www.krspine.org
Thoracic Chordoma in an Atypical Location Mimicking an Esophageal Adenocarcinoma
- A Case Report -
Sam Supreeth MBBS, MS, Chang-Hee Cho, M.D.*, Sang-Il Kim, M.D.*, Young-Hoon Kim, M.D., Ph.D.*
J Korean Soc Spine Surg 2020 September;27(3):109-114.
Originally published online September 30, 2020;
https://doi.org/10.4184/jkss.2020.27.3.109
Korean Society of Spine Surgery
SMG-SNU Boramae Medical Center, 20, Boramae-ro 5-gil, Dongjak-gu, Seoul 07061, Korea Tel: +82-2-831-3413 Fax: +82-2-831-3414
©Copyright 2017 Korean Society of Spine Surgery pISSN 2093-4378 eISSN 2093-4386
The online version of this article, along with updated information and services, is located on the World Wide Web at:
http://www.krspine.org/DOIx.php?id=10.4184/jkss.2020.27.3.109
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://
creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Korean Society of
Spine Surgery
Thoracic Chordoma in an Atypical Location Mimicking an Esophageal Adenocarcinoma - A Case Report -
Sam Supreeth MBBS, MS, Chang-Hee Cho, M.D.*, Sang-Il Kim, M.D.*, Young-Hoon Kim, M.D., Ph.D.* Department of Orthopedic Surgery, Khoula Hospital, Oman
*Department of Orthopaedic Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea Study Design: Case report.
Objectives: To report a case of chordoma mimicking adenocarcinoma in a 52-year-old woman.
Summary of Literature Review: Chordoma, a rare malignant tumor of primitive notochordal origin, accounts for 1-4% of all bone malignancies. Chordoma mimicking esophageal adenocarcinoma in the posterior mediastinum is unique.
Materials and Methods: A 52-year-old asymptomatic woman was referred to our center with an incidentally detected posterior mediastinal mass and no significant medical history. The mass was diagnosed on a routine medical screening by esophagogastroduodenoscopy and the patient was receiving yearly follow-up. An increase in size was noticed during the second year of follow-up on endoscopic ultrasonography and the patient was referred to the Department of Gastrointestinal Surgery of our hospital. This paper was written after receiving institutional review board (IRB) approval (KC20ZASI0214).
Results: En bloc resection was performed for the growing thoracic mass and pathologic findings confirmed it to be chordoma. A follow- up computed tomography examination was conducted at 8 months, as well as magnetic resonance imaging at 1 year, and there was no local recurrence.
Conclusions: Posterior mediastinal chordoma at the thoracic level is very rare. Furthermore, it is difficult to diagnose because its immunohistochemical characteristics mimic those of esophageal adenocarcinoma, meaning that it can be missed. Management is a challenge due to its anatomical location and additional local invasion. Therefore, a multidisciplinary approach is needed, including careful consultation with the patient to provide the optimal treatment for the best possible outcome.
Key words: Chordoma, Mediastinum, Esophageal adenocarcinoma
Received: March 19, 2020 Revised: April 1, 2020 Accepted: September 4, 2020 Published Online: September 30, 2020
Corresponding author: Young-Hoon Kim, M.D., Ph.D.
ORCID ID: Sam Supreeth: https//orcid.org/0000-0003-0962-703X Chang-Hee Cho: https//orcid.org/0000-0002-6850-7284 Sang-Il Kim: https//orcid.org/0000-0002-2758-0012 Young Hoon Kim: https//orcid.org/0000-0003-1237-4600 Department of Orthopaedic Surgery, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea 222 Banpodae-ro, Seocho-Gu, Seoul, 06591 Korea
TEL: +82-2-2258-6118, FAX: +82-2-535-9834 E-mail: [email protected]
Chordoma a rare malignant tumor of primitive notochordal origin accounts for 1-4% of all the bone malignancies.1,2) Surveillance, Epidemiology, and End Results(SEER) database report an incidence of 0.08/100,000 population with predominance in men by 2.7/1–1.6/1 in the age group of 50- 70 year.3,4,5) Chordomas mainly involve the axial skeleton with skull base (32%), sacrum (29.2%) and mobile spine (32.8%) of which thoracic chordoma form 2-5%.3-5)
We report a unique case of thoracic chordoma in a female mimicking poorly differentiated adenocarcinoma of esophagus.
