A Preliminary Study on the Effect of Cognitive Bias Modification on the Attribution of Positive Social
Outcomes in Socially Anxious Individuals
Sung Min Da Hye Hong Soo Hyun Park
†Department of Psychology, Yonsei University, Seoul, Korea
Socially anxious individuals tend to disqualify positive social outcomes by attributing such outcomes to others rather than themselves. Previous research suggests that this tendency is a potentially important target of intervention. Thus, the present study aimed to examine the efficacy of cognitive bias modification (CBM) on attribution bias related to positive social out- comes among socially anxious individuals. A total of 159 undergraduate students were randomly assigned to the CBM or placebo group. Based on their level of social anxiety, participants were subsequently classified into either the high (n=75) or low social anxiety groups (n=18). Results showed that CBM was effective in reducing attribution bias related to positive so- cial outcomes in socially anxious individuals. Social anxiety symptoms also diminished after the intervention. The findings of this study provide preliminary evidence regarding the efficacy of CBM for reducing attribution bias related to positive social outcomes and social anxiety.
Keywords: cognitive bias modification (CBM), attribution bias, disqualification of positive social outcomes, social anxiety
Social anxiety disorder is marked by excessive anxiety and fear of social situations (American Psychiatric Association, 2013). The cognitive model posits that socially anxious individuals demon- strate cognitive bias in information processing of negative social outcomes. For example, they may interpret ambiguous events negatively or inflate the probability of negative social outcomes (Clark & Wells, 1995). However, accumulating empirical evidence suggests that socially anxious individuals exhibit cognitive bias concerning positive social outcomes as well (Laposa, Cassin, &
Rector, 2010).
Since socially anxious individuals tend to hold negatively biased mental self-representation, an etiological factor of social anxiety, they may disqualify positive social outcomes that are not compati-
ble with their negative self-appraisals (Weeks, 2010). For example, when others give positive feedback, individuals with high social anxiety often disqualify their own contribution by attributing such outcomes to other’s characteristics (“People will laugh at my jokes even if they aren’t funny, simply because that is the polite thing to do) (Weeks, Heimberg, Rodebaugh, & Norton, 2008). Weeks (2010) has conceptualized this attribution bias as disqualification of posi- tive social outcomes (DPSO). DPSO includes self-oriented DPSO as in failing to attribute positive social outcomes to oneself and other-oriented DPSO as in attributing such outcomes to exterior factors.
This tendency has been identified as an obstacle to treatment in clinical settings (Heimberg & Becker, 2002) because it interferes with challenging and revising their negative internal self-repre- sentation (Jeon & Park, 2011). Moreover, DPSO reportedly medi- ates the relationship between fear of positive evaluation (FPE) and negative automatic thoughts (Weeks & Howell, 2012) and also the
eISSN 2733-4538
†Correspondence to Soo Hyun Park, Department of Psychology, Yonsei University, 50 Yonsei-ro, Seodaemun-gu, Seoul, Korea; E-mail: parksoohyun@
yonsei.ac.kr
Received Nov 5, 2019; Revised Jan 2, 2020; Accepted Jan 18, 2020
relationship between social anxiety and low level of positive affect (Vassilopoulos & Banerjee, 2010). Negative automatic thoughts and diminished capacity to experience positive emotions are ma- jor risk factors for both anxiety (Talkovsky & Norton, 2018) and depressive disorders (Watson & Naragon-Gainey, 2010). Therefore, it can be postulated that DPSO may serve as a bridge between anx- iety and depression. In fact, Hong and Park (2019) have shown that DPSO mediated the relationship between social anxiety and de- pression. Their results indicated that when individuals with high social anxiety disqualify positive social feedback, it can lead to de- pressive symptoms. Considering that DPSO plays a major role in sustaining and exacerbating social anxiety and comorbid depres- sion, DPSO could be an essential intervention target.
One emerging intervention that targets cognitive processing is Cognitive Bias Modification (CBM; Mathews & Mackintosh, 2000).
CBM modifies existing bias by training individuals to focus on more adaptive interpretations. The rationale is that repeated expo- sures to positive interpretation of situations that typically evoke negative interpretations in anxious individuals can modify inter- pretation bias and reduce anxiety symptoms. CBM has shown ro- bust positive effects in modifying interpretation bias and a small treatment effect on anxiety in meta-analyses (Bowler et al., 2012;
Cristea, Kok, & Cuijpers, 2015). The paradigm has also been ap- plied to attention bias (Heeren, Mogoașe, Philippot, & McNally, 2015) and meta-analyses have indicated that CBM has a reliable effect on reducing attention bias (Beard, Sawyer, & Hofmann, 2012).
