INTRODUCTION
In Korea, the recorded incidence of breast cancer has ra- pidly increasing since the introduction of screening prog- ram. In particular, the proportion of early breast cancer and lymph node negative breast cancer has risen. The Korean Breast Cancer Society report that from 2003 to 2004, the proportion of stage 0 and I breast cancer rose from 30.5%
to 57.3% and the proportion of node-negative breast cancer was 65.1%.(1)
While prognostic factors for breast cancer include tumor size, age, hormone responsiveness, the most important pro- gnostic factor is still axillary lymph node metastasis. An
accurate diagnosis of lymph node metastasis is critical, and decreasing axillary morbidity is very important issue in sur- gical oncology. Side effects of conventional axillary dissec- tion can range from mild to severe and can be a chronic con- dition that affects patients’quality of life for years after cancer surgery.(2) Recently, a less invasive procedure, sen- tinel lymph node biopsy (SLNB), has been developed to stage the axilla for invasive breast cancer. The evaluation of mor- bidity after axillary lymph node dissection (ALND) and SLNB is under investigation in ongoing randomized trials as the NSABP B-32 and the ALMANAC trial.(3) There are many comparisive report between conventional ALND and SLNB for postoperative axillary morbidity. They were almost study about long-term postoperative axillary morbidity after SL- NB. Factors affecting axillary morbidity include postope- rative radiation therapy, adjuvant chemotherapy, and phy- sical therapy. However, few studies have examined axillary Purpose: Sentinel lymph node biopsy (SLNB) is a relatively
accurate diagnostic method for determining the presence of axillary lymph node metastasis (ALND). SLNB reduces the need for axillary lymph node dissection, thereby decreasing the postoperative axillary morbidity. The present study com- pared the postoperative axillary morbidity rates during early postoperative days for patients undergoing either SLNB or conventional ALND.
Methods: We conducted a prospective case-control study of breast cancer patients. The degree of axillary morbidity was compared between 28 SLNB patients (Group I) and 38 ALND patients (Group II).
Results: The SLNB group showed decreased arm swelling and restriction of their shoulder motion in comparison with the conventional axillary dissection group (p<0.05). SLNB
and additional lymph node sampling did not result in any additional morbidity.
Conclusion: SLNB or lymph node sampling was associated with less axillary morbidity like arm edema, limitation of mo- tion than was conventional ALND. The rate of postopera- tive axillary morbidity did not differ following lymph node sam- pling and SLNB. SLNB may be an effective method for dia- gnosing of axillary lymph node metastasis with decreasing the postoperative axillary morbidity. (J Breast Cancer 2007;10:
107-13)
Key Words : Sentinel lymph node biopsy (SLNB), Conventional axillary dissec- tion, Axillary morbidity, Early postoperative period
중심단어 : 감시림프절 생검술, 액와부림프절 곽청술, 액와부합병증, 수술후 초기 상태
Comparison of Early Postoperative Axillary Morbidity Following the Sentinel Lymph Node Biopsy or Axillary Lymph Node Dissection
Jung Sun Lee, Soo Jung Hong, Hee Jeong Kim, Mi Ae Chang, In Young Sung
1, Kyang Yup Gong
2, Euy Nyong Kim
3, Sei Hyun Ahn, Byung Ho Son
Departments of Surgery, 1Rehablitalogy, 2Pathology and 3Nulcear Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Breast Cancer
O R I G N A L A R T I C L E
책임저자 : 손병호
138-736 서울시 송파구 풍납동 388-1, 서울아산병원 외과 Tel: 02-3010-3927, Fax: 02-474-9027
E-mail : [email protected]
접수일 : 2007년 3월 29일 게재승인일 : 2007년 5월 15일
107
morbidity in the early postoperative period. The present study compared SLNB and conventional axillary dissection in term of their effects on axillary morbidity in the early postoperative period.
METHODS
1. Patient population
Patients were prospectively collected between July and August 2005 at the Asan Medical Center. We enrolled 39 SLNB patients and 27 conventional ALND patients. The indication of SLNB was clinically lymph node negative breast cancer. Exclusion criteria were previous sugery for breast cancer, bilateral breast surgery, or preoperative chemo- therapy.
