790
목 적: 슬관절 내측 구획에 국한된 골관절염 환자에서 경골 근위부 개방형 설상 절골술을 시행하고 그 임상적 및 방사선학 적 결과를 폐쇄형 설상 절골술과 비교하였다.
대상 및 방법: 골관절염으로 경골 근위부 개방형 절골술 후 2년 이상 추시가 가능하였던 27명 29예(A군), 비교군으로는 폐쇄형 절골술을 시행했던 30명 30예의 환자(B군)를 대상으로 하였다. 방사선학적으로 Ahlback에 의한 관절염의 정도, 대퇴-경골각, 경골의 관상면 정열 및 후방 경사도와 Insall-Salvati 방법에 의한 슬개골의 높이의 변화를 측정하여 비교하 였으며, 임상적으로는 HSS 점수를 측정하였다.
결 과: 개방형 군에서 수술 전에 측정한 대퇴-경골각은 내반 4.2°, 경골의 정열은 5.3° 내반 및 7.9°의 후방 경사, Insall-Sal- vati ratio는 0.93이었으며 폐쇄형 군에서도 유사한 수치를 보였다. 개방형 군에서 2년 추시 대퇴-경골각은 외반 7.7°, 경골 의 정열은 1.3°의 외반으로 수술 전에 비해 의의있는 교정을 보였으며, Insall-Salvati ratio는 0.92로 수술 전에 비해 변화가 없었다. 그러나, 경골의 후방 경사도는 2년 추시상 10.7°로 수술 전에 비해 약 3° 이상의 증가를 보였다. 폐쇄형 군의 2년 추시에서는 개방형 군과 의의 있는 차이는 없었으나, 경골의 후방 경사도는 수술 전 8.7°에서 2년 추시상 3.7°로 의의있는 감소를 보였다. HSS 점수는 개방형 군에서 수술 전 74점에서 2년 추시 93점으로 향상되었으며, 폐쇄군의 변화와 의미 있 는 차이는 없었다. 합병증으로는 개방형 군에서는 지연유합 1예 외에 다른 합병증은 관찰되지 않았으나, 폐쇄형 군에서 천 비골 신경 손상 3예, 지연유합 1예가 발생하였다.
결 론: 개방형 설상 절골술은 신경 혈관 합병증이 없이 폐쇄형과 비슷한 방사선학적 및 임상적 결과를 얻을 수 있는 비교 적 간단하며 안전한 술식으로 생각되나 후방 경사도의 증가의 방지를 위하여 동일한 정도의 전∙후방 개방에 유의해야 할 것으로 생각된다.
색인 단어: 슬관절 퇴행성 관절염, 개방형 설상 절골술, 폐쇄형 설상 절골술
Purpose: To evaluate the clinical and radiological results of an opening wedge osteotomy for an os- teoarthritic knee, and compared these results with those of a closing wedge osteotomy.
Materials and Methods: The study included 27 patients (29 cases) with an opening wedge osteotomy (Group A) and 30 patients (30 cases) with a closing wedge osteotomy (Group B). The radiological results obtained regarding the degree of osteoarthritis, femur-tibia angle, tibial alignment, posterior tibial slope and patellar height using the Insall-Salvati’s method were analyzed. HSS score was used for evaluation of the clinical results.
Center for Joint Disease, Chonnam National University Hwasun Hospital, Jeonnam; Department of Orthopedics, Chonnam National University School of Medicine*, Gwangju, Korea
Jun Yub Lee, M.D., Jong Keun Seon, M.D., Eun Kyoo Song, M.D.*, Taek Rim Yoon, M.D.*, Seung Young Cheon, M.D., and Keun Young Lim, M.D.*
Comparison of High Tibial Osteotomy - Opening versus Closing Wedge Osteotomy -
790
경골 근위부 절골술 비교
- 개방형 대비 폐쇄형 설상 절골술 -
이준엽∙선종근∙송은규*∙윤택림*∙천승영∙임근영*
화순전남대학교병원 관절센터, 전남대학교 의과대학 정형외과학교실*
790 790 통신저자 : 천 승 영
전남 화순군 화순읍 일심리 160 화순전남대학교병원 관절센터
TEL: 061-379-7676∙FAX: 061-379-7681 E-mail: [email protected]
Address reprint requests to Seung Young Cheon, M.D.