CBM has focused on cognitive processes pertaining to negative social outcomes. However, as discussed previously, cognitive bias concerning positive social outcomes is a major risk factor for social anxiety and a possible target of intervention. Moreover, research- ers have mainly used CBM to target interpretation or attention bias, but not attribution bias. Therefore, we applied CBM to DPSO – attribution bias with respect to positive social outcomes – in in- dividuals with elevated social anxiety to examine whether CBM demonstrates effects on reducing attribution bias regarding posi- tive social outcomes. We used the original paradigm that Mathew and Mackintosh (2000) utilized by presenting ambiguous scenari- os with a fragmented word because a single session of this para- digm has shown to modify cognitive bias (Mobini et al., 2014;
Yiend et al., 2014).
In this study, we examined whether (1) there will be a difference in DPSO measured by a recognition task between individuals with high versus low social anxiety, (2) CBM will reduce DPSO in indi- viduals with high social anxiety compared to a placebo group, and lastly, (3) CBM intervention will improve social anxiety symptoms.
Method
Participants
Participants were 159 undergraduate students between the ages of 18 and 27 (M=21.23, SD =1.96) enrolled in psychology classes in the Republic of Korea. They received course credit for taking part in the study. We used the simple random assignment method us- ing a computerized number generator to allot participants to the CBM (n=76) or the placebo (n=83) group. In the data analysis process, participants were classified in either the high or low social anxiety group. According to Heimberg, Mueller, Holt, Hope, and Liebowitz (1992), mean SIAS and SPS scores in a community group were 19.9 (SD =14.2) and 12.5 (SD =11.5), respectively. Based on these results, participants with scores one standard deviation higher than the mean scores were allotted to the high social anxiety (n=75;
CBM group =33, placebo group = 42) group, while participants whose scores were less than or equal to the scores of the healthy com- munity group were placed in the low social anxiety group (n=18).
The study was approved by the institutional review board of the university.
Measures
Social Interaction Anxiety Scale (SIAS; Mattick & Clarke, 1998) The SIAS is a 19-item scale assessing fear of general social interac- tion using a 5-point Likert scale ranging from 0 (not at all true) to 4 (very true). In this study, the K-SIAS, translated and validated by Kim (2001), was used. Internal consistency measured as Cronbach’s α ranged from .88 to .94. in Kim (2001) and was .91 in this study.
Social Phobia Scale (SPS; Mattick & Clarke, 1998)
The SPS is a 20-item scale measuring fear of being scrutinized by others using a 5-point Likert scale ranging from 0 (not at all true) to 4 (very true). The K-SPS, translated and validated by Kim (2001),
was used in this study. Cronbach's alpha was .92 in Kim (2001) and .90 in this study.
Disqualification of Positive Social Outcomes Scale (DPSOS;
Weeks, 2010)
The DPSOS is a 13-item measure of self- and other-oriented attri- bution tendencies using a 10-point Likert scale ranging from 0 (not at all true) to 9 (very true). The Korean version of the DPSOS (Han, 2015) was used in this study. Internal consistency was .90 in Han (2015) and .89 in this study.
Fear of Positive Evaluation Scale (FPES; Weeks, Heimberg, &
Rodebaugh, 2008)
The FPES is a 10-item measure of one’s fear of positive evaluation using a 10-point Likert scale ranging from 0 (not at all true) to 9 (very true). The K-FPES, translated and validated by Park, Lee, and Oh (2010) was used in this study. Internal consistency was .85 in Park et al. (2010), and .77 in this study.
Fear of Negative Evaluation Scale (FNES; Leary, 1983)
Based on Watson and Friend (1969), the brief FNES was developed to assess fear of negative evaluation. It consists of 12 items rated on a 10-point Likert scale ranging from 0 (not at all true) to 9 (very true). Lee and Choi (1997) translated and validated the K-FNES, and Cronbach’s α was .90. In this study, Cronbach’s α was .90.
Center for Epidemiological Studies-Depression Scale (CES-D;
Radloff, 1977)
The CES-D is a 20-item measure of depressive symptoms in the past week using a 4-point Likert scale ranging from 0 (not at all or less than 1 day) to 3 (nearly every day). Chon, Choi, and Yang (2001) translated and validated the scale. Cronbach’s α was .92 in Chon et al. (2001), and .93 in this study.
Positive Affect and Negative Affect Schedule (PANAS; Watson, Clark, & Tellegen, 1988)
The PANAS is a 20-item measure of positive and negative affect including 10 items related to positive affect (e.g., enthusiastic and proud) and 10 items related to negative affect (e.g., distressed and nervous). The Korean version of the PANAS (Lee, Kim & Lee, 2003)
was used in the present study. Internal consistency was .84 in both Lee et al. (2003) and this study.