2. Surgical procedure
The sentinel lymph node method involved use of a radio- colloid (99m Tc-Antimony trisulfide). On the day of surgery, 0.1 cc radiocolloid (99m Tc-Antimony trisulfide) was injected onto the periareolar area after which lymphoscintigraphy was performed to evaluate the presence of the sentinel lym- ph node in axillary and internal mammary area. During breast cancer surgery, the sentinel lymph node was detected using a handheld gammma-detection probe (Neo2000�, Model 2100, Neoprobe production. Dublin, USA) and excised.
In addition, any grossly suspicious lymph node were excised.
The excised sentinel lymph node and suspicious lymph node were evaluated using intraoperative frozen-section analy- sis. If there was an evidence of metastatic lymph node, a conventional ALND was performed. Patients with palpable metastatic lymph nodes underwent conventional ALND.
3. Axillary morbidity assessment scale
No patients had preexcisting problems in the arm, such as edema, decreased range of motion, or pain. Postoperati- vely, patients were not given any restrictions in their every- day behavior, and were allowed to commence arm exercise as soon as possible. Follow-up examinations were under- taken on postoperative day 5. For measurement of arm swell- ing, the circumference (in cm) of both arm (upper and lower arm) was measured 10 cm above and 10 cm below the lateral
epicondyle of olcecranon, the mean of 3 measurements was recorded.(4) Arm measurement data were analyzed as follow in order to preclude the influence of the dominant arm cir- cumference, and to ensure evaluation only of arm change due to surgery.(5) The upper arm difference=the postoperative circumference of the ipsilateral upper arm minus the posto- perative circumference of contralateral upper arm. The lower arm difference=the postoperative circumference of the ip- silateral lower arm minus the postoperative circumference of the contralateral lower arm. The existence of arm swell- ing was regarded as an upper and lower arm circumference difference of 2 cm or more. For the subjective assessement of arm edema, patients were asked to determine arm swelling on the operated arm compared with the non-operated arm as either none (none, no arm swelling, tightness, or heaviness) or severe (constant arm heaviness, disability, decreased func- tional activity, huge arm swelling). Numbness was assessed comparing the sensitivities of inner and outer skin area of the upper arm, axilla and chest wall of the operated shoulder with the non-operated shoulder. Numbness was recorded as either none, mild or moderate. A subjective assessment of numbness was undertaken using a Visual Analog Scale (VAS) ranging from 0 (no numbness) to 10 (severe). All pati- ents underwent goniometric measurement of the affected arm by a physiotherapist at each time point. Measurement of the following arm movements was undertaken on posto- perative day 5: shoulder flection (0-180°), shoulder extension (0-60°), shoulder abduction (0-180°).(6) Motion restriction was noted using a scale from 0 to 3 (0, no motion restriction;
1, minor restriction; 2, moderate restriction; 3, severe restric- tion). Pain, paresthesia, and stiffness in the operated arm were evaluated using a visual analog scale ranging from 0 to 10. Arm power was measured with method standardized by American society of hand therapist. In sitting position, shoulder abduction, and elbow flexion, they grip the dyna- mometer in each hand.
For 28 patients (Group I), the sentinel lymph node showed no metastatic disease according to examination of intrao- perative frozen section (6-8 sections) or in paraffin sections stained with hematoxylin and eosin staining and anticyto- keratin. In those cases, no further axillary dissection was undertaken other than sampling. these patients were com-
pared prospectively with 38 patients who underwent sur- gery for breast cancer during the same period and who un- derwent complete axillary dissection (Group II). The 8 pa- tients who underwent only SLNB and 20 patients who un- derwent both SLNB and non-sentinel lymph node sampl- ing, were compared with the above variable. Study design is shown in Fig 1.
4. Statistical analysis
SPSS software for Windows was used for statistical an- alyses. Frequency distributions were evaluated using Mann- Whitney U-test and Chi-square test. The level of significance was set p<0.05. Normally distributed quantitative variables were analyzed using t-test for independent samples with correction for heteroscedasticity.
