Korean J Gastroenterol Vol. 66 No. 3, 164-167 http://dx.doi.org/10.4166/kjg.2015.66.3.164 pISSN 1598-9992 eISSN 2233-6869
CASE REPORT
Korean J Gastroenterol, Vol. 66 No. 3, September 2015 www.kjg.or.kr
제1형 신경섬유종증 환자의 파열된 위십이지장동맥 동맥류에서 발생한 위중한 십이지장 궤양 출혈
임규성, 김선용, 임준욱, 전정원, 신현필, 차재명, 주광로, 이정일, 박재준1
경희대학교 의과대학 강동경희대학교병원 내과학교실, 연세대학교 의과대학 강남세브란스병원 내과학교실 소화기내과1
Life-threatening Duodenal Ulcer Bleeding from a Ruptured Gastroduodenal Artery Aneurysm in a Patient with Neurofibromatosis Type 1
Kyu Sung Im, Sunyong Kim, Jun Uk Lim, Jung Won Jeon, Hyun Phil Shin, Jae Myung Cha, Kwang Ro Joo, Joung Il Lee, and Jae Jun Park1
Department of Internal Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Division of Gastroenterology, Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine1, Seoul, Korea
Vasculopathy is rarely reported in neurofibromatosis type 1, but when it occurs it primarily involves the aorta and its main branches. Among vasculopathies, aneurysmal dilatation is the most common form. Although several case reports concerning aneurysms or pseudoaneurysms of visceral arteries in neurofibromatosis type 1 patients have been reported, there are no reports describing gastroduodenal artery aneurysms associated with neurofibromatosis type 1. We experienced a case of life-threatening duodenal ulcer bleeding from a ruptured gastroduodenal artery aneurysm associated with neurofibromatosis type 1. We treated our patient by transarterial embolization after initial endoscopic hemostasis. To our knowledge, this is the first reported case of its type. High levels of suspicion and prompt diagnosis are required to select appropriate treatment options for patients with neurofibromatosis type 1 experiencing upper gastrointestinal bleeding. Embolization of the involved arteries should be considered an essential treatment over endoscopic hemostasis alone to achieve complete hemostasis and to prevent rebleeding. (Korean J Gastroenterol 2015;66:164-167)
Key Words: Neurofibromatoses; Duodenal ulcer; Hemorrhage; Aneurysm, ruptured; Embolization, therapeutic
Received May 1, 2015. Revised May 26, 2015. Accepted May 26, 2015.
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2015. Korean Society of Gastroenterology.
교신저자: 박재준, 06273, 서울시 강남구 언주로 211, 연세대학교 의과대학 강남세브란스병원 내과학교실 소화기내과
Correspondence to: Jae Jun Park, Division of Gastroenterology, Department of Internal Medicine, Gangnam Severance Hospital, Yonsei University College of Medicine, 211 Eonju-ro, Gangnam-gu, Seoul 06273, Korea. Tel: +82-2-2019-4371, Fax: +82-2-3463-3882, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
INTRODUCTION
Neurofibromatosis type 1 is an autosomal dominant dis- order of variable penetration affecting 1 in 3,000 people that predominantly involves abnormal growth of neuroectodermal tumors in the peripheral nervous system. Other clinical mani- festations include café-au-lait spots, Lisch nodules of the iris, meningeal tumors and skin fold freckling.1,2 Besides these features, vasculopathy sometimes occurs with neurofibro-
matosis. The pathogenesis of neurofibromatosis vasculop- athy is not completely understood but may be associated with dysfunction of the neurofibromin in vascular smooth muscle and endothelial cells.3-5 Neurofibromatosis type 1 is caused by mutations of NF1 gene, which encodes neurofibromin.6 Aneurysm formation in neurofibromatosis type 1 may be at- tributable to friable vascular structure secondary to arterial dysplasia or vascular invasion by neurofibroma.
Vascular lesions occur in 3.6% of patients with neuro-
Im KS, et al. Duodenal Ulcer Bleeding in Neurofibromatosis Type 1 165
Vol. 66 No. 3, September 2015 Fig. 1. Photograph of the patient shows a number of cutaneous
neurofibromas on the neck and trunk.
Fig. 2. Endoscopy upon admission reveals a small ulcer (3×7 mm) in the duodenal bulb with visible vessel.
fibromatosis type 1, and most involve the aorta and its main branches.7,8 The renal artery is most frequently affected, usually resulting in secondary hypertension, particularly in young patients.8 Complications of vascular involvement in- clude aneurismal dilation, arteriovenous fistula, arterio- venous malformations, vascular stenosis, and rupture.9 Among such vasculopathies, vascular aneurysms are most common.7 Several cases of aneurysms or pseudoaneurysms of visceral arteries in type 1 neurofibromatosis patients have been reported, with involved arteries including the inter- costal, extracranial, internal pudendal and gastrointestinal arteries.10-13 However, there are no reports regarding gastro- duodenal artery aneurysms associated with neurofibro- matosis type 1.