Case Report
A 52-year-old asymptomatic lady, referred to our center
with an incidentally detected posterior mediastinal mass
Sam Supreeth Mbbs et al Volume 27 • Number 3 • September 30 2020
www.krspine.org 110
with no history of significance. Diagnosed on a routine medical screening by esophagogastroduodenoscopy and was on yearly follow up. An increase in size noticed during the second year of follow-up on endoscopic ultrasonography and was referred to Department of Gastrocolic surgery of our hospital.
Ultrasound showed 11.3 mm lesion of maximum
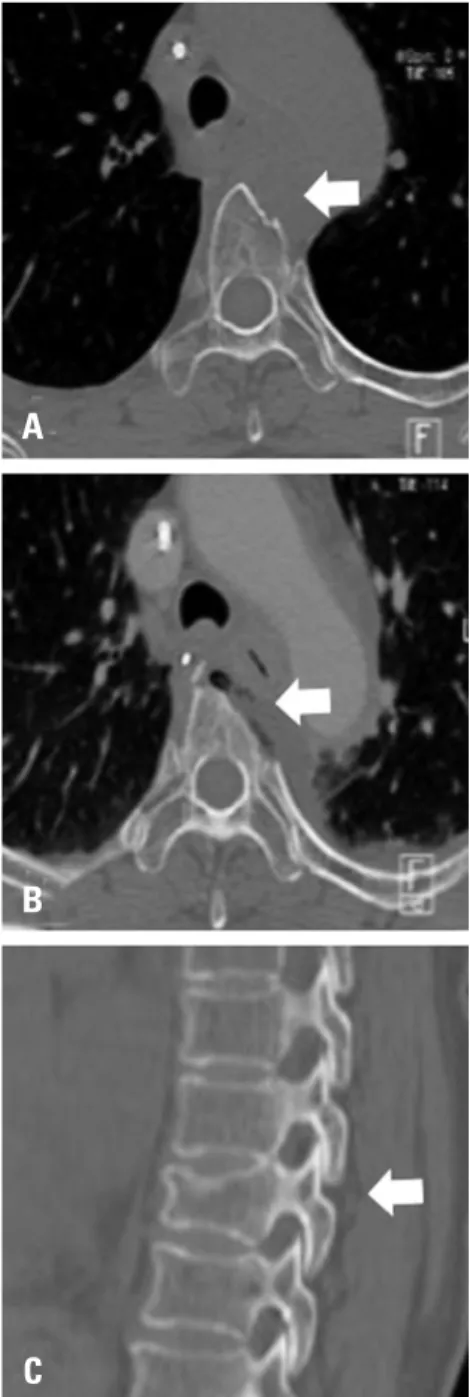
extension, and the clinical diagnosis was Submucosal tumor. CT images showed 30X19mm sized ovoid, well- defined posterior mediastinum mass at T4-5 with bony erosion of the adjacent dorsal spine. MRI reconfirmed CT findings with intermediate signal intensities on both T1 and T2 weighted images. The mass was abutting the trachea and aortic arch without definite invasion and was indistinguishable from the esophagus (Fig. 1). The differentials were Bronchogenic, Neurogenic, Submucosal tumor in order of probability.
Endoscopic biopsy of esophagus showed epithelioid tumor cells and mucin. Immunohistochemistry was positive for CK-7(Cytokeratin), P-63, Pan-cytokeratin, and faintly positive for CEA(Carcinoma embryonic antigen). Findings suggested of a poorly differentiated adenocarcinoma.
Medical Oncology unit started adjuvant concurrent chemoradiation therapy (CCRT), and the patient received a total of 46Gy radiation with Paclitaxel and Carboplatin.
Follow-up PET-CT showed an increased standardized uptake value (SUV) at the lesion from 3.7 to 4.3 and also a hyper-metabolic mass at T4 (Fig. 2) based on which surgical management decided. Patient underwent VATS- assisted thoracotomy for mass excision and vertebral body en-bloc resection with a wide margin by the unit of Cardiothoracic and Spine unit of Orthopedics (Fig. 3).
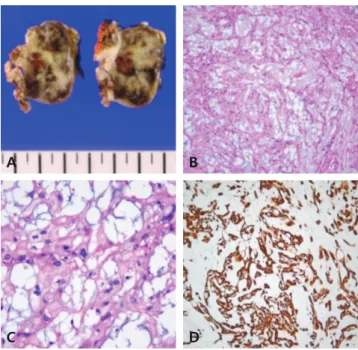
Surgical specimen showed an ill-defined soft and gelatinous tumor (Fig. 4A). Microscopically, epithelioid tumor cells arranged in cords or nets, and background was myxoid (Fig. 4B). Tumor cells had intracytoplasmic vacuoles with bubbly appearance, the so-called physaliferous cell (Fig. 4C). Immunostaining was positive for pan-cytokeratin and epithelial membrane antigen (Fig. 4D). Therefore, the tumor was diagnosed as Chordoma. Given the changed diagnosis, after multi-department and patient consultation, it was agreed the management done was optimum and needed regular follow-up.
