14 Copyright © 2010 The Korean Society of Vascular Neurology
REVIEW ARTICLE
Vascular Neurology 2010;2:14-17 ISSN 2092-6855
Introduction
Atherosclerosis is a serious medical and health care problem, as it is one of the major causes of death world wide.1 Carotid ath- erosclerotic disease, especially, one of the major preventable cau- ses of ischemic stroke. Moreover, carotid intima-media thick- ness (CIMT) can be regarded as an early marker of atherosclero- sis.2 Several studies have shown that increased CIMT confers risk of future stroke and coronary vascular disease.3-9 Total pla- que area (TPA) was also considered to be an another surrogate marker of stroke, myocardial infarction and vascular death than carotid stenosis.10 The atherosclerotic plaque can be character- ized in two different dimensions, size and echogenicity by using externally applied ultrasound on the carotid arteries. Both size and echogenicity of carotid plaques have been shown to predict not only stroke but also other clinical manifestations of athero- sclerosis, such as acute coronary syndromes.11-14 Some studies demonstrated that hypoechoic or anechoic carotid plaques, ei- ther independently or together with stenosis, carry an increased risk of cardiovascular events, such as stroke, transient ischemic attack, myocardial infarction and even to death.15-19 Current tri- als have investigated the role of statin therapy to reduce athero- sclerotic plaque and many studies have demonstrated better outcomes with intensive than with moderate statin treatment.20-22 In addition, some finding reported that more intensive medical therapy based on plaque measurement markedly reduced the rate of carotid plaque progression.23 Although statins rank among the
most extensively studied therapies in contemporary medicine, the optimal target levels for low density lipoprotein-cholesterol (LDL-C) remain controversial. This paper aims to define current and future treatment strategies for atherosclerotic plaque based on current research outcomes and suggest methodology to meas- ure carotid atherosclerotic plaque accurately by using B-mode ul- trasonography.
Carotid Plaque and Morphology Evaluation by Using B-Mode
Ultrasonography
CIMT measurements, TPA and morphology are usually ob- tained using the high-resolution B-mode ultrasonography. B- mode ultrasonography is noninvasive, readily available and easily applicable imaging technique. It allows for visualization of ar- terial wall structures including CIMT, plaque morphology, pla- que surface and fibrous cap. Furthermore, color duplex flow im- aging and power duplex imaging allow to detect carotid stenosis.1 There are several essential considerations to acquire and evalua- te atherosclerotic plaques. As Mannheim consensus defined, plaque is a focal structure encroaching into the arterial lumen of at least 0.5 mm or 50% of the surrounding intima-media thick- ness (IMT) value, or demonstrates a thickness >1.5 mm as meas- ured from the media-adventitia interface to the intima-lumen interface (Fig. 1).24
In the Asymptomatic Carotid Artery Plaque Study measure-
Current Strategies for the Treatment of Atherosclerotic Plaques
Hye Kyong Pae, Gyung Whan Kim
Department of Neurology, Yonsei University College of Medicine, Seoul, Korea
Received August 6, 2010 Revised August 25, 2010 Accepted September 2, 2010 Correspondence Gyung Whan Kim, MD, PhD Department of Neurology,
Yonsei University College of Medicine, 250 Sungsan-ro, Seodaemun-gu, Seoul 120-752, Korea
Tel +82-2-2228-1600 Fax +82-2-393-0705 E-mail gyungkim@yuhs.ac
Lately, there has been an increasing awareness of the importance of total plaque area and mor- phology of the atherosclerotic plaque as a major risk factor for stroke and cerebrovascular disease.
A number of investigators have proposed the use of B-mode ultrasonography to characterize plaque composition and to identify the higher-risk unstable carotid lesion. Recently, multiple studies have been investigated the role of intensive statin therapy for patients with atherosclerosis.
In this review, we will provide a brief overview on methodology of B-mode ultrasonography and clinical trials of high-dose statin treatment. Furthermore, we will discuss the evidence for effects of high-dose statin treatment on atherosclerosis. Vascular Neurology 2010;2:14-17 Key Wordsaa Atherosclerosis, Carotid intima-media thickness, Atherosclerotic plaque,
Echogenicity, B-mode ultrasonography, C-reactive protein, Low density lipoprotein-cholesterol.
online©MLComm
HK Pae, et al.