We experienced a case of life-threatening duodenal ulcer bleeding resulting from a ruptured gastroduodenal artery aneurysm associated with neurofibromatosis type 1. We treated our patient by transarterial embolization (TAE) after initial endoscopic hemostasis. To the best of our knowledge, this is the first case of duodenal ulcer bleeding from a rup- tured gastroduodenal artery aneurysm in a patient with neu- rofibromatosis type 1. This case suggests that high levels of suspicion and prompt diagnosis are required to select appro- priate treatment options for such patients, and that the em- bolization of the involved arteries should be an essential treatment over endoscopic hemostasis alone to accomplish primary hemostasis and to prevent rebleeding in such cases.
CASE REPORT
A 43-year-old man visited the emergency department for sudden onset of hematemesis three hours before his visit. He was admitted twice to another hospital for duodenal ulcer bleeding (one month and two years prior) and was managed with endoscopic hemostasis. He had a known history of neu- rofibromatosis, diagnosed 25 years ago. He denied con- sumption of alcohol, tobacco, or any medication. He had a number of cutaneous neurofibromas on his neck and trunk (Fig. 1). Physical examination revealed hyperactive bowel sounds, and the patient complained of mild tenderness on the upper abdomen without any rebound tenderness. There were no signs of ulcer perforation or peritonitis. Upon arrival at our hospital, the patient was in a state of shock and had a blood pressure of 70/60 mmHg and a heart rate of 102 beats/min. The patient’s laboratory data on admission in- cluded a white blood cell count of 16,400/mm3, a hemoglo- bin concentration of 8.1 g/dL and a platelet count of 221,000/mm3. Other findings, including a chemical battery, PT, aPTT and electrolytes, were not remarkable. After a large volume of fluid resuscitation, upper gastrointestinal endos- copy was performed to detect the cause of the patient’s gas- trointestinal hemorrhage and for hemostasis. Endoscopy re- vealed a small active ulcer (3×7 mm) with a visible vessel in the stenosed duodenal bulb (Fig. 2). During epinephrine in- jection, pulsatile bleeding began at the injection site. Argon plasma coagulation, injection of additional epinephrine, and
166 임규성 등. 제1형 신경섬유종증에서 발생한 십이지장 궤양 출혈
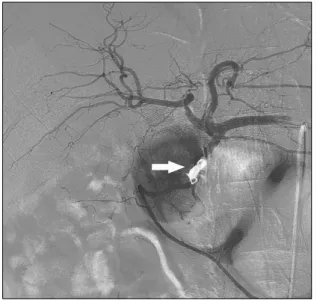
The Korean Journal of Gastroenterology Fig. 3. Selective angiography of the common hepatic artery shows an
aneurysm (arrow) in the mid-portion of the gastroduodenal artery and contrast extravasation into the duodenal lumen before emboli- zation.
Fig. 5. (A) Upper endoscopy 5 days after transarterial embolization reveals an active duodenal ulcer with the metallic coil at the ulcer base. (B) Follow-up endoscopic view 11 days after tran- sarterial embolization shows the ulcer with regenerating epithelium, and the coil material was not visible.
Fig. 4. Postembolization angiography demonstrates successful embolization and cessation of blood flow into the gastroduodenal artery aneurysm with a metallic coil (arrow).
endoscopic hemoclipping were tried and hemostasis was successful. Intravenous pantoprazole (Pacific Pharm., Seoul, Korea) was administered with high-dose continuous in- fusions (i.e., pantoprazole 80 mg bolus followed by 8 mg per hour). On the fourth hospital day, the patient complained of hematemesis and went into hemorrhagic shock that was not responsive to aggressive fluid therapy. Therefore, consider- ing the active re-bleeding from duodenal ulcer, emergency mesenteric angiography was performed to identify and emb- olize the culprit vessel. Before angiography, abdominal com- puted tomography was performed to outline the vascular anatomy, revealing an aneurysm emerging from the gastro- duodenal artery and another aneurysm in the right distal re- nal artery. Subsequent selective angiography of the common hepatic artery showed an aneurysm in the mid-portion of the
gastroduodenal artery and contrast extravasation into the duodenal lumen before embolization (Fig. 3). After selec- tively probing the gastroduodenal artery and aneurysm with a microcatheter, embolization was performed at the distal and proximal segments from the aneurysm using two coils (diameter 6 mm, length 14 cm, NesterⓇ Embolization Micro- coil; Cook Medical, Bloomington, IN, USA) (Fig. 4). These con- secutive procedures produced immediate cessation of ra- dio-contrast extravasation and there were no immediate complications. Upper endoscopy five days after TAE revealed the active duodenal ulcer with the metallic coil at the ulcer base (Fig. 5A), and 11 days after TAE a follow-up endoscopic view showed the ulcer with regenerating epithelium, and the coil material was not visible (Fig. 5B). There were no stigmata of recent bleeding observed on these sequential endoscopic examinations. During first follow-up endoscopy, gastric mu-
Im KS, et al. Duodenal Ulcer Bleeding in Neurofibromatosis Type 1 167
Vol. 66 No. 3, September 2015
cosal biopsies were performed for rapid urease tests and Giemsa staining for the identification of Helicobacter pylori.