Center for Joint Disease, Chonnam National University Hwasun Hospital, 160 Ilsim-ri, Hwasun-eup, Hwasun-gun, Jeonnam 519-809, Korea Tel: +82.61-379-7676, Fax: +82.61-379-7681
E-mail: [email protected]
. .
최근 인공 슬관절 부분 치환술(unicondylar knee arthroplasty)의 좋은 결과로 인해 경골 근위부 절골술 은 수술의 빈도가 줄어들기는 하였으나 비교적 젊은 나 이의 환자에서 내반변형을 가진 슬관절 내측 구획에 국 한된 골관절염에 유용한 술식으로 알려져 있다2,4,5,8,19,28).
절골술 방법으로는 폐쇄형 설상 절골술이 널리 이용되 어 왔으며 수술 후 8-10°의 외반각을 얻었을 경우에는 그 장기 추시 결과도 비교적 좋은 것으로 보고되고 있다15,17). 그러나 폐쇄형 절골술은 비골 절골술 또는 근위부 경비 관절 해리술로 인한 신경혈관 합병증이 약 15% 보고되 며23), 추후 지속적인 퇴행성 관절염의 진행으로 슬관절 전치환술을 필요로 하는 경우에는 연부조직 구축으로 인 해 외측부 도달이 힘들고 경골 근위 외측 골결손으로 인 한 변형으로 정확한 하지 정렬을 얻기 어려운 단점이 있
다10,25). 이에 반해 개방형 설상 절골술은 경골 내측부의
골을 회복시켜 변형을 교정함으로써 추후 슬관절 치환술 을 용이하게 하며 술식이 간단하고 조기 운동이 가능하 다는 장점이 있으며 근래에 몇몇 저자들에 의해 좋은 결 과가 보고되고 있다6,11). 이에 저자들은 슬관절 내반 변 형을 동반한 골관절염 환자에서 개방형 설상 절골술을 시행한 후 임상적 및 방사선학적 추시 결과를 폐쇄형 설 상 절골술의 결과와 비교하고자 하였다.
대상 및 방법
슬관절 내반 변형을 동반한 골관절염 환자에서 수술 후 2년 이상 추시가 가능하였던 개방형 설상 절골술을 시행받은 27명 29예를 대상으로 하였으며, 대조군으로 수술 전 나이, 관절염의 정도 및 대퇴-경골각이 비슷한
폐쇄형 설상 절골술을 시행 받은 30명 30예의 환자를 대상으로 하였다. 수술 적응증으로는 내반 변형이 동반 된 슬관절 내측에 국한된 원발성 골관절염 환자 중 보존 적 치료에 반응하지 않은 환자를 대상으로 하였으며, 수 술 전 관절염의 정도는 Ahlback1)등급 1과 2가 대부분 (88%)을 차지하였다. 또한 15 이상의 내반 변형, 10 이 상의 굴곡 구축 및 불안정성이 있는 환자는 제외시켰다.
두 군 간의 평균 연령, 체중, 신장 및 수술 전 관절염의 정도는 차이가 없었다(Table 1).
1. 수술 방법
슬개건 내측부를 따라 종절개를 가한 후 슬건의 기시부 를 확인하고 천층 내측부 인대의 원위부를 노출 시킨 뒤 C-arm을 보면서 경골 내측부에서 후외방으로 유도선을 비스듬히 삽입하였다. 개방시 안정성을 유지하기 위하 여 가능한 외측 피질골을 손상시키지 않는 정도의 절골 술을 시행하였으며, 고관절-슬관절-족관절(HKA) 축 이 슬관절 외측 경골극을 지나도록 내측을 개방시킨 후 경골의 시상면에서 가능한 중간부보다 후방에 Open- ing wedge osteotomy system (Arthrex, Naples, Florida, USA)을 사용하여 고정하였으며, 10 mm 미 만의 개방이 필요한 경우에는 골이식을 시행하지 않았으 며, 10 mm 이상의 교정이 필요한 경우는 전례에서 이 종골(Lubboc�)을 이용한 골이식을 시행하였다. 수술 후 약 3-4주간 장하지 석고붕대 고정을 시행한 상태로 하지 직거상 및 사두근 강화운동을 시행하였으며, 그 후 슬관절 보조기하에 관절 운동을 시행하였고 체중 부하는 수술 후 2개월 후부터 허용하였다.