RESULTS
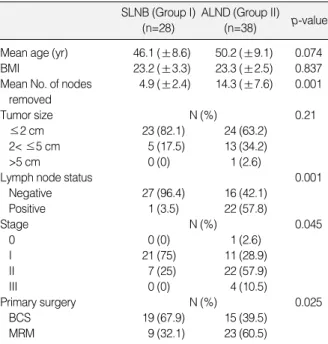
Mean age was 46.1 yr in SLNB (Group I), and 50.2 yr in ALND (Group II) (p=0.074). Group I were likely to have sma- ller primary tumor than Group II (82.1% vs 63.2% with tumor size <2.0 cm). Group I had more early-stage cancer having stage 0 or I patients than Group II (75% vs 31.5%, p=0.045).
Both groups also differed in primary surgery, and Group I were underwent more frequntly breast conserving opera- tion (67.9% vs 39.5%) than Group II. The mean number of sentinel lymph nod dissected was 2.5 (±1.0) lymph nodes in the Group I. In term of the axillary dissection level, 10 pa- tients (15.2%) underwent SLNB only, 20 (30.3%) patients
underwent SLNB and sampling, 3 (4.5%) patients under- went sampling only, 4 (6.1%) patients underwent Level I di- ssection, and 29 patients (43.9%) underwent Level I and II axillary dissection. Mean number of removed axillary lymph node was 4.9 (±2.4) in Group I and 14.3 (±7.6) in Group II.
Charateristics of the study population were shown in Table 1.
1. Postoperative axillary morbidity 1) Subjective side effect
Any Group I patients had not symptom of Arm edema, but 4 (10.5%) patient in Group II were more than 3 cm ede- ma. The incidence of joint pain (more than moderate) was 2 (7.1%) patients in Group II, and 6 patients (15.8%) in Group I. But there was no significant difference of limitation in range of arm motion (p=0.0195). Numbness was reported in 57.9% of the patient after ALND in contrast to 46.5% in the SLNB. There was no significant difference in both Group (Table 2 ).
By visual analogue scale, there was no difference in arm edema, tingling or numbness, and axillary pain between Group I and II (Table 3). But Group II were slightly more than Group I in limitation of range of motion and arm ede-
Sentinel lymph node biopsy (SLNB)
Metastasis (-) Metastasis (+)
Group I Group II
ALND (N=38) SNB only
(N=20)
SNB+Sampling (N=20) Fig 1.Study design.
Table 1.Patient and tumor characteristics
SLNB (Group I) (n=28)
ALND (Group II) (n=38) p-value Mean age (yr) 46.1 (±8.6) 50.2 (±9.1) 0.074
BMI 23.2 (±3.3) 23.3 (±2.5) 0.837
Mean No. of nodes 4.9 (±2.4) 14.3 (±7.6) 0.001 removed
Tumor size N (%) 0.21
≤2 cm 23 (82.1) 24 (63.2)
2< ≤5 cm 5 (17.5) 13 (34.2)
>5 cm 0 (0) 1 (2.6)
Lymph node status 0.001
Negative 27 (96.4) 16 (42.1)
Positive 1 (3.5) 22 (57.8)
Stage N (%) 0.045
0 0 (0) 1 (2.6)
I 21 (75) 11 (28.9)
II 7 (25) 22 (57.9)
III 0 (0) 4 (10.5)
Primary surgery N (%) 0.025
BCS 19 (67.9) 15 (39.5)
MRM 9 (32.1) 23 (60.5)
SLNB=sentinel lymph node biopsy; ALND=axillary lymph node dis- section; BMI=body mass index; BCS=breast conserving surgery;
MRM=modified radical mastectomy Clinically &
Ultrasonographically LN metastasis (-)
ma (arm edema: 1.21±0.62 vs 1.0±0.0, p=0.079; Limita- tion of motion: 1.89±0.65 vs 1.61±0.63, p=0.076).
2) Objective side effect
When the difference between both upper arm circumfe- rence was more than 2 cm, we regarded it as the existence of difference. The significant difference in upper arm cir- cumference was 1 (3.6%) patients in Group I and 6 (15.8%) patients in Group II (p=0.09), and the significant difference in lower arm circumference was 0 patient (0%) in Group I (13.8%) patients in Group II (p=0.046) (Table 4).