CBM
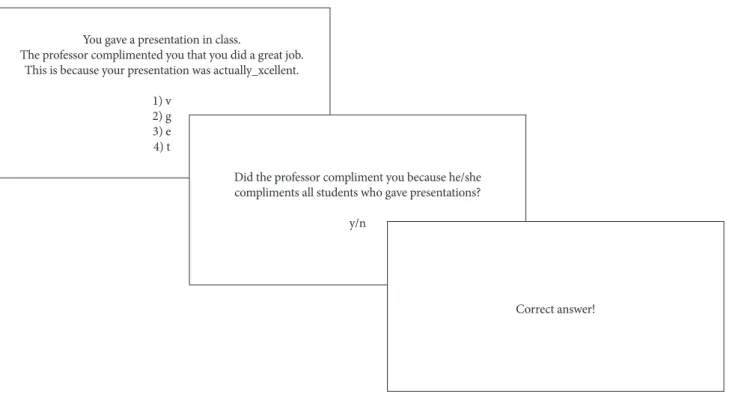
The CBM intervention was made using PsychoPy3 version 3.0. and conducted using an Intel Core i5-5200U CPU, 8.0 GB RAM laptop computer. Because scenarios in CBM must induce cognitive bias, previous studies developed scenarios in accordance with the tar- geted bias and participant characteristics (Kim & Lee, 2019; Sale- mink, Kindt, Rienties, & van den Hout., 2014). In this study, sce- narios were designed based on the Social Stress Questionnaire (Shon, 2001) and included situations that undergraduate students may experience as stressful. Each scenario contained three sen- tences that referred to (1) the situation, (2) any positive social out- comes, and (3) attribution (Figure 1). The last sentence remained ambiguous with a fragmented final word (e.g., “This is because your presentation was actually _xcellent”) and participants were asked to fill in the blank. One hundred forty scenarios were pre- sented to the participants. For the CBM group, there were 100 sce- narios concerning situations in which people received positive so- cial feedback (e.g., “The professor complimented you on your pre- sentation”) and 40 scenarios concerning general positive experi- ences in daily life (e.g., “You bought a delicious cake for your moth- er’s birthday”) to mask the purpose of the task. The placebo group performed a masking task which included 140 scenarios concern- ing positive daily life experiences. After filling in the blank, partic- ipants in the CBM group were asked with yes/no questions wheth- er positive social outcomes in the scenarios are attributable to their own characteristics and abilities or to external factors. If they at- tributed the positive social outcomes to themselves, they received positive feedback (“Correct answer”). If they attributed the out- comes to others, negative feedback (“Wrong answer”) was given.
Recognition task
Recognition task is an established way to measure cognitive bias (Mackintosh, Mathews, Yiend, Ridgeway, & Cook, 2006; Salemink, van den Hout, and Kindt, 2010). During the task, participants read a new set of scenarios that are similar to those in CBM. Then both biased and adaptive interpretations of the situations are presented, and participants rate the likelihood of each interpretation (Mobini,
Reynolds, & Mackintosh, 2013). In this study, ten scenarios were given and there were subsequent comprehension questions with yes/no answers to encourage participants to read scenarios thor- oughly. For example, in the “Telling a joke to friends” scenario, participants read the phrase “You are having a dinner with your friends at an Italian restaurant. You told them a funny joke. Your friends say that it was _ilarious” (fill in the blank). Subsequently, they answered the question “Did you have a dinner with your friends at a Thai restaurant? (yes/no)”.
After answering the comprehension questions, self-attribution and other-attribution of the situation were presented with the title of the scenario. To evaluate whether CBM affected the targeted at- tribution bias or the overall anticipation of social outcomes, posi- tive and negative anticipation (termed “foils”) that were not related to attribution bias were included. For example, for the scenario
“Telling a joke to friends,” the participants read the following state- ments: (1) Your friends genuinely found your joke funny, (2) Your friends said your joke was hilarious only because they did not want to hurt your feelings, (3) The food was delicious, and you had a great time, (4) The food was too expensive, and you did not like the res- taurant. Participants rated the likelihood of each statement based on the scenario that they had read. All statements were answered
using a 4-point Likert scale ranging from 1 (very unlikely) to 4 (very likely) and the mean scores for each of the 4 statements were calculated for analysis. If the mean self-attribution score increased and the mean other-attribution score decreased following the in- tervention, we assumed that the intervention was effective.
Procedure
Participants were told that the purpose of the study was to investi- gate the relationship between memory and positive feedback to prevent potential placebo effects. The participants were fully briefed on the nature of the study after the study. All participants complet- ed self-report questionnaires as pre-intervention measures. The recognition task was then completed to measure participants’ at- tribution bias. For the next 35 minutes, participants in the CBM group received the CBM intervention and participants in the pla- cebo group performed the masking task that did not include any elements addressing cognitive bias. Post-intervention measures were subsequently collected. The study was completed in an hour.
Data Analysis
Data were analyzed using SPSS 25. We conducted an independent samples t-test to see whether there was a difference in attribution You gave a presentation in class.
The professor complimented you that you did a great job.
This is because your presentation was actually_xcellent.