Results: Preoperatively, there were no significant differences between the two groups regarding the degree of osteoarthritis, the femur-tibia angle, tibial alignment, posterior tibial slope, and patellar height.
Two years after surgery, the femur-tibia angle and tibial alignment were significantly improved to 7.7°
valgus and 1.3° valgus, respectively, and the patellar height was not changed significantly in group A.
Similar results were obtained in group B. The tibial posterior slope increased from 3° to 10.7° in group A and decreased from 4° to 3.7° in group B. Clinically, the HSS score was improved from 74 points preop- eratively to 93 points 2 years postoperatively in the opening group, and was similar to the improvement observed in the closing group. The complications included 1 delayed union in the opening group, and 3 cases of superficial peroneal nerve palsy and 1 delayed union in the closing group.
Conclusion: An opening wedge osteotomy is a relatively simple and safe procedure that gives similar radiological and clinical outcomes to a closing wedge osteotomy, without peroneal nerve palsy. Howev- er, surgeons should take care in preventing an increase in the tibial posterior slope.
Key Words: Osteoarthritic knee, Opening wedge osteotomy, Closing wedge osteotomy
. .
2. 연구 방법
수술 전 및 수술 후 2년에 방사선학적 평가 및 임상적 평가를 시행하였으며, 통계학적 분석은 Statistical Pro- duct and Service Solution (SPSS, version 11)의 Chi-square test와 Mann-Whitney U test를 이용 하였으며 신뢰 구간은 95%로 하였다.
1) 방사선학적 평가
체중부하 직립 전후면 사진에서 관절염의 정도는 Ahlback1)에 의한 방사선학적 분류를, 대퇴 경골각은 Bauer 등2)의 방법에 의해 대퇴골과 경골의 해부학적 축 이 이루는 각을 측정하였다. 또한 경골의 정열은 전후면 사진에서 경골 고평부에 수직인 선과 경골의 해부학적 축이 이루는 각을 관상면 정열로, 측면 사진에서 경골
고평부에 수직인 선과 경골 해부학적 축이 이루는 각을 후방 경사도로 측정하였으며 슬개골의 높이 평가를 위해 Insall-Salvati ratio9)를 측정하였다(Fig. 1).
2) 임상적 평가
임상적 평가는 동통, 기능, 관절 운동 범위, 근력, 관절 의 굴곡 변형 그리고 관절의 불안정성으로 구성된 Hos- pital for Special Surgery (HSS) 점수를 이용하였으 며, 각각의 항목에 대해 평가하여 100점을 기준으로 하 였다.
결 과
1. 방사선학적 평가
개방형 절골술군에서 수술 전 관절염은 1등급이 15예, 2등급이 10예, 3등급이 4예이었으며, 대퇴-경골각은 내 반 4.2±1.9°이었다. 경골의 정열은 관상면상에서 5.3± 3.2°의 내반을, 측면상에서는 7.9±3.9°의 후방경사를 보였으며, 슬개골의 높이를 알아보기 위해 측정한 Insall- Salvati ratio는 0.93±0.14°이었다. 폐쇄형 절골술군 에서의 수술 전 관절염의 정도 및 대퇴-경골각과 경골 의 정열 및 슬개골의 높이는 개방형군과 통계학적으로 의의 있는 차이는 보이지 않았다(p>0.05) (Table 2).
지연유합으로 자가골 이식을 시행받은 2예를 제외한 골 유합은 개방형군에서는 15-18주에, 폐쇄형군에서는
Opening wedge osteotomy (n=29)
Closing wedge
osteotomy (n=30) p-value Age (mean, years) 59.6±6.1 61.2±6.6 0.262 Weight (mean, kg) 61.9±6.2 61.8±5.0 0.993 Height (mean, cm) 155.5±4.8 153.2±4.6 0.149 Ahlback grade
1 15 16
2 10 11
3 4 3
Table 1.Details of patients
. .