15 ment protocol, maximum IMT measures were obtained from
walls of three arterial segments of both carotid arteries: the near and far wall of the proximal 8 mm of the internal carotid ar- tery, the near and far wall of the carotid bifurcation beginning at the tip of the flow divider and extending 8 mm proximally, and the near and far wall of the arterial segment extending 8 to 16 mm proximally to the tip the flow divider into the common carotid artery (CCA)(Fig. 2).25
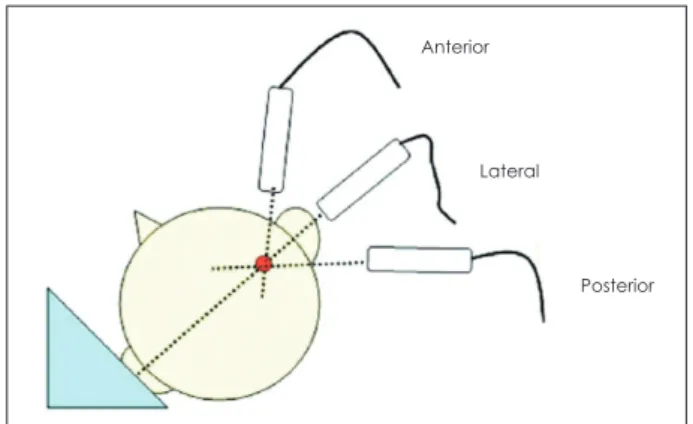
Another tips for accurate carotid plaque screening is follow- ing. Because of the eccentric nature of plaques, a circumferen- tial scan ranging from anterior to posterior angles and imaging the near or far walls of the CCA, bulb and internal carotid ar- tery segments is required to differentiate plaques (Fig. 3).26
Last, plaque echogenicity is assessed by the gray scale median (GSM) using the histogram function. In the Tromsø study, pla- que echogenicity was graded visually from 1 to 4, where grade 1 denotes low echogenicity or echolucency (defined as a plaque ap- pearing black or almost black as flowing blood), and grade 4 de- notes strong echogenicity (defined as a plaque appearing white or almost white, similar to the far wall media-adventitia inter- face).27 In another study, plaque echogenicity was classified by GSM value, which was calculated from pixel analysis within in the range 0-256. Plaques were defined as echolucent if GSM value was lower than 70, and as echorich if GSM was higher than 70.28
High-dose statin therapy
Current studies have reported that high-dose statin treatment results in a greater reduction compared with a moderate thera- py.20-22,29,30 Nissen et al.20 assigned randomly moderate treatment or intensive treatment to patients with coronary artery disease.
This study demonstrated that the mean LDL-C level was reduced from 150.2 mg/dL at baseline to 94.5 mg/dL at 18 months (p<
0.001), and the geometric mean C-reactive protein (CRP) level decreased from 2.9 to 2.3 mg/L (p<0.001) by using intensive statin treatment. Furthermore, Nicholls et al.22 investigated re- lationship between changes in lipoprotein levels and coronary artery atheroma volume. As a result, mean LDL-C levels were re- duced from 124.0 mg/dL to 87.5 mg/dL (a 23.5% decrease; p<
0.001), and high density lipoprotein-cholesterol (HDL-C) level increased from 42.5 mg/dL to 45.1mg/dL (a 7.5% increase; p<
0.001). Substantial atheroma regression was observed in pa- tients with level of LDL-C less than the mean (87.5 mg/dL) dur- ing treatment and percentage increases of HDL-C greater than the mean. Some investigators assessed whether high-intensive statin therapy could regress coronary atherosclerosis as deter- Figure 3. Head position and probe orientation for carotid ultrasound scanning, right-side example.26
Anterior
Lateral
Posterior
Bifurcation and origin of ICA CCA
Figure 1. Drawn representation of carotid tree, with plaque and IMT measurement according to Mannheim consensus. 1: thickness >1.5 mm, 2: lumen encroaching >0.5 mm, 3 and 4: >50% of the surround- ing IMT value.24 IMT: intima-media thickness, ICA: internal carotid ar- tery, CCA: common carotid artery, ECA: external carotid artery.