1) v2) g 3) e4) t
Did the professor compliment you because he/she compliments all students who gave presentations?
y/n
Correct answer!
Figure 1. Example of CBM intervention.
bias between the high and low social anxiety groups based on the recognition task. Next, to assess the efficacy of CBM on attribution bias and social anxiety symptoms in the high social anxiety group, we conducted a two-way mixed-model ANOVA. Lastly, we used a paired samples t-test to further investigate the pre- and post-inter- vention differences in the CBM and the placebo groups.
Results
Baseline attribution bias
As shown in Table 1, there were significant differences in attribu- tion bias measured with the recognition task between the high and low social anxiety groups. Individuals with high social anxiety demonstrated the tendency not to attribute positive social outcomes to themselves compared with individuals with low social anxiety (t(91)=2.89, p=.005). In addition, individuals with high social
anxiety had the tendency to attribute positive social outcomes to others compared with individuals with low social anxiety (t(91)=
-2.28, p=.025). There was no significant difference in the general expectation of positive social outcomes between the two groups (t(91)=-.08, p=.938). However, the high social anxiety group re- ported that negative social outcomes were more likely to occur compared to the low social anxiety group (t(91)=-3.45, p=.001).
Table 1. Cognitive Bias in the High versus Low Social Anxiety Group High social
anxiety (N=75) Low social
anxiety (N=18) t p
M (SD) M (SD)
Self-attribution 3.46 (.38) 3.73 (.24) 2.89 .005**
Other-attribution 2.03 (.49) 1.75 (.41) -2.28 .025*
Foil-positive 2.67 (.57) 2.66 (.69) -0.08 .938 Foil-negative 1.73 (.45) 1.34 (.34) -3.45 .001**
*p<.05, **p<.01.
Table 2. Measured Outcome Variables at Pre- and Post-Intervention
Variables Group
(CBM N=33, Placebo N=42)
M (SD)
t(p) Cohen’s d
Group Time Group*Time
Pre- Post- F(p) F(p) F(p) Partial
η2
Self-attribution CBM 3.42 (.41) 3.65 (.33) -4.14*** (.000) -.72 0.78 11.55** 6.50* .08
Placebo 3.49 (.35) 3.52 (.38) -0.62 (.538) -.10 (.380) (.001) (.013) Other-attribution CBM 1.98 (.56) 2.31 (.49) -5.54*** (.000) -.96 4.50* 108.56*** 6.66* .08
Placebo 2.07 (.43) 2.62 (.35) -9.42*** (.000) -1.45 (.037) (.000) (.012)
Foil-positive CBM 2.55 (.49) 2.50 (.67) 0.53 (.597) .09 2.54 0.73 0.003 .00
Placebo 2.77 (.61) 2.72 (.68) 0.69 (.496) .11 (.115) (.396) (.956)
Foil-negative CBM 1.73 (.51) 1.63 (.50) 2.50* (.018) .44 0.83 0.08 5.52* .07
Placebo 1.72 (.39) 1.80 (.44) -1.32 (.194) -.20 (.366) (.779) (.021) Social interaction anxiety CBM 40.48 (8.44) 36.70 (9.09) 3.72** (.001) .65 0.87 24.28*** 0.27 .00
Placebo 41.88 (6.61) 38.81 (10.10) 3.27** (.002) .50 (.355) (.000) (.608)
Social phobia CBM 22.33 (9.62) 20.45 (10.84) 1.85 (.074) .32 1.45 4.68* 0.02 .00
Placebo 25.57 (12.03) 23.90 (15.59) 1.38 (.177) .21 (.232) (.034) (.897) Disqualif-ication of
positive social outcomes CBM 46.06 (19.76) 44.33 (21.53) 1.22 (.231) .21 0.89 4.45* 0.10 .00 Placebo 50.00 (12.85) 47.67 (14.46) 1.80 (.079) .28 (.349) (.038) (.754) Fear of positive evaluation CBM 28.12 (10.83) 25.70 (10.94) 2.60* (.014) .45 12.22** 5.76* 1.26 .02
Placebo 35.64 (9.87) 34.76 (10.92) 0.90 (.372) .14 (.001) (.019) (.266) Fear of negative evaluation CBM 40.03 (9.75) 38.21 (10.03) 3.37** (.002) .59 0.18 10.34** 1.73 .02
Placebo 40.33 (6.98) 39.57 (7.66) 1.33 (.190) .21 (.671) (.002) (.192)
Depression CBM 21.03 (12.35) 20.48 (12.76) 1.36 (.184) .24 0.20 4.75* 0.29 .00
Placebo 19.98 (11.30) 19.07 (11.60) 1.82 (.077) .28 (.656) (.033) (.591)
Positive affect CBM 20.55 (5.99) 20.21 (6.55) 0.28 (.780) .05 1.85 0.14 0.64 .01
Placebo 18.36 (5.36) 19.29 (6.07) -0.90 (.375) -.14 (.178) (.706) (.425)
Negative affect CBM 22.70 (8.17) 20.88 (8.59) 1.38 (.179) .24 0.67 1.77 0.03 .00
Placebo 23.64 (7.83) 22.21 (7.49) 0.75 (.456) .12 (.418) (.188) (.874)
*p<.05, **p<.01, ***p<.001.