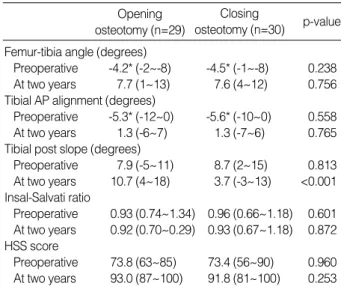
Opening osteotomy (n=29)
Closing
osteotomy (n=30) p-value Femur-tibia angle (degrees)
Preoperative -4.2* (-2~-8) -4.5* (-1~-8) 0.238 At two years 7.7 (1~13) 7.6 (4~12) 0.756 Tibial AP alignment (degrees)
Preoperative -5.3* (-12~0) -5.6* (-10~0) 0.558 At two years 1.3 (-6~7) 1.3 (-7~6) 0.765 Tibial post slope (degrees)
Preoperative 7.9 (-5~11) 8.7 (2~15) 0.813 At two years 10.7 (4~18) 3.7 (-3~13) <0.001 Insal-Salvati ratio
Preoperative 0.93 (0.74~1.34) 0.96 (0.66~1.18) 0.601 At two years 0.92 (0.70~0.29) 0.93 (0.67~1.18) 0.872 HSS score
Preoperative 73.8 (63~85) 73.4 (56~90) 0.960 At two years 93.0 (87~100) 91.8 (81~100) 0.253
*: varus.
Table 2.Comparison of mean value of radiological assess- ment for the 29 knees by opening wedge osteotomy and 30 knees by closing wedge osteotomy
Fig. 1.Illustration demonstrating measurement of the tibial align- ment, posterior tibial slope and patellar height using the Insall- Salvati’s ratio. (A) Tibial alignment ( ) was measured as the angle between the anatomical axis of tibia and a line perpendicular to the tibial plateau on the anteropsterior radiograph. (B) Poste- rior slope ( ) was measured as the angle between the anatomi- cal axis of tibia and a line perpendicular to the tibial plateau on the lateral radiograph. (C) Insall-Salvati’s ratio was measured as the ratio of LL/LP, LL-length of patellar ligament, LP-length of the patella.
A B C
LP
LL
. .
12-18주에 관찰되었다. 수술 후 2년에 관절염은 개방형 군에서 1등급 12예, 2등급 11예, 3등급이 6예이었으며 폐쇄형군에서와 의미 있는 차이는 없었다(p>0.05). 수 술 후 2년의 대퇴-경골각은 개방형군과 폐쇄형군에서 각 각 7.7°, 7.6°로 수술 전에 비해 의의 있는 증가를 보였으 나 두 군 간에 통계학적 차이는 보이지 않았다(p>0.05) (Table2).
경골의 관상면 정열도 수술 전에 비해 두 군 모두에서 의의 있게 내반변형이 외반으로 교정되었으나 두 군 간 의 차이는 보이지 않았으나(p>0.05), 경골의 후방경사 도는 개방형군에서는 수술 전 7.9°에서 수술 후 10.7°로 증가를(Fig. 2), 폐쇄형 절골술군에서는 수술 전 8.7°에 서 수술 후 3.7°로 감소를(Fig. 3) 보여 두 군 간에 뚜렷
한 차이를 보였다(p<0.05)(Table 2). Insall-Salvati ratio는 개방형군에서 수술 전 0.93에서 2년 추시상 0.92, 폐쇄형군에서 수술 전 0.96에서 2년 추시상 0.93으로 폐쇄형군에서 슬개골의 하방 전위가 개방형군 보다 약간 더 많았으나 통계학적으로 의의 있는 차이는 존재하지 않았다(p>0.05)(Table 2).
2. 임상적 평가
개방형 절골술군에서 HSS score는 수술 전 73.8점 에서 2년 추시상 93.0점으로 향상되었으며, 폐쇄형군에 서는 수술 전 73.4에서 최종 추시상 91.8로 향상되어 두 군 간의 차이는 보이지 않았다(p>0.05)(Table 2). 경골 의 후방 경사도 증가에 의한 10° 이상의 신전 제한 및 감
A B
Fig. 2.A 50-year-old woman with opening wedge osteotomy for osteoarthritis. (A) Preoperative radiographs shows 2° varus of femur- tibia angle and 10° posterior slope of tibial plateau. (B) Radiographs at 2 years postoperatively shows that femur-tibia angle was corrected to 7° valgus and posterior slope significantly increased to 17°.