8 month CT (Fig. 5A, B) and 1 year MRI (Fig. 5C, D) follow up examination was done and there was no local recurrence.
Discussion
The incidence of Chordoma spinal tumor at thoracic is Fig. 1. Magnetic resonance imaging and computed tomography (CT) im-
ages of the thoracic spine revealing a circumscribed posterior mediastinal mass. (A) Axial T1-weighted image demonstrating that the mass had intermediate signal intensity. (B) Sagittal image demonstrating that the mass was indistinguishable from the esophagus. (C) Axial CT demon- strating bony erosion of the T4 body.
A
B
C
rare and much rarer in the female. Few cases of Chordoma at the thoracic level reported in the literature(Table 1).2,5)
Radiological diagnosis based on the location was gastric mucosal tumor, schwannoma, neurofibroma, ganglioneuroma, chondrosarcoma.2) Our patient also had a slow and delayed growth in the lesion which is seen in conditions aforementioned.2,4). Chordoma is similarly a slow-growing, low-grade neoplasm which is locally aggressive, invasive, and radioresistant.4)
On exhaustive search of the literature, there are mention of epithelial neoplasms, metastatic adenocarcinoma known to mimic Chordoma, histologically making diagnosis difficult.6,7) One case has been reported of the unlikely possibility of collision tumor of Chondroid chordoma and
nasal adenocarcinoma in sino-nasal space by Gallet et al.8) Histologically chordoma is classified into Classic, chondroid and undifferentiated. The classic chondroma is typical of the extensively abundant vacuolated cytoplasm known as Physaliferous cell.The cytokeratin staining has sensitivity and specificity of 98%,100% for chordoma differentiating from chordosarcoma.4) In retrospect when Fig. 2. Positron emission tomography/computed tomography showing
increased standardized uptake values in (A) a coronal image and (B) an axial image of the mass after concurrent chemoradiation therapy.
Fig. 3. Computed tomography findings. (A) A pre-operative axial image.
(B) An axial image showing postoperative en bloc resection with a wide margin. (C) Sagittal scout image at the T4 level.
A
B
C A
B
Sam Supreeth Mbbs et al Volume 27 • Number 3 • September 30 2020
www.krspine.org 112
the histopathological slides of FNA reanalyzed traces of Chordoma features were present but missed due to small biopsy sample.
The tumor was radio-resistant to CCRT and noticed to be locally aggressive on PET-CT even after a high dose of radiation of 48 Gy.4) The lesion was excised en-bloc which is the treatment of choice for Chordoma.2,4). Posterior mediastinal Chordoma at the thoracic level is very rare.
Owing to its immune-histological mimicking is tricky to diagnose and can be missed. Management is a challenge due to its anatomic location and added local invasion for which a multidisciplinary approach is needed, taking the patient into confidence to provide the optimum treatment for the best possible outcome.
REFERENCES
1. Healey JH, Lane JM. Chordoma: a critical review of di- agnosis and treatment. Orthop Clin North Am. 1989 Jul;20(3):417-26.
2. Wang TJ, Shu SH, Lin CW, et al. Thoracic chordoma:
An unusual presentation of the spinal tumor. Am J Med Sci. 2008 Mar;335(3):239-41. DOI: 10.1097/
MAJ.0b013e3180ebeac3.
3. McMaster ML, Goldstein AM, Bromley CM, et al. Chor- doma: incidence and survival patterns in the United States, Cancer Causes Control. 2001 Jan;12(1):1-11. DOI:
10.1023/a:1008947301735.
4. Walcott BP, Nahed B V., Mohyeldin A, et al. Chordoma:
Current concepts, management, and future directions. Lan- cet Oncol. 2012 Feb;13(2):e69-76. DOI: 10.1016/S1470- Fig. 4. Operative findings. (A) Gross photo of sagittal cut surfaces of ex-
tra-osseous chordoma involving the anterior T4 vertebral bone. The tumor was soft, gelatinous, tan-gray, and hemorrhagic. (B) The tumor showed epithelioid tumor cells arranged in cohesive cords and nests. The stroma was basophilic and myxoid (×100). (C) The tumor cells had an abundant eosinophilic cytoplasm and intracytoplasmic vacuoles (arrow) with a bubbly appearance (×400). (D) The tumor cells were diffusely positive for pancytokeratin (×100).