Attribution bias outcome measures
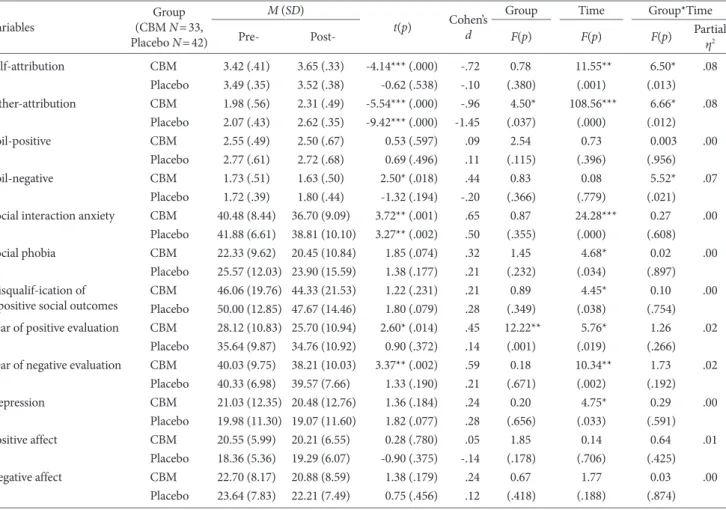
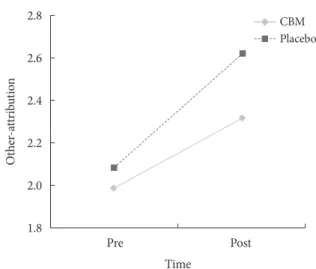
To evaluate the efficacy of CBM, we used a two-way mixed model ANOVA with group (CBM vs. placebo) as the between-subjects factor and time (pre- vs. post-intervention) as the within-subjects factor (Table 2). First, there was a statistically significant main ef- fect of time on self-attribution bias (F(1, 73)=11.55, p=.001) but not assignment (F(1, 73)=.78, p=.380). Also, there was a statisti- cally significant interaction effect between group and time on self- attribution bias (F(1, 73)= 6.50, p=.013, partial η2=.08) (Figure 2), indicating that both groups demonstrated increased self-attribution tendency following the task. However , the CBM group showed a significantly larger increase in self-attribution tendency. Next, there were statistically significant main effects of time (F(1, 73)=108.56, p=.000) and group (F(1, 73)=4.50, p=.037) on other-attribution bias. In addition, there was a statistically significant interaction ef- fect between group and time on other-attribution bias (F(1, 73)=
6.66, p=.012, partial η2=.08) (Figure 3). Prior to the intervention, there was no significant difference in other-attribution between the two groups. Following CBM, however, the CBM group exhibited a significantly lower level of other-attribution tendency. Interesting- ly, degrees of other-attribution tendency increased following the interventions in both groups. There was no significant main nor interaction effect on expectation of positive social outcomes. Also, the main effect of group or time was not significant for anticipation of negative social outcomes. There was, however, a significant in- teraction effect between group and time in anticipation of negative social outcomes (F(1, 73)=5.52, p=.021, partial η2=.07).
Clinical outcomes measures
In respect to clinical outcome measures, the main effect of time on social interaction anxiety (F(1, 73)=24.28, p=.000), social phobia (F(1, 73)=4.68, p=.034), disqualification of positive social outcomes (F(1, 73)=4.45, p=.038), fear of positive evaluation (F(1, 73)=5.76, p=.019), fear of negative evaluation (F(1, 73)=10.34, p=.002), and depressive symptom (F(1, 73)=4.75, p=.033) was significant. How- ever, the interaction effect between time and assignment was not significant. Hence, we used a paired samples t-test and calculated effect sizes in Cohen’s d to further assess potential effects of the CBM intervention (Table 2). In the CBM group, there were statisti- cally significant differences between pre- and post-CBM in social interaction anxiety (t(32)=3.72, p=.001), fear of positive evaluation (t(32)=2.60, p=.014), and fear of negative evaluation (t(32)=3.37, p=.002). However, there were no statistically significant differences in social phobia, disqualification of positive social outcomes, and general emotional state. In the placebo group, on the other hand, the only statistically significant difference was in social interaction anxiety (t(41)=3.27, p=.002) such that following the intervention, social anxiety symptoms in the placebo group significantly de- creased.