Comparising with the degree of extension and elevation motion in two groups, when there are difference in both shoulder, we defined the restriction. There was little signi- ficant difference in abduction, 11 (39.3%) patients in Group I, 18 (47.4%) patients in Group II (p=0.51), but there was sig-
nificant difference of flection motion 12 (42.9%) patients in Group I, 27 (71.1%) patients in Group II (p=0.021). There was no difference of both arm power in 31.9 kg in Group I, 34.7 kg in Group II (p>0.56).
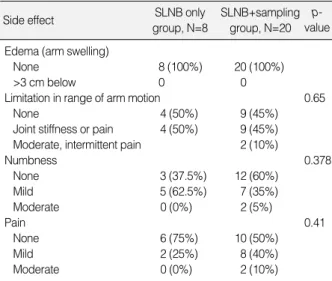
2. The comparision between SLNB group and additional sampling group
No patients had arm swelling, limitation in range of arm Table 2.The comparision with side effect between SLNB group
and ALND group
SLNB (Group I) N (%)
Side effect ALND (Group II)
N (%)
p- value
Edema (Arm swelling) 0.077
None 28 (100) 34 (89.5)
>3 cm below 0 (0) 4 (10.5)
Limitation in range of arm motion
None 13 (46.4) 10 (26.3) 0.195
Joint stiffness or pain 13 (46.4) 22 (57.9) Moderate, intermittent 2 (7.1) 6 (15.8)
joint pain
Numbness 0.570
None 15 (53.6) 16 (42.1)
Mild 12 (42.9) 19 (50.0)
Moderate 1 (3.6) 3 (7.9)
Pain 0.936
None 16 (57.1) 20 (52.6)
Mild 10 (35.7) 15 (39.5)
Moderate 2 (7.1) 3 (7.9)
SLNB=sentinel lymph node biopsy; ALND=axillary lymph node dissec- tion.
Table 3.Means VAS (S.D) for subjective symptoms in axillary morbidity
SLNB (Group I) ALND (Group II) p-value Arm edema (VAS) 1.0±0.0 1.21±0.62 0.079 Limitation of ROM (VAS) 1.61±0.63 1.89±0.65 0.076 Tingling, numbness (VAS) 1.50±0.58 1.66±0.63 0.30 Axillary pain (VAS) 1.50±0.64 1.55±0.65 0.74 VAS=visual analogue scale; SLNB=sentinel lymph node biopsy; ALND=
axillary lymph node dissection; ROM=range of motion.
Table 4.Comparision of objective symptoms between SLNB (Group I) and ALND (Group II)
SLNB (Group I) N (%)
ALND (Group II)
N (%) p-value Arm circumference
Upper C10
<2 cm 27 (96.4) 32 (84.2) 0.099
≥2 cm 1 (3.6) 6 (15.8)
Lower C10
<2 cm 28 33 0.046
≥2 cm 0 5
ROM Flection
No 16 (57.1) 11 (28.9) 0.021
Yes 12 (42.9) 27 (71.1)
Abduction
No 17 (60.7) 20 (52.6) 0.513
Yes 11 (39.3) 18 (47.4)
Arm power
kg 31.93 34.66 0.564
SLNB=sentinel lymph node biopsy; ALND=axillary lymph node dis- section; ROM=Rang of motion; C10=10 cm above lateral epicondyle of olacreon.
Table 5.The comparision with side effect between SLNB only group and additional sampling group
SLNB only group, N=8
Side effect SLNB+sampling
group, N=20 p- value Edema (arm swelling)
None 8 (100%) 20 (100%)
>3 cm below 0 0
Limitation in range of arm motion 0.65
None 4 (50%) 9 (45%)
Joint stiffness or pain 4 (50%) 9 (45%) Moderate, intermittent pain 2 (10%)
Numbness 0.378
None 3 (37.5%) 12 (60%)
Mild 5 (62.5%) 7 (35%)
Moderate 0 (0%) 2 (5%)
Pain 0.41
None 6 (75%) 10 (50%)
Mild 2 (25%) 8 (40%)
Moderate 0 (0%) 2 (10%)
SLNB=sentinel lymph node biopsy.