A B
Fig. 3.A 68-year-old woman with closing wedge osteotomy (A) Preoperative radiographs shows 4° varus of femur-tibia angle and 6°
posterior slope of tibial plateau. (B) Postoperative radiographs at 5 years postoperatively shows 6° valgus and 3° anterior slope.
소에 의한 전후방 불안정성은 두 군 모두에서 관찰되지 않았다. 합병증으로는 폐쇄형 절골술 군에서 천 비골신 경 손상 3예 발생하였으나 저절로 회복되었고 개방형군 에서는 관찰되지 않았으며, 지연유합이 개방형군에서는 수술 후 5개월에, 폐쇄형군에서는 수술 후 4개월 각각 1 예 발생하여 자가골 이식술 후 골유합을 얻을 수 있었다.
고 찰
내반 변형을 동반한 슬관절 내측부에 국한된 단구획 퇴 행성 관절염의 수술적 치료로는 경골 근위부 절골술과 인 공 슬관절 부분 치환술(Unicondylar knee arthroplas- ty)이 주로 사용되고 있다. 슬관절 부분치 환술은 최근 좋 은 결과가 보고3,26)됨에 따라 노령 인구에서 증가 추세에 있으나 활동력이 있는 젊은 환자에서는 아직도 경골 근 위부 절골술이 주된 치료법으로 알려져 있다2,4,5,7-9,19,28).
경골 근위부 절골술은 폐쇄형 또는 돔(dome)형의 절 골술이 주로 사용되었으며 5년 추시에서 80-90%의 만 족한 결과를, 10년 이상의 장기 추시에서는 50% 이상에 서 만족할 만한 결과를 보고하였다2,4,5,12,21,23,24,28). 그러 나 폐쇄형 절골술은 술식이 어렵고 비골 절골술 또는 근 위 경비골 관절의 해리술에 따른 신경 및 혈관 손상 등 합병증이 많으며, 외측부 골 절제로 인한 하지 단축과 추후 인공 관절 전치환술이 필요로 하는 경우 변형 및 외 측과 골결손 으로 인해 정확한 정렬을 회복하기 어려울 수 있다는 단점이 있다7,10,25).
이에 반해 개방형 절골술은 술식이 간단하며, 비골 절 골술이 필요하지 않으므로 신경 혈관 합병증을 줄일 수 있으며, 폐쇄형 절골술과는 달리 외측 경골로부터 골을 제거하지 않고 정상적이고 해부학적인 골 형태를 유지함 으로써 후에 인공 관절 치환술이 용이하다는 점과 이완 된 내측부 인대에 적절한 긴장을 줄 수 있다는 장점이 있 다. 그 방법으로는 외고정 기기를 이용한 내측 개방형 절골술이 시도되어 만족할 만한 결과가 보고되면서 개방 형 절골술은 외고정 장치 및 hemicallostasis를 이용한 치료가 주로 사용되었다16,18,27). Weale 등27)은 hemi- callostasis를 이용한 내측 개방형 절골술로 5년 추시 상 89%, 10년 추시상 63%의 생존율을 보고하였다. 그 러나 외고정 장치를 이용한 내측 개방형 절골술은 핀 삽 입으로 인한 핀 경로 감염으로 종종 골수염 및 화농성 관 절염이 보고되며, 환형 외고정 기구의 경우 술식이 복잡
하며 간혹 발생하는 장무지 신건의 마비가 보고된다.
이에 Hernigou 등6)은 장골 이식과 금속판을 이용한 내측 개방형 설상 절골술로 5년 추시상 90%, 10년 추시 상 45%에서 양호 이상의 결과를 보고하고 내고정술을 이용한 개방형 절골술을 권장하였으며, 이 등14)도 19예 에서 금속판을 이용한 내측 개방형 절골술 후 5.3년 추 시상 좋은 결과를 보고하였다.