Plaque 4
3
10 mm length ECA
Bulb
2
Figure 2. Portrayal of common, bifurcation, and internal segments of the carotid artery as defined by protocol in Asymptomatic Carotid Ar- tery Plaque Study.25
External
Ultrasound pulse
Near wall (NW)
Far wall (FW)
Internal (NW & FW)
Bifurcation (NW & FW)
Common (NW & FW) Skin
8 mm
8 mm
8 mm Internal
Lumen
Current Strategies for the Treatment of Atherosclerotic Plaques
16 Vascular Neurology 2010;2:14-17
mined by intravascular ultrasound imaging. This trial reported that very high-intensity statin achieved an average LDL-C of 60.8 mg/dL and increased HDL-C by 14.7%.21 Spence and Hackam23 studied the proportion of patients with plaque progression vs.
regression before and after intensive statin treatment by carotid ultrasound. It has been demonstrated recently that plaque regres- sion decreased abruptly after implementation of intensive treat- ment compared with treating as consensus guidelines.
Discussion
CIMT, TPA and plaque echogenicity are associated with risks of future stroke and cerebrovascular disease (CVD), so many in- vestigators have sought the methodology of carotid ultrasound to predict clinical events. Furthermore, a number of researchers have investigated for decreasing LDL-C and CRP. Nevertheless, the question remains how to measure CIMT and TPA accurately.
The situation is that there is no clinical standard for training and certification for sonographers or readers in spite of causing sig- nificant problems such as low reliability and low agreement each other. Ideally, a national certification and registry for carotid ultrasonography scanning for stroke or CVD risk assessment would be developed. It is necessary that significant CIMT exper- tise be documented to assure the validity and the sensitivity on their researches. The problem also remains how best to treat pa- tients with atherosclerotic plaque without adverse effects. The clinical trials discussed in this review provide substantial sup- port for the institution of intensive statin treatment in diverse clinical setting. Investigators have proved effects of high-dose statin therapy for reducing LDL-C and CRP level and for in- creasing HDL-C as above mentioned. Nevertheless, the Food
& Drug Administration has warned safety and adverse effects of intensive statin treatment and has recommended to prescribe low dose or moderate dose. If new solutions to solve known problems of high dose statin therapy are reconfirmed by the ma- jority of clinical trials, the management for patients with ath- erosclerotic plaque will be established.
REFERENCES
1. Devuyst G, Piechowski-Józwiak B, Bogousslavsky J. Arterial Wall Im- aging. In: Baumgartner RW. Handbook on Neurovascular Ultrasound.
Front Neurol Neurosci. Basel: Karger, 2006;19-26.
2. Grobbee DE, Bots ML, Carotid artery intima-media thickness as an indicator of generalized atherosclerosis. J Intern Med 1994;236:567- 3. Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE. Common 573.
carotid intima-media thickness and risk of stroke and myocardial in- farction: the Rotterdam Study. Circulation 1997;96:1432-1437.
4. Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, et al. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: the Atherosclerosis Risk in Communities (ARIC) Study, 1987-1993. Am J Epidemiol 1997;146:
483-494.
5. Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu CR, Liu CH, et al. The
role of carotid arterial intima-media thickness in predicting clinical coronary events. Ann Intern Med 1998;128:262-269.
6. O’Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N Engl J Med 1999;340:14-22.
7. Chambless LE, Folsom AR, Clegg LX, Sharrett AR, Shahar E, Nieto FJ, et al. Carotid wall thickness is predictive of incident clinical stroke: the Atherosclerosis Risk in Communities(ARIC) Study. Am J Epidemiol 2000;151:478-487.
8. Yamasaki Y, Kodama M, Nishizawa H, Sakamoto K, Matsuhisa M, Ka- jimoto Y, et al. Carotid intima-media thickness in Japanese type 2 dia- betic subjects: predictors of progression and relationship with incident coronary heart disease. Diabetes Care 2000;23:1310-1315.
9. del Sol AI, Moons KG, Hollander M, Hofman A, Koudstaal PJ, Grob- bee DE, et al. Is carotid intima-media thickness useful in cardiovas- cular disease risk assessment? The Rotterdam Study. Stroke 2001;32:
1532-1538.
10. Iemolo F, Martiniuk A, Steinman DA, Spence JD. Sex differences in ca- rotid plaque and stenosis. Stroke 2004;35:477-481.
11. Polak JF, Shemanski L, O’Leary DH, Lefkowitz D, Price TR, Savage PJ, et al. Hypoechoic plaque at US of the carotid artery: an independent risk factor for incident stroke in adults aged 65 years or older. Cardio- vascular Health Study. Radiology 1998;208:649-654.