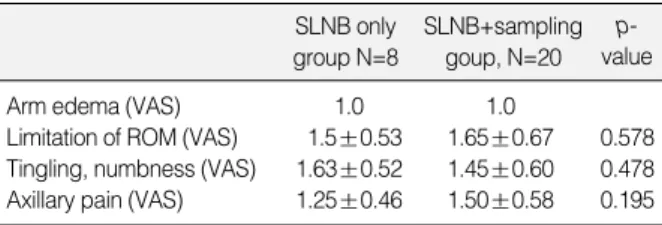
motion, numbness, and pain in both SLNB only and addi- tional sampling and by visual analogue scale, there no diffe- rence in subjective and objective side effect in both group (Table 5-7).
DISCUSSION
Recommended surgical care for invasive breast cancer includes removal of the primary tumor and a level I and II ALND. The status of the axillary node helps to determine the prognosis and guide treatment decisions. Unfortunately, side-effects after ALND are relatively common. The side- effect incidence varies with the length of follow-up, mea- surement techniques used, and other patient- and treat- ment-related factors.(7) The side-effect include upper-ex- tremity lymphedema (6-49%), arm numbness/tingling (7-75
%), pain (16-54%), impaired shoulder morbidity (4-45%), arm weakness (19-35%), and infections in the breast, chest, or arm.(8, 9)
Recently, a less invasive procedure, SLNB, has been de- veloped to diagnosing the status of axilla in early breast cancer. The sentinel lymph node is the nearest lymph node from the tumor, and the possibility of first metastasis from tumor cell is high, and so the sentinel lymph node is the
guard of lymph node metastasis. Morton et al.(10) initially described using blue dye to identify the SLNB in patitents with melanoma. In 1993, Krag et al.(11) first reported the use of SLNB in breast cancer.(11) Subsequent studies by Gi- uliano et al., using blue dye in patients with early breast can- cer, demonstrated its feasibility and accuracy. They found 95.6% accuracy in prediction the status of the axilla, but they also demonstrated that there was a significant learning curve for the technique, with successful identification in only 65.5%
of cases.(12) Albertini et al.(13) subsequently reported on the additional use of the radioisotope and a gamma detection probe. They successfully identified the SLNB in 92% of pa- tients by using a combination of blue dye and radioisotope.
Other studies have validated the accuracy of SLNB.(14, 15) SLNB has become an acceptable alternative to ALND for patients with clinically negative lymph node. Surgical prac- tice for staging the axilla for breast cancer is changing AL- ND to SLNB because SLNB has been found to be accurate in determining whether metastatic disease has spread to the axilla. The availability of SLNB excists in aspects of diag- nostic accuracy and decrease of axillary morbidity after con- ventional axillary dissection. Potential side effect of SLNB are likely to be less than with an ALND because there is less extensive surgery in the axilla. Recently, pubulished data showed no sensory morbidity after SLNB at a median follow- up of 39 months.(16) Schrenk et al.(17) reported less postope- rative arm pain, numbness and arm motion restriction after SLNB at a follow-up period of 15.4 months. The evaluation of morbidity after ALND and SLNB is under investigation in ongoing randomized trials as the NSABP B-32 and the AL- MANAC trial. There are many comparisive report between conventional axillary lymph node dissection and SLNB for Table 6.Comparision of objective symptoms between SLNB
only group and additional sampling group
SLNB only group, N=8
SLNB+sampling group, N=20
p- value Arm circumference
Upper C10
<2 cm 8 (100%) 19 (95%) 0.407
≥2 cm 0 1 (5%)
Lower C10
<2 cm 8 20
≥2 cm 0 0
ROM Flexion
No 6 (75%) 10 (50%) 0.218
Yes 2 (25%) 10 (50%)
Abduction
No 6 (75%) 11 (55%) 0.318
Yes 2 (25%) 9 (45%)
Arm power
kg 15.44 14.13 0.709
SLNB=sentinel lymph node biopsy; ROM=Rang of motion; C10=10 cm above lateral epicondyle of olacreon.
