, 1993.
88) Dixon ME. Commentary: role of Helicobacter pylori on gastric mucosal damage, gastric cancer and gastric MALT lymphona.
Gastroenterology 113, 565-566, 1997.
89) Doll R, Peto R, Wheatley K, Gray R, Sutherland I. Mortality in relation to smoking: 40 years’ observations on male British doctors. BMJ 309, 901-911, 1994.
90) Engeland A, Andersen A, Haldorsen T, Tretli S. Smoking habits and risk of cancers other than lung cancer: 28 years’
follow-up of 26,000 Norwegian men and women. Cancer Causes Control 7, 497-506, 1996.
91) Hansson LE, Baron J, Nyrén O, Bergström R, Wolk A, Adami HO. Tobacco, alcohol and the risk of gastric cancer.
A population-based case-control study in Sweden. Int J Cancer 57, 26-31, 1994.
92) Ji BT, Chow WH, Yang G, McLaughlin JK, Gao RN, Zheng W, Shu XO, Jin F, Fraumeni JF Jr, Gao YT. The influence of cigarette smoking, alcohol, and green tea consumption of the risk of carcinoma of the cardia and distal stomach in Shanghai, China. Cancer 77, 2449-2457, 1996.
93) McLaughlin JK, Hrubec Z, Blot WJ, Fraumeni JF Jr.
Smoking and cancer mortality among US Veterans: a 26 year follow-up. Int J Cancer 60, 190-193, 1995.
94) Vaughan TL, Davis S, Kristal A, Thomas DB. Obesity, alcohol, and tobacco as risk factors for cancers of the eso- phagus and gastric cardia: adenocarcinoma versus squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev 4, 85-92, 1995.
95) Gammon MD, Schoenberg JB, Ahsan H, Risch HA, Vaughan TL, Chow WH, Rotterdam H, West AB, Dubrow R, Stanford JL, Mayne ST, Farrow DC, Niwa S, Blot WJ, Fraumeni JF Jr. Tobacco, alcohol, and socioeconomic status and adenocarcinomas of the esophagus and gastric cardia. J Natl Cancer Inst 89, 1277-1284, 1997.
96) Unakami M, Hara M, Fukuchi S, Akiyama H. Cancer of the gastric cardia and the habit of smoking. Acta Pathol Jpn 39, 420-424, 1989.
97) Franceschi S, La Vecchia C. Alcohol and the risk of cancers of the stomach and colon-rectum. Dig Dis 12, 276-289, 1994.
98) Gray JR, Coldman AJ, MacDonald WC. Cigarette and alcohol use in patients with adenocarcinoma of the gastric cardia or lower esophagus. Cancer 69, 2227-2231, 1992.
99) Guo W, Blot WJ, Li JY, Taylor PR, Liu BQ, Wang W, Wu YP, Zheng W, Dawsey SM, Li B, Fraumeni JF Jr. A nested case-control study of oesophageal and stomach cancers in the Linzian nutrition intervention trial. Int J Epidemiol 23, 444-450, 1994.
100) Palli D, Bianchi S, Decarli A, Cipriani F, Avellini C, Cocco P, Falcini F, Puntoni R, Russo A, Vindigni C. A case-control study of cancers of the gastric cardia in Italy. Br J Cancer 65, 263-266, 1992.
101) Kabat GC, Ng SK, Wynder EL. Tobacco, alcohol intake, and diet in relation to adenocarcinoma of the esophagus and gastric cardia. Cancer Causes Control 4, 123-132, 1993.
102) Andersen A, Glattre E, Johansen BV. Incidence of cancer among lighthouse keepers exposed to asbestos in drinking
water. Am J Epidemiol 138, 682-687, 1993.
103) Cocco P, Palli D, Buiatti E, Cipriani F, DeCarli A, Manca P, Ward MH, Blot WJ, Fraumeni JF Jr. Occupational exposures as risk factors for gastric cancer in Italy. Cancer Causes Control 5, 241-248, 1994.
104) Frumkin H, Berlin J. Asbestos exposure and gastrointestinal malignancy-review and meta-analysis. Am J Indust Med 14, 79-95, 1988.
105) Zandjani F, Hogsaet B, Andersen A, Langard S. Incidence of cancer among nitrate fertilizer workers. Int Arch Occup Environ Health 66, 189-193, 1994.
106) de Klerk NH, Armstrong BK, Musk AW, Hobbs MS.
Cancer mortality in relation to measures of occupational exposure to crocidolite at Wittenoom Gorge in Western Australia. Br J Indust Med 46, 529-536, 1989.
107) La Vecchia C, Negri E, Franceschi S, Gentile A. Family history and the risk of stomach and colorectal cancer. Cancer 70, 50-55, 1992.
108) Lissowska J, Groves FD, Sobin LH, Fraumeni JF Jr, Nasierowska-Guttmejer A, Radziszewski J, Regula J, Hsing
AW, Zatonski W, Blot WJ, Chow WH. Family history and risk of stomach cancer in Warsaw, Poland. Eur J Cancer Prev 8, 223-227, 1999.
109) Palli D, Galli M, Caporaso NE, Cipriani F, Decarli A, Saieva C, Fraumeni JF Jr, Buiatti E. Family history and risk of stomach cancer in Italy. Cancer Epidemiol Biomarkers Prev 3, 15-18, 1994.
110) Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M, Pukkala E, Skytthe A, Hemminki K.
Environmental and heritable factors in the causation of cancer. Analysis of cohorts of twins from Sweden, Denmark and Finland. N Engl J Med 343, 78-85, 2000.
111) Kwiatkowski D. Susceptibility to infection. BMJ 321, 1061-1065, 2000.
112) Schlesseman JJ. Case-control studies. Design, conduct, analy- sis. New York, Oxford University Press, 1982.
113) Labenz J, Blum AL, Bayerdorffer E, Meining A, Stolte M, Borsch G. Curing Helicobacter pylori infection in patients with duodenal ulcer may provoke reflux osophagitis. Gastro- enterology 112, 1442-1447, 1997.