개방형 절골술 후의 대퇴-경골각 및 경골의 관상면 정 열은 대체적으로 폐쇄형과 비슷하게 보고6,14,18)되고 있으 며 저자들의 경우에도 2년 추시상 두 군 간의 차이는 없 었다. 경골의 후방 경사도는 폐쇄형 절골술의 경우 감소 하나 개방형의 경우 증가할 수 있으며 이는 전방십자인 대 부전이 있는 경우 문제가 되며 경사도의 증가는 경골 의 전방전위를 야기한다. Nakamura 등18)은 개방형 절 골술의 경우 수술 전에 비해 큰 변화를 보이지 않았으나 저자들은 수술 전에 비해 약 3°의 증가를 보였으나 이로 인한 불안정성은 관찰되지 않았다. 경골의 후방 경사도 의 증가는 후외측의 절골술이 부족하여 전방만 개방되어 초래되므로 전방과 후방을 동일한 정도로 개방시키는 것 으로 이를 방지할 수 있을 것이다. 슬개골의 하방전위는 경골 근위부 절골술 후 약 10-30%까지 보고되는 흔한
합병증20,22)으로 Nakamura 등18)은 개방형에서 폐쇄형
보다 슬개골의 하방 전위가 적게 관찰되었다고 하였으나 본 연구에서는 슬개골의 하방전위에 있어 두 군 간의 유 의한 차이는 보이지 않았다(p>0.05). 개방형 절골술 시 사용되는 골이식으로는 장골 자가 이식, 수산화 칼슘이 나 이종골의 사용이 보고6,11,13)되고 있으며, 일반적으로 10 mm 이상의 개방을 요하는 경우 tricortical 자가골 이식이 권장되나, 저자들은 10 mm 이상의 개방이 필요 했던 경우에도 이종골(Lubboc�)을 사용하였으며 지연유 합 1예를 제외한 모든 예에서 불유합은 관찰되지 않았다.
결 론
경골 근위부 개방형 설상 절골술은 시술 방법이 간단 하고 비골 절골술 및 근위 경비골 관절 해리술이 필요하 지 않아 폐쇄형 절골술에 비해 비골 신경 손상 등의 신경 혈관 합병증이 적으며 경골 근위부 골 소실이 적어 추후 퇴행성 관절염의 진행으로 슬관절 전치환술이 필요할 경 우 시술이 용이하다는 장점이 있어 내측 구획에 국한된 슬관절 퇴행성 관절염에 유용한 술식으로 생각된다. 그
러나 경골의 후방 경사도의 증가가 흔히 나타나므로 경 골 후외측의 충분한 절골술 후 동일한 정도의 전∙후방 개방에 유의해야 할 것으로 생각된다.
참고문헌
1. Ahlback S: Osteoarthrosis of the knee: a radiographic investiga- tion. Acta Radiol Diagn (Stockh), 277 (Suppl): 7-72, 1968.
2. Bauer GC, Insall J and Koshino T: Tibial osteotomy in gonar- throsis (osteo-arthritis of the knee). J Bone Joint Surg, 51-A: 1545- 1563, 1969.
3. Broughton NA, Newman JH and Baily RJ: Unicompartmen- tal replacement and high tibial osteotomy or osteoarthritis of the knee. A comparative study after 5-10 years follow-up. J Bone Joint Surg, 68-B: 447-452, 1986.
4. Coventry MB and Bowman PW: Long-term results of upper tibial osteotomy for degenerative arthritis of the knee. Acta Orthop Belg, 48: 139-156, 1982.
5. Coventry MB, Ilstrup DM and Wallrichs SL: Proximal tib- ial osteotomy: a critical long-term study of eight-seven cases. J Bone Joint Surg, 75-A: 196-201, 1993.
6. Hernigou Ph, Medevielle D, Debeyre J and Goutallier D:
Proximal tibial osteotomy for osteoarthritis with varus deformity.
J Bone Joint Surg, 69-A: 332-354, 1987.
7. Insall JN: Osteotomy. In: Insall JN, Windsor RE, Scott WN, Kelly MA, Alietti P eds. Surgery of the knee. New York, Churchill Liv- ingstone, 635-676, 1993.