Table 7.Means VAS (S.D) for subjective symptoms in axillary morbidity between SLNB only group and additional sampling group
SLNB only group N=8
SLNB+sampling goup, N=20
p- value
Arm edema (VAS) 1.0 1.0
Limitation of ROM (VAS) 1.5±0.53 1.65±0.67 0.578 Tingling, numbness (VAS) 1.63±0.52 1.45±0.60 0.478 Axillary pain (VAS) 1.25±0.46 1.50±0.58 0.195 VAS, visual analogue scale; SLNB=sentinel lymph node biopsy; ROM=
Rang of motion.
postoperative axillary morbidity. A single-institution study has shown a reduction in arm numbness, arm pain, arm morbidity and lymphedema after sentinel lymph node dis- section as compared with ALND.(16) Another recently pu- bulished study compared side effects between patients having an SLNB and ALND along with breast conserving surgery and found that SLNB patients had less arm swelling than fewer subjective arm complaint. (18) Swenson et al.(19) an- nounced that SLND decreases the degree of interference with daily life caused by arm symptoms. They repeatedly analyzed with serial time (postoperative 1 month, 6 month, and 12 month). At 1 month, SLND patjents reported less pain, numbness, limitation in rang of motion (ROM), and seromas than ALND patients. At 6 months, SLND patients had less pain, numbness, and arm swelling and at 12 months, SLND patients had less numbness, and arm swelling, and limi- nation in ROM than ALND patients. At 1 months, pain, num- bness and limitation in ROM interfered significantly more with daily life for ALND patients. At 6 and 12 months, only numbness interfered more with daily life for ALND patients.
On conclusion, SLND was associated with fewer side effects than ALND at all time patients.(19)
Our study corroborates previous work by Schrenk and Swenson that patients experience less than pain, numbness, and ROM restriction after SLND than ALND. Additional axillary lymph node sampling, suspicious and swelling lymph node sampling, did not increased the incidence of axillary morbidity. If sentinel lymph node and suspicious lymph node was founded intraoperatively, additional lymph node sam- pling may not increase the axillary morbidity. In compari- son with previous study, it was short term period of posto- perive day, and then it was not influenced with adjuvant therapy, such as radiation therapy, chemotherapy. Our study may be primarily influenced by axillary operation method.
The degree of arm swelling in the early postoperative pe- riod is commonly observed and tends to settle spontanously within a matter of weeks.(20) Much of this variation is due to different levels of awareness of the problem, different techniques for measuring arm volume and lack of a univer- sal definition of what degree of swelling constitutes ‘lym- phedema’, as well as genuine differences resulting from var- iation in clinical practice. But the present study was evaluat-
ed in immediate postoperative period, and then there are no effect of spontanous resolution.
Kissen and colleagues, reported a subjective prevalence of arm swelling, as noted by either patients or observer, of 14 percent, but on measurement of volume excess compared with the contralateral arm, 25 percent exceeded the 200 mL cut-off that had been adopted for this study.(21)
In the present study, we evaluate arm swelling between subjectively by visual analog scale and objectively by gonio- metric measurement. In both evaluation, ALND slightly in- creased arm swelling in comparison to SLNB. In the mor- bidity of shoulder motion, subjectively ALND didn’t increas- ed the limitation of shoulder motion, but objectively incre- ased the limitation of shoulder motion in comparision to SLNB. In our study, Numbness was reported in 57.9% of the patients after ALND in contrast to 46.5% in the SLNB group. There are no significant difference in both group, but it is difficult that there was truly no difference due to limitation in number of patient with additional sampling.
We suggest that this may be due to the description of sen- sory qualities of numbness by word description as ‘pain’,
‘tugging’.
In the present study, we used a validated measurement instruments to specify reliability patients’subjective ex- perience of postoperative morbidity after SLNB in compari- son to ALNB. To our knowledge, this is one of the first re- port to compare various aspect of arm/shoulder morbidity after different types of axillary surgery in early postopera- tive period. However, despite the analysis of many cova- riates with different measurement instruments a potential limitation of our study may be the small sample size.
CONCLUSION
SLNB and sampling results in less axillary morbidity com- pared to conventional axillary dissection, especiailly in term of arm swelling and restriction of motion. SLNB and suspi- cious lymph node sampling did not increase postoperative axillary morbidity. SLNB may be effective method for dia- gnosis of axillary lymph node metastasis with decreasing the postoperative axillary morbidity.