Discussion
In this study, we examined the efficacy of CBM in modifying at- tribution bias related to positive social outcomes and associated social anxiety symptoms. First, individuals with high social anxi- Figure 2. Self-attribution at Pre- and Post-intervention.
3.70 3.65 3.60 3.55 3.50 3.45 3.40
Self-attribution
Pre Post
CBM Placebo
Time
Figure 3. Other-attribution at Pre- and Post-intervention.
2.8 2.6 2.4 2.2 2.0 1.8
Other-attribution
Pre Post
CBM Placebo
Time
ety tended to disqualify positive social outcomes by attributing such outcomes to external factors rather than to themselves, which supports findings from previous studies (Hong & Park, 2019;
Weeks, 2010). Individuals with high social anxiety also tended to anticipate that negative social outcomes were more likely com- pared to individuals with low social anxiety. The result is in line with studies which reported that socially anxious individuals ex- pect that negative social outcomes will occur more frequently than individuals without social anxiety (Clark & Wells, 1995; Spokas, Rodebaugh, & Heimberg, 2007).
Secondly, we demonstrated the preliminary efficacy of the CBM intervention on attribution bias. The tendency to attribute positive social outcomes to oneself improved in both the CBM and placebo groups following the intervention, but the degree of improvement was significantly larger in the CBM group showing a medium ef- fect size in regard to the interaction effect. There was no difference between the two groups in anticipation of positive social outcomes, indicating that the change in attribution bias did not stem from a change in general positive perception of social outcomes. The re- sult of this study, although preliminary, holds potential clinical implications, because negative self-appraisal is one of the core fea- tures of social anxiety (Abbott & Rapee, 2004), and attributing positive social outcomes to oneself can help revising negative self- appraisal in a positive way. Moreover, CBM reduced anticipation of negative social outcomes in the CBM group, but not in the pla- cebo group.
We expected that CBM would reduce the tendency to attribute positive social outcomes to others, but this tendency was increased in both the CBM and placebo group after the intervention. The degree of increase was significantly smaller in the CBM group than in the placebo group, yet the result needs further explanation. One possible explanation is that the result may have been due to the in- direct effect of repeated reading of positive social scenarios. Self- attribution is associated with one’s self-appraisal. Other-attribu- tion, however, is implicitly related to the appraisal of both self and others because it implies that one fails to attribute positive social outcomes to oneself and instead attributes such outcomes to others.
Therefore, we believe that reading positive social scenarios repeat- edly during the CBM and placebo task may have not only positive- ly affected participants’ self-appraisal but also in part indirectly af-
fected participants’ appraisal of others positively, thus increasing other-attribution of positive social outcomes. Statements describ- ing other-attribution such as “Your friend said thank you simply because he was moved by your efforts” may be judged to be more likely if one’s appraisal of the other person was positive. However, the degree of increase in other-attribution was smaller while the degree of change in self-attribution was greater in the CBM group compared to the placebo group. These results indicate that CBM was still effective in increasing the tendency to attribute positive social outcomes to oneself rather than to others.
We also examined the efficacy of CBM on social anxiety symp- toms, and there was no significant difference between the two groups as indicated by the interaction effect of time and group.
However, the extent of change in symptoms varied depending on the group. In the CBM group, social interaction anxiety, fear of negative evaluation, and fear of positive evaluation decreased with medium effect sizes following the CBM intervention, whereas in the placebo group, only social interaction anxiety symptoms de- creased. Therefore, our findings partially support the short-term efficacy of CBM on social anxiety symptoms.
However, disqualification of positive social outcomes measured with self-report questionnaires decreased but not at a statistically significant level in the CBM group, even though CBM showed ef- ficacy as measured with the recognition task. When cognitive bias is measured with self-report questionnaires, there have been mixed results, showing less consistent efficacy compared to out- come measured with a recognition task (de Hullu, Sportel, Nauta,
& de Jong, 2017; Steinman & Teachman, 2010). In the recognition task, participants read interpretations that the researcher provid- ed, but a self-report questionnaire requires more in-depth cogni- tive reconstruction such as self-evaluation of their information processing (e.g., “I am able to take compliments easily”) (Glass &
Arnkoff, 1997). Hence, a single session of CBM may not be suffi- cient to engender enduring change in cognitive processes, which is necessary for significant change in self-report questionnaire re- sponses.
In addition, the placebo group also showed improvement in so- cial interaction anxiety, and this may have been the result of the priming effect. The masking task for the placebo group presented positive social situation scenarios to minimize the possible con-
founding effects of negative or neutral scenarios. However, even in the absence of any significant improvement in overall mood, par- ticipants may have been primed to feel positive about social inter- action as a result of having read positive social scenarios. Despite the mixed results, CBM did reduce fear of positive and negative evaluation as well as social interaction anxiety, whereas the place- bo did not affect any variables other than social interaction anxiety.
