The Effect of Graston Technique and Chuna manual therapy combined with Korean Medical Treatment for
fibromyalgia: A Case Report
Myung Kwan Kim, Hyun Ji Kim, Hye Su Kim, Jeong Gyo Jeong, Ju Hyun Jeon
*Dept. of Acupuncture & Moxibustion, College of Korean Medicine, Daejeon University
[Abstract]
Objectives : The purpose of this study was to report the clinical effects of the Graston Technique and Chuna manual therapy, combined with Korean Medical Treatment for fibromyalgia.
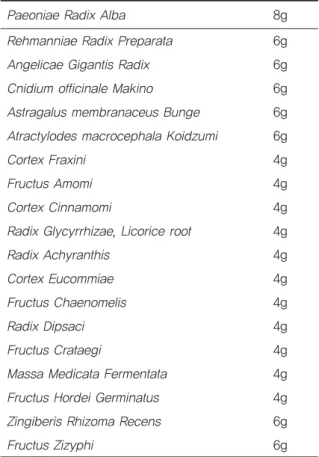
Methods : We treated a patient diagnosed with fibromyalgia. We used acupuncture, the Graston Technique, Chuna manual therapy, pharmacopuncture, herbal medicine, moxibustion and physical therapy. Outcomes were evaluated using the American College of Rheumatology Pre- liminary Diagnostic Criteria (ACR), the Fibromyalgia Impact Questionnaire (FIQ), and the Nu- meric Rating Scale (NRS).
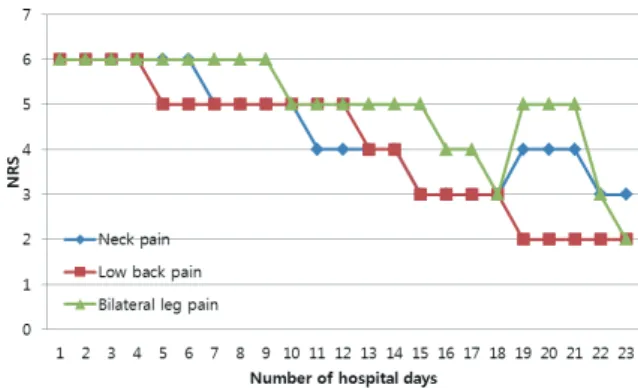
Results : The widespread pain index (WPI) scale score of the ACR decreased from 12 to 9, and the symptom severity scale (SS) score of the ACR decreased from 8 to 6. The FIQ score de- creased from 63.69 to 50.15. On the NRS, lower back pain & lower limb pain decreased from 6 to 2; neck pain from 6 to 3; muscle tenderness & morning stiffness from 6 to 4; fatigue from 6 to 3; urticaria from 6 to 2.
Conclusion : This case study suggests that the Graston Technique and Chuna manual therapy combined with Korean Medical Treatment may be effective treatments for fibromyalgia. How- ever, further studies are needed.
✱ Corresponding author : Dept. of Acupuncture & Moxibustion, College of Korean Medicine, Dae- jeon University, 176-9, Daehung-ro, Jung-gu, Daejeon, Republic of Korea
Tel : +82-42-229-6816 E-mail : [email protected] Key words :
Graston Technique
;Chuna manual theraphy;
Fibromyalgia;
American College of Rheumatology Pre- liminary Diagnostic Criteria (ACR);
Fibromyalgia Impact Questionnaire (FIQ);
Numeric Rating Scale (NRS)
Received : 2017. 05. 24.
Revised : 2017. 07. 19.
Accepted : 2017. 07. 21.
On-line : 2017. 08. 20.
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.