REFERENCES
1. Son BH, Kwack BS, Kim JK, Kim JH, Hong SJ, Lee JS, et al. Chang- ing patterns in the clinical charateristics of Korean patients with breast cancer during the last 15 years. Arch Surg 2006;141:155-60.
2. Kuehn T, Klauss W, Darsow M, Regele S, Flock F, Maiterch C, et al.
Long term morbidity following axillary dissection in breast cancer patients-clinical assessment, significance for life quality and the im- pact of demographic, oncologic and therapeutic factors. Breast Cancer Res Treat 2000;64:275-86.
3. Peintinger F, Reitsamer R, Stranzi H, Ralph G. Comparision of qu- ality of life and arm complaints after axillary lymph node dissection vs sentinel lymph node biopsy in breast cancer patients. Br J Cancer 2003;89:648-52.
4. Waldman SD. Interventional pain management. 2nd ed. Philadelphia:
WB Saunders; 2001, pp196.
5. Gosselink R, Rouffaer L, Vanhelden P, Piot W, Troosters T, Chris- tiaens MR. Recovery of upper limb function after axillary dissection.
J Surg Oncol 2003;83:204-11.
6. Riddle DL, Rothestein JM, Lamb RL. Goniometric reliability in a clinical setting. Shoulder measurements. Phys Ther 1987;67:668-73.
7. Kakuda JT, Stuntz M, Trivedi V, Klein SR, Vargas HI. Objective assessment of axillary morbidity in breast cancer treatment. Am Surg 1999;65:995-8.
8. Sener SF, Winchester DJ, Martz CH, Feldman JL, Cavanaugh JA, Winchester DP, et al. Lymphedema after sentinel lymphadenectomy for breast cancer. Cancer 2001;92:748-52.
9. Baron RH, Fey JV, Raboy S, Thaler HT, Borgen PI, Temple LK, et al. Eighteen sensations after breast cancer surgery: a comparion of sentinel lymph node biopsy and axillary lymph node dissection. On- col Nurs Forum 2002;29:651-9.
10. Morton DL, Wen DR, Wong JH, Economou JS, Cagele LA, Storm FK, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 1992;124:392-9.
11. Krag D, Weaver D, Ashikaga T, Moffat F, Klimberg VS, Shrirer C, et al. The sentinel node in breast cancer- a multicenter validation
study. N Engl J Med 1998;339:941-6.
12. Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 1994;220:391-401.
13. Albertini JJ, Lyman GH, Cox C, Yeatman T, Balducci L, Ku N, et al. Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA 1996; 276:1818-22.
14. McMasters KM, Tuttle TM, Carlson DJ, Brown CM, Noyes RD, Glaser RL, et al. Sentinel lymph node biopsy for breast cancer: a suitable alternatives to routine axillary dissection in multi-institu- tional practice when optimal technique is used. J Clin Oncol 2000;
18:2560-6.
15. Giuliano AE, Dale PS, Turner RR, Morton DL, Evans SW, Krasne DL. Improved axillary staging of breast cancer with sentinel lym- phadenectomy. Ann Surg 1995;222:394-9.
16. Giuliano AE, Haigh PI, Brennan MB, Hansen NM, Kelley MC, Ye W, et al. Prospective observational study of sentinel lymphadenec- tomy with out further axillary dissection in patients with sentinel node- negative breast cancer. J Clin Oncol 2000;18:2553-9.
17. Schrenk P, Rieger R, Shamiyeh A, Wayand W. Morbidity following a sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer 2000;88:608-14.
18. Burak WE, Hollenbeck ST, Zervos EE, Hock KL, Kemp LC, Young DC. Sentinel lymph node biopsy results in less postoperative mor- bidity compared with axillary lymph node dissection for breast cancer.
Am J Surg 2002;183:23-7.
19. Swenson KK, Nissen MJ, Ceronsky C, Swenson L, Lee MW, Tuttle TM. Comparision of side effects between sentinel lymph node and axillary lymph node dissection for breast cancer. Ann Surg Oncol 2002;9:745-53.
20. Mortimer PS. The pathophysiology of lymphedema. Cancer 1998;
83(Suppl 12):2798-802.
21. Kissin MW, Querci della Rovere G, Easten D, Westbury G. Risk of lymphedema following the treastment of breast cancer. Br J Surg 1986;73:580-4.