This study holds several limitations. We applied a single session of CBM and did not collect data at follow-up. Secondly, although the results imply that change in self-attribution tendency was high- ly associated with improvement in social anxiety, we cannot make assumptions regarding the underlying mechanism. Therefore, fu- ture studies should conduct a mediation analysis to clarify this mechanism. Also, even though we examined socially anxious in- dividuals, participants were all undergraduate students, thus not representing the general population. For future studies, compar- ing CBM with diverse placebo conditions including not only posi- tive but also neutral and/or negative social outcomes, or with other established interventions such as traditional CBT is needed. In ad- dition, comparing the effect of CBM that targets different cogni- tive biases such as interpretation, attention and attribution bias and examining their unique effect on social anxiety may also con- tribute to providing a better understanding of cognitive bias relat- ed to social anxiety.
References
Abbott, M. J., & Rapee, R. M. (2004). Post-event rumination and negative self-appraisal in social phobia before and after treatment.
Journal of Abnormal Psychology, 113, 136-144.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Association.
Beard, C., Sawyer, A. T., & Hofmann, S. G. (2012). Efficacy of at- tention bias modification using threat and appetitive stimuli: A meta-analytic review. Behavior Therapy, 43, 724-740.
Bowler, J. O., Mackintosh, B., Dunn, B. D., Mathews, A., Dalgleish, T., & Hoppitt, L. (2012). A comparison of cognitive bias modifi- cation for interpretation and computerized cognitive behavior therapy: Effects on anxiety, depression, attentional control, and interpretive bias. Journal of Consulting and Clinical Psychology, 80, 1021-1033.
Chon, K. K., Choi, S. C., & Yang, B. C. (2002). Integrated adapta-
tion of CES-D in Korea. Korean Journal of Health Psychology, 6, 59-76.
Clark, D. M., & Wells, A. (1995). A cognitive model of social pho- bia. In R. G. Heimberg, M. R. Liebowitz, D. A. Hope & F. R.
Schneier (Eds.), Social phobia: Diagnosis, assessment, and treat- ment. New York, NY: Guilford Publications.
Cristea, I. A., Kok, R. N., & Cuijpers, P. (2015). Efficacy of cognitive bias modification interventions in anxiety and depression: Meta- analysis. The British Journal of Psychiatry, 206, 7-16.
de Hullu, E., Sportel, B. E., Nauta, M. H., & de Jong, P. J. (2017).
Cognitive bias modification and CBT as early interventions for adolescent social and test anxiety: Two year follow-up of a ran- domized controlled trial. Journal of Behavior Therapy and Ex- perimental Psychiatry, 55, 81-89.
Glass, C. R., & Arnkoff, D. B. (1997). Questionnaire methods of cognitive self-statement assessment. Journal of Consulting and Clinical Psychology, 65, 911-927.
Han, S. Y. (2015). The relationship between disqualification of posi- tive social outcomes and social anxiety (Unpublished master’s thesis). Seoul National University, Seoul, Korea.
Heeren, A., Mogoașe, C., Philippot, P., & McNally, R. J. (2015). At- tention bias modification for social anxiety: A systematic review and meta-analysis. Clinical Psychology Review, 40, 76-90.
Heimberg, R. G., & Becker, R. E. (2002). Cognitive-behavioral group therapy for social phobia: Basic mechanisms and clinical strategies.
New York, NY: Guilford Press.
Heimberg, R. G., Mueller, G. P., Holt, C. S., Hope, D. A., & Liebow- itz, M. R. (1992). Assessment of anxiety in social interaction and being observed by others: The social interaction anxiety scale and the social phobia scale. Behaviour Therapy, 23, 53-73.
Hong, D. H., & Park, S. H. (2019). Mediating effect of disqualifica- tion of positive social outcomes on the relationship between so- cial anxiety and depression. Korean Journal of Clinical Psycholo- gy, 38, 70-81.
Jeon, Y. J., & Park, K. H. (2011). The relationships between fear of positive evaluation and social anxiety: The mediating effects of interpretation biases of positive social events. Cognitive Behavior Therapy in Korea, 11, 59-73.
Kim, H. S. (2001). Memory bias in subtypes of social phobia (Unpub- lished master’s thesis). Seoul National University, Seoul, Korea.
Kim, S., & Lee, J. S. (2019). Effects of computer-based cognitive bias modification for interpretation on memory, cognitive con- trol, and motivation. Korean Journal of Clinical Psychology, 38, 335-348.
Laposa, J. M., Cassin, S. E., & Rector, N. A. (2010). Interpretation of positive social events in social phobia: An examination of cognitive correlates and diagnostic distinction. Journal of Anxi- ety Disorders, 24, 203-210.
Leary, M. R. (1983). A brief version of the Fear of Negative Evalua-
tion Scale. Personality and Social Psychology Bulletin, 9, 371-375.
Lee, H. H., Kim, E. J., & Lee, M. K. (2003). A validation study of Korea Positive and Negative Affect Schedule: The PANAS scales.