Fig. 5. Computed tomography. (A) An 8-month follow-up axial image.
(B) A sagittal image showing no local recurrence. Magnetic resonance imaging demonstrating (C) a 1 year follow-up axial image. (D) A sagittal image showing no local recurrence.
Table 1. Previous case reports
Author Year Age Sex Complaints Location
Walsh et al. 1992 69 F Back pain, numbness T10-12 Holden et al. 1998 20 M Numbness, ataxia T4-5 Hester et al. 1999 53 M Dysphagia, dyspnea C6-T1 Wang et al. 2008 25 F Left hand anhydrosis T1-5 Matsubayashi et al. 2012 47 F Asymptomatic T horacic-
Extraosseous Royo et al. 2013 52 M Upper back pain T5-7
2045(11)70337-0.
5. Royo Crespo I, Rivas de Andrés JJ, Embún Flor R, et al.
Chondroid Chordoma in an Atypical Location. Arch Bronconeumol. 2013 Nov;49(11):491-3. DOI: 10.1016/
j.arbres.2013.03.006.
6. Bjornsson J, Wold LE, Laws EX, et al. Chordo- ma of the mobile spine. A clinicopathologic analy- sis of 40 patients. Cancer. 1993 Feb 1;71(3):735-40.
DOI: 10.1002/1097-0142(19930201)71:3<735::aid- cncr2820710314>3.0.co;2-8.
7. Coffin CM, Swanson PE, Wick MR, et al. An immuno- histochemical comparison of chordoma with renal cell carcinoma, colorectal adenocarcinoma, and myxopapillary ependymoma: a potential diagnostic dilemma in the di- minutive biopsy. Mod Pathol. 1993 Sep;6(5):531-8.
8. Gallet P, Marcon N, Georgel T, et al. Chondroid Chordo- ma and Nasal Adenocarcinoma: An Exceptional Associa- tion. Case Rep Oncol Med. 2012;2012:861217. Epub 2012 Sep 17. DOI: 10.1155/2012/861217.
114
J Korean Soc Spine Surg. 2020 Sep;27(3):109-114
Case Report
© Copyright 2020 Korean Society of Spine Surgery
Journal of Korean Society of Spine Surgery. www.krspine.org. pISSN 2093-4378 eISSN 2093-4386
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
식도 선암종 감별을 요하는 비전형적인 위치에 발생된 흉부 척색종 - 증례 보고 -
Sam Supreeth MBBS • 조창희* • 김상일* • 김영훈*
Department of Orthopedic Surgery, Khoula Hospital, Oman
*가톨릭대학교 서울성모병원 정형외과학교실 연구 계획: 증례 보고
목적: 52세 여성 환자에서 흉추에 발생한 식도 선암종 감별을 요하는 척색종을 보고하고자 한다.
선행 연구문헌의 요약: 원시 척삭 기원의 희귀 악성 종양인 척색종은 모든 골 악성 종양의 1-4%를 차지한다. 특히 후종격동에서 식도 선암종과 감별을 요하는 척색종은 매우 특이한 사례이다.
대상 및 방법: 특이 병력 없는 52세 무증상 여성으로 후방 종격동 종괴가 우연히 발견되어 본원으로 내원하였다. 건강 검진 상 식도 위장관 내시경 검사에 서 발견되어 매년 정기적으로 경과 관찰을 시행하였다. 경과 관찰 2년차에 크기 증가로 본원으로 의뢰되었다. 본 논문은 본원 IRB 승인(KC20ZASI0214) 을 받은 이후 진행되었다.
결과: 증가된 종괴에 대해 절제술이 시행되었고, 병리학 소견상 척색종으로 확인되었다. 수술 후 8개월차 CT 및 1년차 MRI 상 국소 재발은 없었다.
결론: 흉부 후종격동 척색종은 매우 드물다. 특히 면역 조직학적으로 식도 선암종을 흉내 내기 때문에 진단하기 까다롭고 진단을 놓치기 쉽다. 해부학적 위치와 국소 침습적인 특성으로 인해 최적의 치료를 하기 위해서는 다학제적인 접근 방식이 필요하다.
색인 단어: 척색종, 종격동, 식도 선암종 약칭 제목: 비정형 위치 발생한 흉부 척색종
접수일: 2020년 3월 19일 수정일: 2020년 4월 1일 게재확정일: 2020년 9월 4일 교신저자: 김영훈
서울시 서초구 반포대로 222 가톨릭대학교 의과대학 서울성모병원 정형외과학교실
TEL: 02-2258-6118 FAX: 02-535-9834 E-mail: [email protected]