The patient received antibiotics therapy for H. pylori erad- ication due to positive results of the Giemsa staining and the intravenous proton pump inhibitor was changed to an oral agent. He was discharged in good condition on the 18th day of hospitalization. The patient remained asymptomatic and showed no recurrent duodenal ulcer bleeding for nine months after the TAE.
DISCUSSION
Technical advances in endoscopic hemostasis enable ef- fective gastrointestinal bleeding control in most patients.
However, endovascular management and surgery may prove necessary after failed endoscopic management for intract- able gastrointestinal bleeding, as in our case. Upper gastro- intestinal bleeding (UGIB) can be caused by a number of pathologies. Aneurysms of the gastroduodenal artery are rare causes of UGIB. If UGIB associated with a gastroduo- denal artery aneurysm occurs, the massive bleeding can be catastrophic. Therefore, early recognition and prompt treat- ment are crucial in UGIB patients suspected to have gastro- duodenal artery aneurysms.14 A literature review of visceral aneurysm cases performed by Moore et al.15 found that 35%
of gastroduodenal artery aneurysms are already ruptured at presentation, with an associated mortality rate of 21%. The most common clinical event associated with ruptured gastro- duodenal artery aneurysms is UGIB, which occurs in 50% of patients, with retroperitoneal and intraperitoneal bleeding occurring less frequently.15
To the best of our knowledge, this is the first case of duode- nal ulcer bleeding resulting from a ruptured gastroduodenal artery aneurysm in a patient with neurofibromatosis type 1.
This case suggests that a high level of suspicion for aneur- ysmal rupture bleeding is needed to select appropriate treat- ment options for such patients, and that embolization of the involved arteries should be considered an essential treat- ment over endoscopic hemostasis alone to prevent recurrent bleeding in such cases.
REFERENCES
1. Friedman JM. Epidemiology of neurofibromatosis type 1. Am J Med Genet 1999;89:1-6.
2. Riccardi VM. Neurofibromatosis: past, present, and future. N Engl J Med 1991;324:1283-1285.
3. Hamilton SJ, Friedman JM. Insights into the pathogenesis of neurofibromatosis 1 vasculopathy. Clin Genet 2000;58:341- 344.
4. Li F, Munchhof AM, White HA, et al. Neurofibromin is a novel regu- lator of RAS-induced signals in primary vascular smooth muscle cells. Hum Mol Genet 2006;15:1921-1930.
5. Norton KK, Xu J, Gutmann DH. Expression of the neuro- fibromatosis I gene product, neurofibromin, in blood vessel en- dothelial cells and smooth muscle. Neurobiol Dis 1995;2:13- 21.
6. Viskochil D. Genetics of neurofibromatosis 1 and the NF1 gene.
J Child Neurol 2002;17:562-570; discussion 571-572, 646-651.
7. Dominguez J, Sancho C, Escalante E, Morera JR, Moya JA, Bernat R. Percutaneous treatment of a ruptured intercostal aneurysm presenting as massive hemothorax in a patient with type I neurofibromatosis. J Thorac Cardiovasc Surg 2002;124:1230- 1232.
8. Salyer WR, Salyer DC. The vascular lesions of neurofibro- matosis. Angiology 1974;25:510-519.
9. Brasfield RD, Das Gupta TK. Von Recklinghausen's disease: a clinicopathological study. Ann Surg 1972;175:86-104.
10. Kipfer B, Lardinois D, Triller J, Carrel T. Embolization of a ruptured intercostal artery aneurysm in type I neurofibromatosis. Eur J Cardiothorac Surg 2001;19:721-723.
11. Mendonça CT, Weingartner J, de Carvalho CA, Costa DS.
Endovascular treatment of contained rupture of a superior mes- enteric artery aneurysm resulting from neurofibromatosis type I. J Vasc Surg 2010;51:461-464.
12. Tsutsumi M, Kazekawa K, Tanaka A, et al. Rapid expansion of be- nign scalp neurofibroma caused by massive intratumoral hemor- rhage: case report. Neurol Med Chir (Tokyo) 2002;42:338-340.
13. Zhang CW, Yang ZG, Xie XD, Wang CH, You C, Li W. Transcatheter embolization of a ruptured internal pudendal artery pseudoa- neurysm in a patient with neurofibromatosis type 1. J Korean Med Sci 2010;25:638-640.
14. Lee CH, Lan CC, Wang CC, Chan CY, Wu YK. Spontaneous rupture of gastroduodenal artery pseudoaneurysm following vigorous cough. Am J Gastroenterol 2009;104:529-530.
15. Moore E, Matthews MR, Minion DJ, et al. Surgical management of peripancreatic arterial aneurysms. J Vasc Surg 2004;40:247- 253.