12. Honda O, Sugiyama S, Kugiyama K, Fukushima H, Nakamura S, Koide S, et al. Echolucent carotid plaques predict future coronary events in pa- tients with coronary artery disease. J Am Coll Cardiol 2004;43:1177-1184.
13. Grønholdt ML, Nordestgaard BG, Schroeder TV, Vorstrup S, Sillesen H.
Ultrasonic echolucent carotid plaques predict future strokes. Circula- tion 2001;104:68-73.
14. Seo Y, Watanabe S, Ishizu T, Moriyama N, Takeyasu N, Maeda H, et al.
Echolucent carotid plaques as a feature in patients with acute coronary syndrome. Circ J 2006;70:1629-1634.
15. Schmidt C, Fagerberg B, Wikstrand J, Hulthe J; RIS Study Group. Mul- tiple risk factor intervention reduces cardiovascular risk in hyperten- sive patients with echolucent plaques in the carotid artery. J Intern Med 2003;253:430-438.
16. Biasi GM, Froio A, Diethrich EB, Deleo G, Galimberti S, Mingazzini P, et al. Carotid plaque echolucency increases the risk of stroke in carotid stenting: the Imaging in Carotid Angioplasty and Risk of Stroke (IC- AROS) study. Circulation 2004;110:756-762.
17. Mathiesen EB, Bønaa KH, Joakimsen O. Echolucent plaques are asso- ciated with high risk of ischemic cerebrovascular events in carotid ste- nosis: the tromsø study. Circulation 2001;103:2171-2175.
18. Grønholdt ML, Nordestgaard BG, Schroeder TV, Vorstrup S, Sillesen H. Ultrasonic echolucent carotid plaques predict future strokes. Circu- lation 2001;104:68-73.
19. Tegos TJ, Kalomiris KJ, Sabetai MM, Kalodiki E, Nicolaides AN. Sig- nificance of sonographic tissue and surface characteristics of carotid plaques. AJNR Am J Neuroradiol 2001;22:1605-1612.
20. Nissen SE, Tuzcu EM, Schoenhagen P, Crowe T, Sasiela WJ, Tsai J, et al. Statin therapy, LDL cholesterol, C-reactive protein, and coronary ar- tery disease. N Engl J Med 2005;352:29-38.
21. Nissen SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, et al. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA 2006;295:1556-1565.
22. Nicholls SJ, Tuzcu EM, Sipahi I, Grasso AW, Schoenhagen P, Hu T, et al. Statins, high-density lipoprotein cholesterol, and regression of cor- onary atherosclerosis. JAMA 2007;297:499-508.
23. Spence JD, Hackam DG. Treating arteries instead of risk factors: a par- adigm change in management of atherosclerosis. Stroke 2010;41:1193- 1199.
24. Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al. Mannheim carotid intima-media thickness consensus (2004-
HK Pae, et al.
17
2006). An update on behalf of the Advisory Board of the 3rd and 4th Watching the Risk Symposium, 13th and 15th European Stroke Con- ferences, Mannheim, Germany, 2004, and Brussels, Belgium, 2006. Ce- rebrovasc Dis 2007;23:75-80.
25. Espeland MA, Craven TE, Riley WA, Corson J, Romont A, Furberg CD.
Reliability of longitudinal ultrasonographic measurements of carotid intimal-medial thicknesses. Asymptomatic Carotid Artery Progression Study Research Group. Stroke 1996;27:480-485.
26. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al.
Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thick- ness Task Force. Endorsed by the Society for Vascular Medicine. J Am Soc Echocardiogr 2008;21:93-111.
27. Joakimsen O, Bønaa KH, Stensland-Bugge E. Reproducibility of ultra- sound assessment of carotid plaque occurrence, thickness, and mor- phology. The Tromsø Study. Stroke 1997;28:2201-2207.
28. Andersson J, Sundström J, Kurland L, Gustavsson T, Hulthe J, Elmgren A, et al. The carotid artery plaque size and echogenicity are related to different cardiovascular risk factors in the elderly: the Prospective In- vestigation of the Vasculature in Uppsala Seniors (PIVUS) study. Lip- ids 2009;44:397-403.
29. LaRosa JC, Grundy SM, Waters DD, Shear C, Barter P, Fruchart JC, et al. Intensive lipid lowering with atorvastatin in patients with stable coronary disease. N Engl J Med 2005;352:1425-1435.
30. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, et al. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med 2004;350:1495-1504.