8. Insall JN, Joseph DM and Msika C: High tibial osteotomy for varus gonarthrosis. A long-term follow-up study. J Bone Joint Surg 66-A: 1040-1048, 1984.
9. Insall JN and Salvati E: Patella position in the normal knee joint.
Radiology, 101: 101-104, 1971.
10. Katz MM, Hungerford DS, Krackow KA and Lennox DW:
Results of total knee arthroplasty after failed proximal tibial osteoto- my for osteoarthritis. J Bone Joint Surg, 69-A: 225-233, 1987.
11. Koshino T, Murase T and Saito T: Medial opening-wedge high tibial osteotomy with use of porous hydroxyapatite to treat medial compartment osteoarthritis of the knee. J Bone Joint Surg, 85-A: 78-85, 2003.
12. Koshino T, Moril T, Wada J, Salto H, Ozawa N and Noyori K:High tibial osteotomy with fixation by a blade plate for medial
compartment osteoarthritis of the knee. Orthop Clin North Am, 20: 227-243, 1989.
13. Kwok TG: Open wedge high tibial osteotomy using allo and auto- genous bone grafts. J West Pacific Orthop Assoc, 29: 93-97, 1992.
14. Lee KW, Ahn TG and Choy WS: Factors affecting the results of proximal tibia opening wedge osteotomy. J Korean Orthop Assoc, 37: 611-616, 2002.
15. Mathews LS, Goldstein SA, Malvitz TA, Katz BP and Kau- fer H:Proximal tibial osteotomy. Factors that influence the dura- tion of satisfactory outcome. Clin Orthop, 229: 193-200, 1988.
16. Magyar G, Toksvig-Larsen S and Lindstrand A: Open wedge tibial osteotomy by callus distraction in gonarthrosis. Operative technique and early results in 36 patients. Acta Orthop Scand, 69:
147-151, 1998.
17. Murphy SB: Tibial osteotomy for genu varum. Indications, pre- operative planning, and technique. Orthop Clin North Am, 25:
477-482, 1994.
18. Nakamura E, Mizuta H, Kudo S, Takagi K and Sakamoto K:Open-wedge osteotomy of the proximal tibia with hemicallota- sis. J Bone Joint Surg, 83-B: 1111-1115, 2001.
19. Odenbring S: Osteotomy for medial gonoarthrosis. Thesis, Lund University, 15-18, 1991.
20. Okamoto R, Koshino T and Morii T: Shortening of patellar ligament and patella baja with improvement of quadriceps muscle strength after high tibial osteotomy. Bull Hosp Jt Dis, 53: 21-24, 1993.
21. Rinonapoli E, Mancini GB, Corvaglia A and Musiello S:
Tibial osteotomy for varus gonarthrosis. A 10- to 21 year follow- up study. Clin Orthop, 353: 185-193, 1998.
22. Scuderi GR, Windsor RE and Insall JN: Observations on patel- lar height after proximal tibial osteotomy. J Bone Joint Surg, 71-A:
245-248, 1989.
23. Sundaram NA, Hallett JP and Sullivan MF: Dome osteotomy of the tibia for osteoarthritis of the knee. J Bone Joint Surg, 68-B:
782-786, 1986.
24. Valenti JR, Calvo R, Lopez R and Canadell J: Long-term evaluation of high tibial valgus osteotomy. Int Orthop, 14: 347- 349, 1990.
25. Windsor RE, Insall JN and Vince KG: Technical considera- tions of total knee arthroplasty after proximal tibial osteotomy. J
Bone Joint Surg, 70-A: 547-555, 1988.
26. Weale AE and Newman JH: Unicompartmental arthroplasty and high tibial osteotomy for osteoarthrosis of the knee. A compar- ative study with a 12 to 17 year follow-up period. Clin Orthop, 302: 134-137, 1994.
27. Weale AE, Lee AS and MacEachern AG: High tibial osteoto-
my using a dynamic axial external fixator. Clin Orthop, 382: 154- 167, 2001.
28. Yasuda K, Majima T, Tsuchida T and Kaneda D: A ten to 15 year follow-up observation of high tibial osteotomy in medial compartment osteoarthritis. Clin Orthop, 282: 186-195, 1992.