Korean Journal of Clinical Psychology, 22, 935-946.
Lee, J. Y., & Choi, C. H. (1997). A study of the reliability and the validity of the Korean versions of social phobia scales (K-SAD, K-FNE), Korean Journal of Clinical Psychology, 16, 251-264.
Mackintosh, B., Mathews, A., Yiend, J., Ridgeway, V., & Cook, E.
(2006). Induced biases in emotional interpretation influence stress vulnerability and endure despite changes in context. Be- havior Therapy, 37, 209-222.
Mathews, A., & Mackintosh, B. (2000). Induced emotional inter- pretation bias and anxiety. Journal of Abnormal Psychology, 109, 602-615.
Mattick, R. P., & Clarke, J. C. (1998). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy, 36, 455-470.
Mobini, S., Mackintosh, B., Illingworth, J., Gega, L., Langdon, P., Hoppitt, L. (2014). Effects of standard and explicit cognitive bias modification and computer-administered cognitive-behaviour therapy on cognitive biases and social anxiety. Journal of Behav- ior Therapy and Experimental Psychiatry, 45, 272-279.
Mobini, S., Reynolds, S., & Mackintosh, B. (2013). Clinical implica- tions of cognitive bias modification for interpretative biases in social anxiety: An integrative literature review. Cognitive Therapy and Research, 37, 173-182.
Park, S. J., Lee, J. A., & Oh, K. S. (2010). Validation and clinical effi- cacy of the Korean Fear of Positive Evaluation Scale. Korean Jour- nal of Clinical Psychology, 29, 205-221.
Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the general population. Applied Psychologi- cal Measurement, 1, 385-401.
Salemink, E., Kindt, M., Rienties, H., & van den Hout, M. (2014).
Internet-based cognitive bias modification of interpretations in patients with anxiety disorders: A randomized controlled trial.
Journal of Behavior Therapy and Experimental Psychiatry, 45, 186-195.
Salemink, E., van den Hout, M., & Kindt, M. (2010). Generalisa- tion of modified interpretive bias across tasks and domains.
Cognition and Emotion, 24, 453-464.
Shon, J. (2001). The effects of social stress, dysfunctional beliefs, and negative automatic thoughts on social anxiety (Unpublished mas-
ter’s thesis). The Catholic University of Korea, Seoul, Korea.
Spokas, M. E., Rodebaugh, T. L., & Heimberg, R. G. (2007). Cogni- tive biases in social phobia. Psychiatry, 6, 204-210.
Steinman, S. A., & Teachman, B. A. (2010). Modifying interpreta- tions among individuals high in anxiety sensitivity. Journal of Anxiety Disorders, 24, 71-78.
Talkovsky, A. M., & Norton, P. J. (2018). Negative affect and intol- erance of uncertainty as potential mediators of change in comor- bid depression in transdiagnostic CBT for anxiety. Journal of Af- fective Disorders, 236, 259-265.
Vassilopoulos, S. P., & Banerjee, R. (2010). Social interaction anxi- ety and the discounting of positive interpersonal events. Behav- ioural and Cognitive Psychotherapy, 38, 597-609.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063-1070.
Watson, D., & Friend, R. (1969). Measurement of social-evaluative anxiety. Journal of Consulting and Clinical Psychology, 33, 448-457.
Watson, D., & Naragon-Gainey, K. (2010). On the specificity of positive emotional dysfunction in psychopathology: Evidence from the mood and anxiety disorders and schizophrenia/schizo- typy. Clinical Psychology Review, 30, 839-848.
Weeks, J. W. (2010). The disqualification of positive social outcomes scale: A novel assessment of a long-recognized cognitive tenden- cy in social anxiety disorder. Journal of Anxiety Disorders, 24, 856-865.
Weeks, J. W., Heimberg, R. G., & Rodebaugh, T. L. (2008). The fear of positive evaluation scale: Assessing a proposed cognitive com- ponent of social anxiety. Journal of Anxiety Disorders, 22, 44-55.
Weeks, J. W., Heimberg, R. G., Rodebaugh, T. L., & Norton, P. J.
(2008). Exploring the relationship between fear of positive evalu- ation and social anxiety. Journal of Anxiety Disorders, 22, 386-400.
Weeks, J. W., & Howell, A. N. (2012). The bivalent fear of evalua- tion model of social anxiety: Further integrating findings on fears of positive and negative evaluation. Cognitive Behaviour Therapy, 41, 83-95.
Yiend, J., Lee, J. S., Tekes, S., Atkins, L., Mathews, A., Vrinten, M., . . . Shergill, S. (2014). Modifying interpretation in a clinically de- pressed sample using ‘cognitive bias modification-errors’: A dou- ble blind randomized controlled trial. Cognitive Therapy and Re- search, 38, 146-159.